


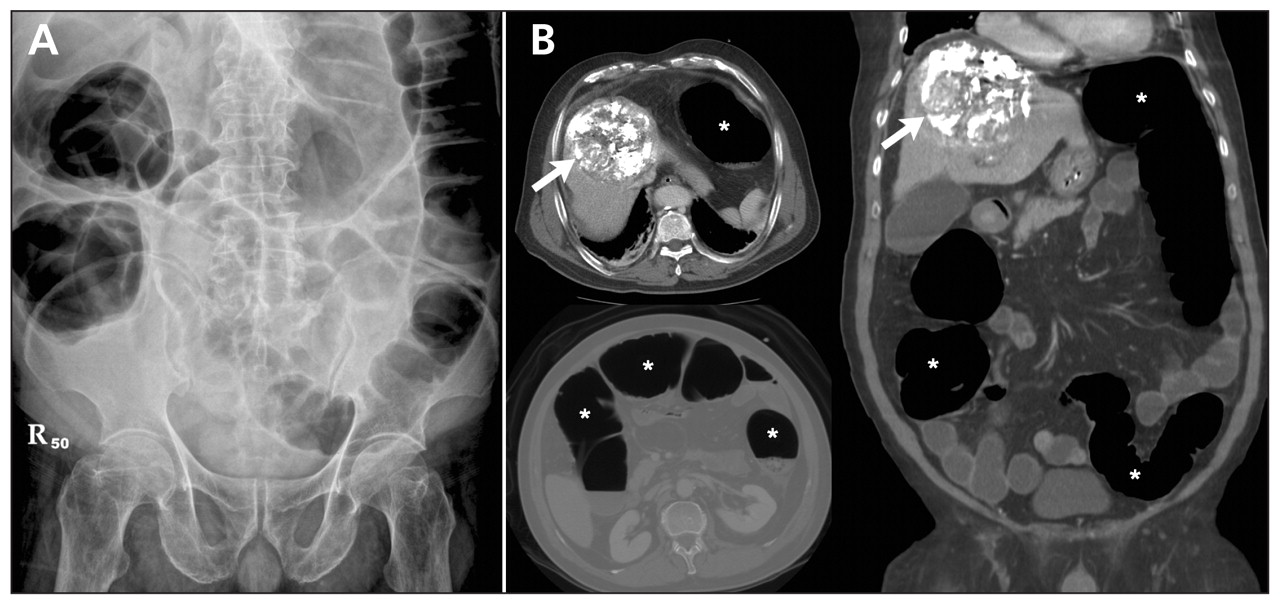
A 76-year-old man with a history of hepatitis C infection and newly diagnosed hepatocellular carcinoma was admitted for scheduled transcatheter arterial chemoembolization therapy. He developed abdominal discomfort and nausea one day after the procedure. On examination, he had a distended abdomen, diffuse tenderness without rebound pain and reduced bowel sounds. He was afebrile, and results of blood tests were unremarkable. Plain abdominal radiography showed diffuse bowel loop dilation (Figure 1A), and computed tomography showed marked bowel loop dilation and colonic gas, without obstructive masses or ischemic bowel lesions (Figure 1B).

(A) Plain abdominal radiograph of a 76-year-old man with abdominal discomfort after transcatheter arterial chemoembolization therapy for hepatocellular carcinoma, showing diffuse bowel loop dilation. (B) Computed tomographic scan in axial and coronal planes showing diffuse dilation of the bowels, especially the colon (*). The maximal colonic diameter was 8.8 cm. Note the embolized hepatocelluar carcinoma (arrows).
We diagnosed acute pseudo-obstruction of the colon (Ogilvie syndrome). Nasogastric decompression and discontinuation of oral intake did not relieve our patient’s abdominal pain. He developed dyspnea because of persistent abdominal distention, and we decided to use colonoscopic decompression followed by neostigmine. He recovered fully from the syndrome and received treatment for hepatocellular carcinoma.
Ogilvie syndrome is marked by nonmechanical dilation of the cecum and right colon.1 It presents with abdominal pain and abnormal intestinal motility, and is not uncommon in patients with critical illnesses, electrolyte imbalances, anticholinergic medication regimens and recent surgery. In our patient, we believe the syndrome was related to transcatheter arterial chemoembolization therapy. The exact pathogenesis of the syndrome remains unclear, although imbalance of the autonomic nervous system affecting the colon has been proposed.2
Unlike toxic megacolon (often caused by inflammatory bowel disease or infection), Ogilvie syndrome usually does not present with signs of systemic toxicity. Computed tomography is usually indicated for ruling out obstructive lesions or possible bowel ischemia. If the syndrome is left untreated, life-threatening complications such as bowel ischemia or perforation may occur in an estimated 3%–15% of patients, with a 50% reported mortality rate.2 The success rate for nasogastric decompression with or without anal tube placement is variable (20%–92%), and colonoscopic decompression is successful in about 70% of patients.2 A resolution rate of 80%–90% has been reported for use of neostigmine (2.0 mg intravenously) when conservative therapy has failed.2 Surgical management with cecostomy or colectomy is reserved for refractory cases.
Footnotes
-
This article has been peer reviewed.
-
Competing interests: None declared.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles

