


Abstract
Background: Risk factors for type 2 diabetes remain poorly characterized among Aboriginal Canadians. We aimed to determine the incidence of type 2 diabetes in an Aboriginal community and to evaluate prospective associations with metabolic syndrome and its components.
Methods: Of 606 participants in the Sandy Lake Health and Diabetes Project from 1993 to 1995 who were free of diabetes at baseline, 540 (89.1%) participated in 10-year follow-up assessments. Baseline anthropometry, blood pressure, fasting insulin and serum lipid levels were measured. Fasting and 2-hour postload glucose levels were obtained at follow-up to determine incident cases of type 2 diabetes.
Results: The 10-year cumulative incidence of diabetes was 17.5%. High adiposity, dyslipidemia, hyperglycemia, hyperinsulinemia and hypertension at baseline were associated with an increased risk of diabetes after adjustment for age and sex (all p ≤ 0.03). Metabolic syndrome had high specificity (75%–88%) and high negative predictive value (85%–87%) to correctly detect diabetes-free individuals at follow-up. It had low sensitivity (26%–48%) and low positive predictive value (29%–32%) to detect future diabetes. Metabolic syndrome at baseline was associated with incident diabetes after adjustment for age and sex, regardless of whether the syndrome was defined using the National Cholesterol Education Program criteria (odds ratio [OR] 2.03, 95% confidence interval [CI] 1.10–3.75) or the International Diabetes Federation criteria (OR 2.14, 95% CI 1.29–3.55). The association was to the same degree as that for impaired glucose tolerance assessed using the oral glucose tolerance test (OR 2.87, 95% CI 1.52–5.40; p > 0.05 for comparison of C statistics).
Interpretation: Metabolic syndrome and its components can be identified with readily available clinical measures. As such, the syndrome may be useful for identifying individuals at risk of type 2 diabetes in remote Aboriginal communities.
Type 2 diabetes mellitus has become an epidemic, particularly among Aboriginal Canadians, who have a prevalence of the disease 3–5 times higher than non-Aboriginal Canadians.1 Although no cure exists for diabetes, the disease and its complications can be prevented, delayed and managed by identifying risk factors and detecting the condition at an early stage. Traditional risk factors for diabetes include obesity, dyslipidemia, hyperglycemia and hypertension.2 The clustering of these metabolic abnormalities has long been recognized and is now commonly termed metabolic syndrome.3–5 Although the clinical application and practicality of the syndrome continue to be debated,6,7 a number of studies have associated the syndrome with increased risk of diabetes8–10 and cardiovascular disease.8,9
Previous cross-sectional studies have indicated a high prevalence of risk factors for diabetes, including obesity, impaired glucose tolerance and metabolic syndrome, among Aboriginal Canadians.1,11–13 Recent studies have reported on diabetes incidence in this population using data from an administrative database14 and a hospital registry.15 No study to date has determined the incidence of diabetes using detailed individual assessments, nor has there been any prospective population-based study of metabolic risk factors for diabetes onset among Aboriginal Canadians.
The identification of impaired glucose tolerance, at which stage intervention strategies are often initiated, requires a 2-hour oral glucose tolerance test. Because such a test may not be easily applied in community settings, especially in remote Aboriginal communities, the use of routinely measured clinical variables to detect individuals at high risk of diabetes would offer a practical alternative. Metabolic syndrome has been identified to offer this potential in other populations.8–10 However, its role has not been assessed in Aboriginal Canadians, who have experienced a rapid epidemiologic transition in conjunction with a unique genetic susceptibility to diabetes.1,16
We conducted this study to determine the incidence of type 2 diabetes in an Aboriginal community and to evaluate prospective associations between readily available clinical variables and diabetes.
Methods
Study design
The Sandy Lake Health and Diabetes Project is a population-based cohort study designed to determine the incidence of diabetes and its associated risk factors in an Aboriginal Canadian population. The project has been described in detail previously.11,17 Between 1993 and 1995, baseline data were obtained from 728 (71.5%) of 1018 eligible residents of Sandy Lake First Nation aged 10–79 years. Informed consent was obtained from all participants. The study was approved by the Sandy Lake First Nation Band Council and the University of Toronto Ethics Review Committee.
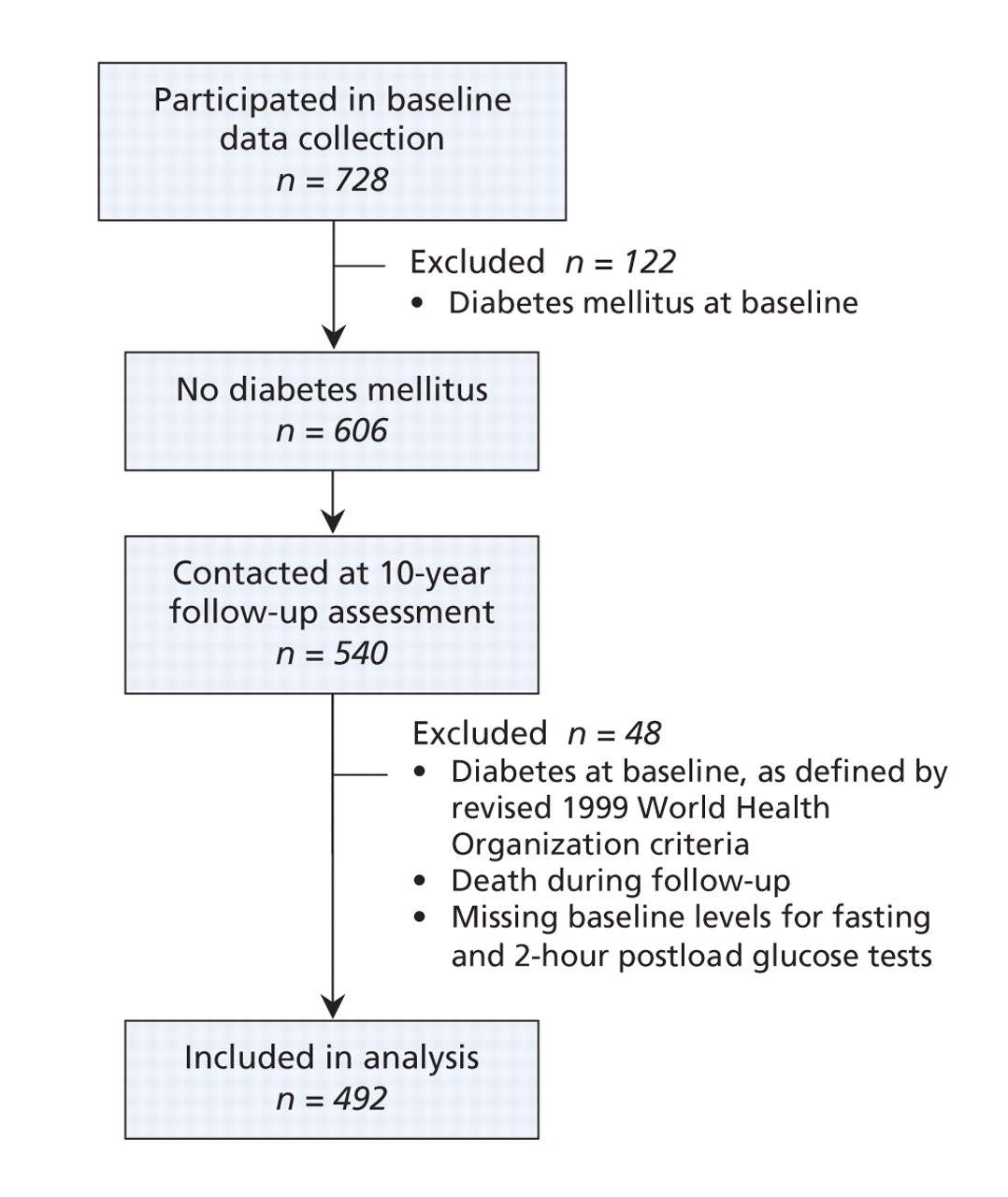
Between 2003 and 2005, 540 (89.1%) of 606 participants who were free of diabetes at baseline participated in 10-year follow-up assessments. They were slightly older than the 66 who did not return for follow-up but otherwise were similar in terms of sex and body mass index. During follow-up, 27 (5.0%) of the 540 participants died because of cancer (n = 6), pneumonia (n = 5), cirrhosis of the liver (n = 3), cardiovascular disease (n = 2), brain tumour or aneurysm (n = 2), suicide (n = 2) and other causes (n = 7). In the present analysis, we excluded participants who died during follow-up, who had missing results of baseline fasting and 2-hour postload glucose tests, or who had diabetes at baseline as defined by the revised diagnostic criteria of the World Health Organization.18 This left 492 men and women for inclusion in our study (Figure 1).

Figure 1: Eligibility and participation in the Sandy Lake Health and Diabetes Project follow-up study.
Baseline data collection and laboratory procedures
At baseline, blood samples were collected after an 8- to 12-hour overnight fast to determine each participant's glucose, insulin and lipid profile. A 75-g oral glucose tolerance test was administered, after which a second blood sample was drawn for glucose measurement.
Details of the baseline biochemical analyses have been described previously.11 In brief, the glucose level was determined by means of the glucose oxidase method. The fasting plasma insulin level was analyzed by means of a radioimmunoassay (Pharmacia, Piscataway, USA). Levels of triglycerides, high-density lipoprotein (HDL) cholesterol and low-density lipoprotein (LDL) cholesterol were determined using standard methods described in the Lipid Research Clinics manual of operations.19
Each anthropometric measurement and blood pressure reading was taken twice; we used the average in the analyses.17 Height was measured with an Accustat wall-mounted stadiometer (Genentech Inc., San Francisco, USA) and weight with a hospital beam scale (Health-o-Meter Inc., Bridgeview, USA). Waist circumference was measured at the iliac crest using an inelastic tape. Percent body fat was estimated by means of bioelectrical impedance analysis (Tanita TBF-201 Body Fat Analyzer, Tanita Corp., Tokyo, Japan). Blood pressure was recorded with the participant seated.
The participants' medical history and their family history of diabetes were obtained by means of an interviewer-administered questionnaire. Participants were considered to have a family history of diabetes if one or both biological parents had diabetes.17
Definition of incident type 2 diabetes
Incident diabetes was defined as the presence of any of the following at follow-up assessments: (a) a fasting plasma glucose level of 7.0 mmol/L or greater, or a 2-hour postload plasma glucose level of 11.1 mmol/L or greater on an oral glucose tolerance test; (b) current use of insulin or oral hypoglycemic agents; or (c) a positive response to the question Have you ever been diagnosed with diabetes by a nurse (practitioner) or a doctor? Among the 492 participants, follow-up blood samples were collected from 383 (77.8%). The diabetes status of the remaining 109 (22.2%) participants was ascertained on the basis of a self-reported clinical diagnosis of diabetes through a phone interview.
Definitions of metabolic syndrome
We determined whether participants had metabolic syndrome according to 2 definitions of the syndrome: that of the National Cholesterol Education Program3 and that of the International Diabetes Federation.4,5
According to the National Cholesterol Education Program definition,3 we considered participants to have metabolic syndrome if they met 3 or more of the following criteria: abdominal obesity (waist circumference > 102 cm in men and > 88 cm in women); high triglyceride level (≥ 1.7 mmol/L); low HDL cholesterol level (< 1.03 mmol/L in men and < 1.29 mmol/L in women); hypertension (systolic pressure ≥ 130 mm Hg, diastolic pressure ≥ 85 mm Hg, or use of antihypertensive drug therapy); or high fasting plasma glucose level (≥ 6.1 mmol/L).
The International Diabetes Federation defines metabolic syndrome using age-specific criteria.4,5 According to this definition, participants aged 16 years or more were considered to have metabolic syndrome if they had central obesity (waist circumference ≥ 94 cm in men and ≥ 80 cm in women [we used European cut-off points given the absence of cut-off points for Aboriginal populations]) in addition to any 2 of the following criteria: high triglyceride level (≥ 1.7 mmol/L); low HDL cholesterol level (< 1.03 mmol/L in men and < 1.29 mmol/L in women); hypertension (systolic blood pressure ≥ 130 mm Hg, diastolic blood pressure ≥ 85 mm Hg or use of antihypertensive drug therapy); or high fasting plasma glucose level (≥ 5.6 mmol/L).4 For participants aged 10–15 years, the International Diabetes Federation criteria are the same as those for adults, except that central obesity is defined as a waist circumference in the 90th percentile or higher (as assessed by the Third National Health and Nutrition Examination Survey [NHANES III] waist circumference percentile regression for European-American children20) and the cut-off for HDL cholesterol is 1.03 mmol/L for both boys and girls.5
Statistical analysis
We assessed distributions of continuous variables for normality; we used natural log-transformations of skewed variables in descriptive statistical analyses. Descriptive statistics for continuous variables are summarized as means and standard deviations, or as medians and interquartile ranges for variables with a skewed distribution. Categorical variables are summarized as proportions. We compared baseline characteristics of participants with and without incident diabetes using Welch's modified t test or the χ2 test as appropriate.
We conducted multivariable logistic regression analysis to evaluate the association of clinical variables with incident diabetes. The clinical variables were body mass index, percent body fat, waist circumference, waist-to-height ratio, systolic and diastolic blood pressures, hypertension, HDL cholesterol, LDL cholesterol and triglyceride levels, fasting plasma glucose and 2-hour postload glucose levels, fasting insulin level and current smoking status. Each clinical variable was individually assessed in 2 models: model 1 adjusted for age and sex, and model 2 adjusted for model 1 variables in addition to individual components of metabolic syndrome (i.e., International Diabetes Federation criteria for waist circumference, triglycerides, HDL cholesterol, blood pressure and fasting plasma glucose, excluding the main effect). We calculated odds ratios (ORs) and 95% confidence intervals (CIs). We assessed sex interactions with independent variables by adding an interaction term into a model adjusted for model 2 variables in addition to the main effect.
We calculated the sensitivity, specificity, positive predictive value and negative predictive value to assess the ability of baseline impaired glucose tolerance status to detect incident diabetes after adjustment for age and sex. We performed the same diagnostic tests to assess the ability of metabolic syndrome and its components, using each definition. We used age- and sex-adjusted logistic regression analysis to evaluate the association between metabolic syndrome (each definition) and incident diabetes, and between impaired glucose tolerance and incident diabetes. To compare different logistic models in their capability to discriminate participants with and without incident diabetes, we calculated C statistics, which are analogous to the area under the receiver-operating-characteristic curve; we determined significance using the DeLong algorithm.21
Results
The baseline characteristics of the participants with and without incident diabetes at 10-year follow-up are presented in Table 1. Of the 492 participants included in our analysis, 86 (17.5%) were found to have diabetes at follow-up. Diabetes was ascertained on the basis of fasting or 2-hour postload glucose levels, or both, in 72 (18.8%) of 383 participants. For 14 (12.8%) of 109 participants without follow-up blood samples, diabetes was ascertained on the basis of self-reported clinical diagnosis only. Compared with participants who had follow-up blood samples, those without samples were younger (p = 0.009) but were not different in terms of sex or body mass index (each p ≥ 0.05). When only self-report was considered for ascertainment of incident diabetes among participants with follow-up blood samples, 53 (13.8%) of 383 had diabetes.
Table 1.
The incidence of diabetes increased with age (p < 0.001). It was 10.5% among participants aged 10–19 years, 15.1% among those aged 20–29 years, 27.3% among those 30–39 years, 43.3% among those 40–49 years and 18.9% among those aged 50 and older.
Compared with individuals who did not have diabetes at the 10-year follow-up, those who did have incident diabetes had a higher body mass index, percent body fat, waist circumference and waist-to-height ratio at baseline (each p < 0.001). They also had a lower baseline HDL cholesterol level (p = 0.02) and higher baseline LDL cholesterol, triglyceride, fasting plasma glucose, 2-hour postload glucose and fasting insulin levels, and higher baseline systolic and diastolic blood pressures (each p < 0.001). Participants with incident diabetes were also more likely than those without diabetes to have had hypertension, impaired glucose tolerance and metabolic syndrome at baseline (each p ≤ 0.001) (Table 1).
In the multiple logistic regression analysis, we found that the following clinical variables at baseline were significantly associated with an increased risk of incident diabetes in the age- and sex-adjusted models: high body mass index, percent body fat, waist circumference, waist-to-height ratio; high fasting plasma glucose, 2-hour postload glucose and fasting insulin levels; high systolic and diastolic blood pressures; high LDL cholesterol and triglyceride levels; a low HDL cholesterol level; and hypertension (each p ≤ 0.03) (Figure 2).

Figure 2: Age- and sex-adjusted risk of type 2 diabetes associated with readily accessible clinical measurements.
When we adjusted the models further for individual components of metabolic syndrome, excluding the main effect, we found that the direction of the associations of clinical variables with incident diabetes remained the same (data not shown), except for certain variables that were no longer significantly associated with incident diabetes. These variables were systolic blood pressure (OR 1.18, 95% CI 0.98–1.41), HDL cholesterol (OR 0.51, 95% CI 0.18–1.44), LDL cholesterol (OR 1.24, 95% CI 0.84–1.84) and fasting insulin level (OR 1.05, 95% CI 0.99–1.12). Active smoking was not independently associated with incident diabetes in model 1 (Figure 2) or model 2 (data not shown). There were no statistically significant sex interactions with clinical variables in predicting incident diabetes (all interactions p ≥ 0.05), except with baseline fasting plasma glucose level (p = 0.03) (data not shown). When we stratified data by sex, we found a significant association between fasting plasma glucose level and incident diabetes among males after adjustment for components of metabolic syndrome (OR 2.05, 95% CI 1.31–3.19). This was not the case among females (OR 1.06, 95% CI 0.76–1.48).
When we assessed the diagnostic performance of impaired glucose tolerance at baseline in predicting incident diabetes, we found that it had high specificity (91%) and high negative predictive value (85%), yet low sensitivity and low positive predictive value (Table 2). We found similar performance results for metabolic syndrome regardless of which set of defining criteria were used; however, we observed a slightly lower specificity and higher sensitivity for the syndrome as defined by the International Diabetes Federation criteria (Table 2). For the individual components of metabolic syndrome, we found that, in general, the specificity and negative predictive values were within a moderate to high range, and the sensitivity and positive predictive values were low (Table 2). As an exception, waist circumference as defined by the International Diabetes Federation had a high sensitivity and negative predictive value but a low specificity and positive predictive value (Table 2).
Table 2.
We found that metabolic syndrome at baseline was associated with incident diabetes after adjustment for age and sex regardless of whether we used the National Cholesterol Education Program definition (OR 2.03, 95% CI 1.10–3.75) or the International Diabetes Federation definition (OR 2.14, 95% CI 1.29–3.55) (Figure 3). There was no significant difference between the 2 definitions in their ability to discriminate participants with incident diabetes from those who did not have diabetes (p ≥ 0.05 for comparison of C statistics).

Figure 3: Age- and sex-adjusted risk of type 2 diabetes associated with impaired glucose tolerance and with metabolic syndrome. C statistics for metabolic syndrome, whether defined by the National Cholesterol Education Program criteria (0.668) or the International Diabetes Federation criteria (0.682), were not significantly different from the C statistic for impaired glucose tolerance (0.681) (p > 0.05 for comparisons of C statistics).
When we lowered the fasting plasma glucose cut-off to 5.6 mmol/L or greater in the National Cholesterol Education Program criteria, we found that the modified definition of metabolic syndrome was significantly associated with incident diabetes to the same degree as the original definition (p = 0.54 for comparison of C statistics) and as the International Diabetes Federation definition (Appendices 1 and 2, available at www.cmaj.ca/cgi/content/full/180/6/617/DC2). The age- and sex-adjusted model for impaired glucose tolerance (C statistic 0.681) was not better at detecting future diabetes than the metabolic syndrome models, whether defined by the National Cholesterol Education Program criteria (C statistic 0.668) or the International Diabetes Federation criteria (C statistic 0.682) (comparison of C statistics: p = 0.57 for the National Cholesterol Education Program definition v. impaired glucose tolerance, and p = 0.96 for the International Diabetes Foundation definition v. impaired glucose tolerance) (Figure 3). In addition, the capability of individual components of the metabolic syndrome (i.e., waist circumference, triglyceride level, HDL cholesterol level, blood pressure or fasting plasma glucose level) did not differ significantly from the capability of impaired glucose tolerance in predicting incident diabetes (each p ≥ 0.05 for comparison of C statistics) (Appendices 3 and 4, available at www.cmaj.ca/cgi/content/full/180/6/617/DC2).
Interpretation
In this prospective study, we documented that the 10-year cumulative incidence of type 2 diabetes was 17.5% in the Aboriginal study population. We also noted that the incidence increased with age, from 10.5% among participants 10–19 years old, to 43.3% among those 40–49 years. High adiposity, dyslipidemia, hyperglycemia, hyperinsulinemia and hypertension at baseline were associated with increased risk of diabetes after adjustment for age and sex. Although metabolic syndrome at baseline had low sensitivity and low positive predictive value for detecting future diabetes, it had high specificity and high negative predictive value for correctly identifying disease-free individuals at follow-up. In addition, metabolic syndrome at baseline was associated with incident diabetes to the same degree that impaired glucose tolerance was.
Similar observations were reported in the Strong Heart Study, a cohort study that followed Aboriginal North Americans aged 45–74 years with a high prevalence of diabetes and metabolic syndrome.10,22–24 In that study, the incidence of diabetes over a follow-up period of about 8 years was 17.0%. The risk of diabetes was higher among those with metabolic syndrome than among those without the syndrome.10
Our results confirmed that traditional risk factors documented in non-Aboriginal populations, including obesity, dyslipidemia, hyperglycemia and hypertension,2 were associated with increased risk of diabetes in this Aboriginal population with unique genetic susceptibility to diabetes.16 There were no significant sex interactions with these traditional risk factors in predicting diabetes, except for fasting plasma glucose level at baseline. When we stratified data by sex, we found a significant association between fasting plasma glucose level and incident diabetes among males, but not among females. This difference may have been influenced by sex differences in other baseline characteristics: a higher number of females in the study population had obesity at baseline,11,12 which has a greater impact on 2-hour postload glucose levels and impaired glucose tolerance than on fasting plasma glucose levels.25
Randomized controlled trials have previously shown that lifestyle interventions, including physical activity and dietary modification, reduce the incidence of diabetes among participants with impaired glucose tolerance at baseline.26–28 However, impaired glucose tolerance is determined by means of a 2-hour oral glucose tolerance test, which often is not accessible or easy to perform in community settings. Stern and colleagues29 demonstrated that a multivariable model including routinely obtained clinical variables (i.e., age, sex, ethnicity, fasting plastma glucose level, systolic blood pressure, HDL cholesterol level, body mass index and family history of diabetes) was better than the oral glucose tolerance test alone in identifying individuals at high risk of diabetes (p < 0.001). They also found that a multivariable model including lipid levels, blood pressure, body mass index, smoking history and family history of cardiovascular disease was better than the oral glucose tolerance test alone in detecting individuals at high risk of cardiovascular disease.30
A number of studies have shown an association between metabolic syndrome, defined using common clinical measurements, and increased risk of diabetes8–10 and cardiovascular disease.8,9 Our findings are consistent with this literature and offer the potential to use metabolic syndrome in identifying individuals at increased risk of diabetes and possibly cardiovascular disease in remote community settings. This potential is of particular interest to Aboriginal communities with a high prevalence of diabetes1,11 and evidence of increasing rates of hospital admission because of cardiovascular disease.12,31
The Diabetes Prevention Program randomized trial showed that intensive lifestyle intervention and metformin therapy can reduce the incidence of metabolic syndrome and also the prevalence of metabolic syndrome at follow-up.32 Other randomized controlled trials have confirmed that lifestyle intervention can reduce the prevalence of metabolic syndrome.33,34 Therefore, implementing intervention strategies for individuals with the syndrome may be a practical solution to prevent, or at least to delay, the onset of diabetes in Aboriginal communities.
Limitations
Limitations of our study include challenges of conducting investigations in a remote community. Specifically, we were unable to collect interim data to analyze the time to onset of diabetes. Also, we were unable to obtain follow-up blood samples from all of the participants: for 109 (22.2%), the assessments of diabetes outcomes were by self-reported clinical diagnosis only. This may have caused underreporting of incident diabetes. Nevertheless, we were able to retain a high 10-year follow-up rate of 89.1% (540/606).
Conclusion
The presence of metabolic syndrome at baseline was associated with incident diabetes to the same degree that impaired glucose tolerance was, although not all individuals with the syndrome had incident diabetes. The absence of the syndrome at baseline was likely to identify individuals free of incident diabetes correctly. Metabolic syndrome is not a diagnostic tool; however, the syndrome and its components may be used to communicate increased risk of diabetes to individuals in remote Aboriginal communities, where the oral glucose tolerance test is not easily accessible.
Our findings are likely applicable to other First Nations populations in Canada, particularly Subarctic Algonquian-speaking peoples, who share a similar historical, cultural and social background as the community in our study.35 However, more studies are needed in other Aboriginal communities and groups, especially among Métis and Inuit populations. Our findings may facilitate the development and promotion of preventive strategies in primary care settings, including lifestyle interventions to reduce long-term risk. They may also assist in reducing the incidence of diabetes in Aboriginal populations by influencing future public health initiatives.
@@ See related commentary by Reaven, page 601
Footnotes
-
Funding: This work was supported by grants from the Canadian Institutes of Health Research (CIHR). Sylvia Ley is supported by a University of Toronto Banting and Best Diabetes Centre Novo Nordisk Studentship. Stewart Harris holds the Canadian Diabetes Association Chair in Diabetes Management and the Ian McWhinney Chair in Family Medicine at the University of Western Ontario. Bernard Zinman holds the Sam and Judy Pencer Family Chair in Diabetes Research at Mount Sinai Hospital and University of Toronto. Anthony Hanley holds the CIHR Canada Research Chair in the Epidemiology of Type 2 Diabetes and is supported by the Ontario Ministry of Research and Innovation Early Researcher Award.
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/180/6/617/DC1
This article has been peer reviewed.
Contributors: Sylvia Ley contributed to the analysis and interpretation of the data and drafted the manuscript. Stewart Harris, Joel Gittelsohn, Thomas Wolever, Philip Connelly, Robert Hegele, Bernard Zinman and Anthony Hanley contributed to the conception and design of the study and revised the manuscript critically for important intellectual content. Mary Mamakeesick, Tina Noon and Edith Fiddler contributed to the acquisition of data and revised the manuscript critically for important intellectual content. All of the authors approved the final version submitted for publication.
Acknowledgement: We are indebted to the leadership and community members of Sandy Lake First Nation for their enthusiastic partnership and participation in this project.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Prevalence of metabolic syndrome and diabetes mellitus in Sami and Norwegian populations. The SAMINOR--a cross-sectional study
- Association of Apolipoprotein B with Incident Type 2 Diabetes in an Aboriginal Canadian Population
- Is diagnosing metabolic syndrome a uniquely simple way to predict incident type 2 diabetes mellitus?
More in this TOC Section
Similar Articles
Collections

