


- © 2007 Canadian Medical Association
Abstract
Background: The health care system in Canada provides essential health services to all women irrespective of socioeconomic status. Our objective was to determine whether perinatal and infant outcomes varied by family income and other socioeconomic factors in this setting.
Methods: We included all 92 914 women who delivered in Nova Scotia between 1988 and 1995 following a singleton pregnancy. Family income was obtained for 76 440 of these women through a confidential link to income tax records and was divided into 5 groups. Outcomes studied included pregnancy complications, preterm birth, small-for-gestational-age live birth, perinatal death, serious neonatal morbidity, postneonatal death and infant death. Logistic regression models were used to adjust for potential confounders.
Results: Compared with women in the highest family income group, those in the lowest income group had significantly higher rates of gestational diabetes (crude rate ratio [RR] 1.44, 95% confidence interval [CI] 1.21–1.73), preterm birth (crude RR 1.20, 95% CI 1.06–1.35), small-for-gestational-age live birth (crude RR 1.81, 95% CI 1.66–1.97) and postneonatal death (crude RR 5.54, 95% CI 2.21–13.9). The opposite was true for rates of perinatal death (crude RR 0.74, 95% CI 0.56–0.96), and there was no significant difference between the 2 groups in the composite of perinatal death or serious neonatal morbidity (crude RR 1.01, 95% CI 0.82–1.24). Adjustment for behavioural and lifestyle factors accentuated or attenuated socioeconomic differences.
Interpretation: Lower family income is associated with increased rates of gestational diabetes, small-for-gestational-age live birth and postneonatal death despite health care services being widely available at no out-of-pocket expense.
Socioeconomic factors can have profound effects on the health of individuals and populations, and the perinatal domain is particularly susceptible to such influences. The principal pathways by which socioeconomic status affects perinatal health include those that operate through lifestyle and behavioural factors: a large fraction of socioeconomic differences in adverse perinatal outcomes can be explained on the basis of factors such as maternal age,1,2 smoking,3,4 marital status,5,6 alcohol consumption,7 obesity,8,9 residence (rural v. urban),10 education,7,11 weight gain,12 early prenatal care,13 prenatal class attendance, parity and breast-feeding.7
Differential access to good-quality obstetric services and neonatal care is another main reason for socioeconomic disparities in perinatal health. We have previously shown that the system of health care prevalent in Canada provides obstetric, neonatal and related health care services to women regardless of their socioeconomic status.14 In fact, we found that rates of labour induction and cesarean delivery were higher among women from lower income families than among those from higher income families, after controlling for lifestyle and behavioural factors.14 More generally, it has been shown that the introduction of universal access to essential health services in Canada in 196815 led to a decline in regional disparities in infant mortality, whereas such disparities have tended to increase globally.16
We carried out a population-based study to quantify the effects of socioeconomic factors (e.g., family income) on perinatal and infant outcomes in a setting where obstetric, neonatal and related health care services are widely available and provided with no out-of-pocket payments. Whereas other studies have examined this question previously using ecologic measures such as neighbourhood income,17–19 we used highly reliable individual-level information on family income and related measures of socioeconomic status.
Methods
Study design
We included all women residing in Nova Scotia who delivered between 1988 and 1995 following a singleton pregnancy. Information on pregnancy, labour and delivery was obtained from the Nova Scotia Atlee Perinatal Database, a population-based database containing detailed information extracted from antenatal and medical charts by trained personnel using standardized forms. An ongoing data quality-assurance program, which carries out periodic abstraction studies, as well as validation studies20 have shown that the information in the database is reliable. We excluded deliveries involving births at a gestational age of less than 20 weeks or a birth weight of less than 500 g to avoid potential bias due to variations in birth registration.21
Information on family income of the women in the study population and other details regarding their socioeconomic status were obtained through a confidential linkage between the Nova Scotia Atlee Perinatal Database and the federal income tax (T1 Family File) records maintained by the Small Area and Administrative Data Division of Statistics Canada. The T1 Family Files are created from several administrative data sources, the primary source being annual T1 income tax returns.22 The linkage was carried out using a combination of deterministic and probabilistic methods. Linkage was successful for 76 440 (82.3%) of the 92 914 women who had singleton births between 1988 and 1995 in Nova Scotia. All linkages and analyses involving income-related information were carried out by personnel in the Small Area and Administrative Data Division in their highly secure offices, and all identifying information was removed. Tabular analyses involving income or related information that resulted in cells with counts of fewer than 15 were suppressed, and all tabulated counts were rounded to the nearest 10. Regression analyses were carried out without any such restrictions.
Income information regarding each woman's family was obtained for the year in which the delivery occurred. Family income was adjusted for family size (using standard methods23) and inflation, with all income being expressed in 1988 Canadian dollars. Size-and inflation-adjusted family income was categorized into 5 groups (< $7500; $7500–$13 399; $13 400–20 299; $20 300–$29 299 and ≥ $29 300) based on the quintile cut-offs created in a pilot study of linkage feasibility.
Tax-deductible investments to a registered retirement savings plan (RRSP) made in the year of delivery were also examined as an additional measure of socioeconomic status. This measure reflects a dimension not captured by family income (similar to house and car ownership24).
The study was approved by the Dalhousie University Research Ethics Board.
Outcome measures
The outcomes of interest included pregnancy complications such as hypertensive disorders (yes/no for chronic hypertensive disease, severe pregnancy-induced hypertension, HELLP [hemolysis, elevated liver enzymes and low platelet count] syndrome or eclampsia), gestational diabetes (yes/no), pre-existing diabetes mellitus (yes/no), other chronic medical disease (yes/no), placenta previa (yes/no) and placental abruption (yes/no). Fetal and infant outcomes studied included preterm birth (< 37 weeks and < 32 weeks), small-for-gestational-age live birth (< 10th percentile and < 3rd percentile25), perinatal death, composite of perinatal death or serious neonatal morbidity (5-minute Apgar score ≤ 3, severe respiratory distress syndrome requiring assisted ventilation, bronchopulmonary dysplasia, grade 3 or 4 intraventricular hemorrhage, periventricular leukomalacia, severe retinopathy of prematurity or necrotizing enterocolitis), postneonatal death and infant death.
Maternal behavioural and lifestyle factors assessed included maternal age (< 20, 20–24, 25–29, 30–34, 35–39 and ≥ 40 years), parity (0, 1, 2, ≥ 3), marital status (married, common law, single, other), smoking status at delivery (nonsmoker, 1–9 cigarettes per day, ≥ 10 cigarettes per day), prepregnancy weight (< 55, 55–59, 60–69, 70–74 and ≥ 75 kg) and residence in rural area (yes/no based on postal code). Relevant obstetric history, including previous cesarean delivery (yes/no), previous low-birth-weight infant (yes/no) and previous perinatal death (yes/no), were also studied among multiparous women.
Statistical analysis
The relation between socioeconomic status and perinatal outcomes was modelled using logistic regression, with adjustment for behavioural and lifestyle factors and period of delivery (1988–1990, 1991–1992, 1993–1995). Variance estimates were adjusted to account for the potential nonindependence of observations,26 since some women had more than 1 delivery during the study period.
Results
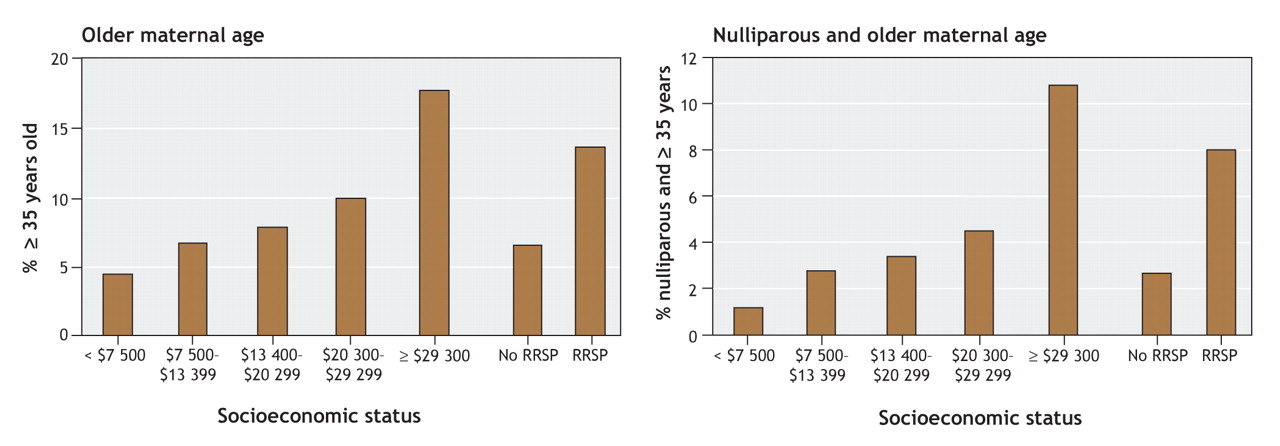
Women in the higher family income groups were more likely than those in the lower income groups to be older (35 years of age or more) at delivery (Figure 1). Differences across family income groups were also evident for behavioural, lifestyle and other factors: women in the lower family income groups were more likely than those in the higher income groups of being smokers (Figure 2) and of having a prepregnancy weight of 75 kg or more (Figure 3). Women with a lower family income were also more likely to be single, reside in a rural area and have an unfavourable obstetric history (Appendix 1, available online at www.cmaj.ca/cgi/content/full/177/6/583/DC2). Such differences were also noted when women were categorized according to their RRSP investment status (Figure 1, Figure 2, Figure 3, and online Appendix 1).
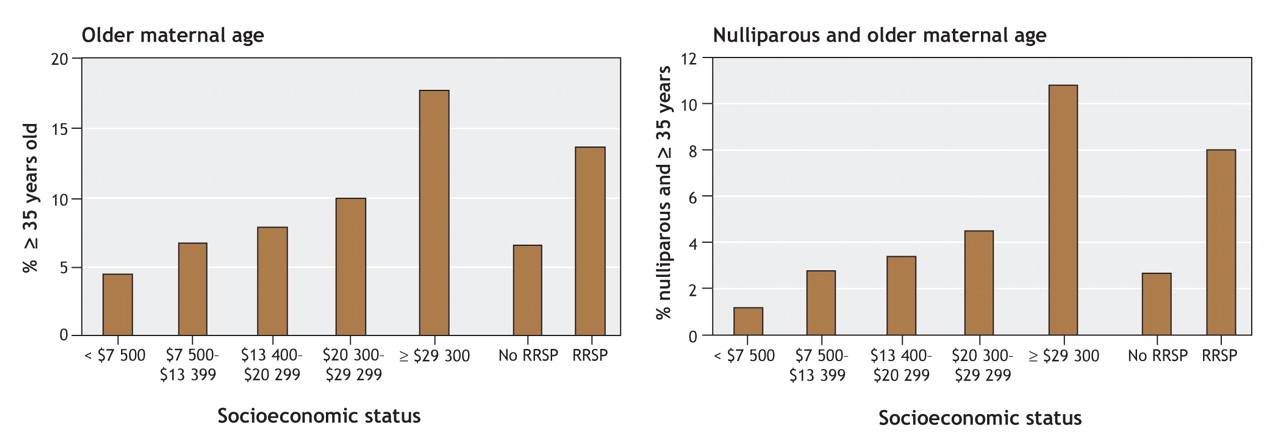
Figure 1: Relation between socioeconomic status (family income and contribution to registered retirement savings plan [RRSP]) and maternal age among women with singleton deliveries in Nova Scotia, 1988–1995. Women in the lower family income groups were less likely than those in the highest income group to be older (35 years of age or more); this observation was true for all women in the study population (left panel) and for those who were nulliparous (right panel).
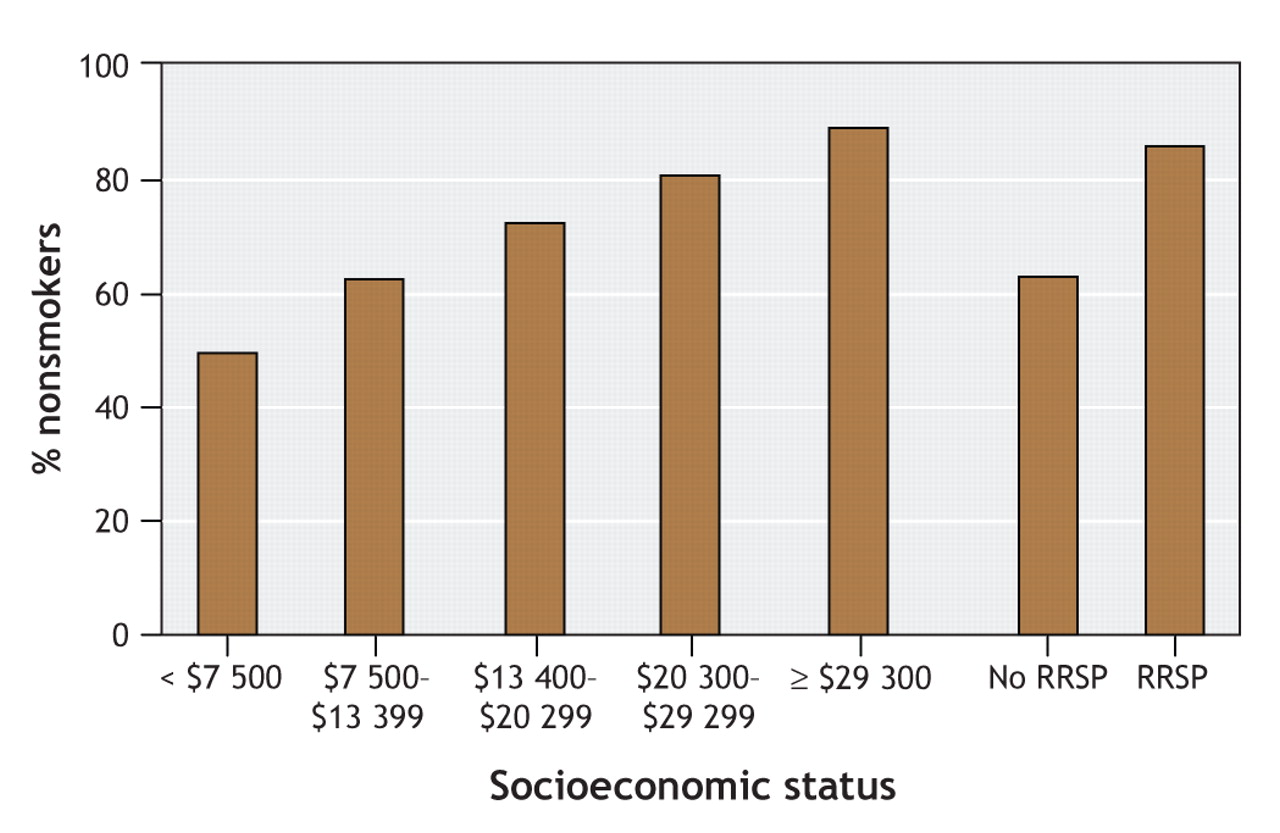
Figure 2: Relation between socioeconomic status (family income and contribution to registered retirement savings plan [RRSP]) and smoking status among women with singleton deliveries in Nova Scotia, 1988–1995. Women in the lower family income groups were less likely than those in the highest income group to be nonsmokers.

Figure 3: Relation between socioeconomic status (family income and contribution to registered retirement savings plan [RRSP]) and maternal weight before pregnancy among women with singleton deliveries in Nova Scotia, 1988–1995. Women in the lower family income groups were more likely than those in the highest income group to have a prepregnancy weight of 75 kg or more.
Women whose perinatal records did not link to income tax information had perinatal and infant outcomes similar to those of women whose records did link: preterm birth, 4.9% and 4.9%; small-for-gestational-age live birth, 11.6% and 10.7%; perinatal death, 7.5 and 7.6 per 1000 total births; and composite of perinatal death or serious neonatal morbidity, 14.9 and 14.1 per 1000 total births, respectively.
Rates of gestational diabetes were substantially and significantly higher among women in the lowest family income group than among those in the highest family income group (crude rate ratio [RR] 1.44, 95% confidence interval [CI] 1.21–1.73; RR adjusted for maternal age, parity, prepregnancy weight, smoking status, marital status, residence and period of delivery 2.48, 95% CI 1.93–3.20). Rates of gestational diabetes were higher among women who did not contribute to an RRSP than among those who did (crude RR 1.12, 95% CI 1.01–1.24), although adjusted rates did not differ significantly.
There were no significant differences in the crude or adjusted rates of pre-existing diabetes mellitus, placenta previa or chronic medical disease by family income. Crude rates of hypertensive disorders did not differ by family income (RR for lowest v. highest income group 0.89, 95% CI 0.76–1.05), although adjusted rates were significantly higher in the lowest family income group than in the highest income group (adjusted RR 1.33, 95% CI 1.05–1.69). In terms of investment status, women who did not contribute to an RRSP were more likely than those who did to have higher crude rates of diabetes mellitus (RR 1.34, 95% CI 0.99–1.80) and placental abruption (RR 1.34, 95% CI 1.13–1.58). Adjusted rates of chronic medical disease, placenta previa and placental abruption did not differ by investment status, although rates of hypertensive disorders (crude RR 1.07, 95% CI 0.96–1.19; adjusted RR 1.20, 95% CI 1.04–1.39) and diabetes mellitus (adjusted RR 1.45, 95% CI 1.00–2.11) were significantly higher among women who did not contribute to an RRSP.
The rate of preterm birth before 37 weeks was slightly higher in the lowest family income group than in the highest income group, but differences were not evident after adjustment for potential confounders (Table 1). Additional adjustment for previous low-birth-weight infant and previous cesarean delivery did not alter the results.
Table 1.
Small differences in crude rates of preterm birth among women who did not contribute to an RRSP were also abolished after adjustment (Table 1). Similar findings were obtained for preterm birth before 32 weeks (data not shown). The rates of small-for-gestational-age live birth (< 10th percentile) were substantially and significantly different by family income (Table 2). The rate of small-for-gestational-age live birth was 81% higher in the lowest income group than in the highest income group. Adjustment for potential confounders attenuated but did not abolish these differences. The rate of small-for-gestational-age live birth was 49% higher among women who did not contribute to an RRSP than among those who did, but adjustment for potential confounders abolished this difference (Table 2). Similar results were obtained with small-for- gestational-age live births below the third percentile.
Table 2.
The crude rate of perinatal death was significantly lower among women in 2 of the lower family income groups than among those in the highest income group. Adjustment for behavioural and lifestyle factors accentuated these differences: adjusted rates of perinatal death decreased proportionately with decreasing income levels (Table 3). Analysis that excluded perinatal deaths due to congenital anomalies yielded similar results. Perinatal death rates were higher among women who did not contribute to an RRSP than among those who did, and adjustment for confounders strengthened this relation (Table 3).
Table 3.
There was no statistically significant difference between the lowest and highest family income groups in the rate of the composite of perinatal death or serious neonatal morbidity (Table 4). Adjustment for behavioural and lifestyle factors resulted in significantly lower composite rates in the lowest 3 family income groups than in the highest income group. Women who did not contribute to an RRSP had higher composite rates than those who did, and adjustment for potential confounders did not alter this relation (Table 4).
Table 4.
Crude rates of stillbirth were significantly lower among women in the lowest 3 family income groups than among those in the highest income group (lowest v. highest RR 0.69, 95% CI 0.49–0.96). Crude rates of neonatal death did not differ between family income groups (lowest v. highest RR 0.82, 95% CI 0.53–1.27). Adjusted rates of stillbirth and of neonatal death were significantly lower among women in the lower family income groups than among those in the highest income group.
The crude rate of postneonatal death was more than 5 times higher among women in the lowest 2 family income groups than among those in the highest income group (Table 5). Adjustment for behavioural and lifestyle factors abolished these differences. Small numbers precluded a comparison of the rate of sudden infant death syndrome by family income group. Crude rates of postneonatal death were 3 times higher among women who did not contribute to an RRSP (Table 5) and crude rates of sudden infant death syndrome were 5 times higher (RR 5.10, 95% CI 1.84–14.2) than among women who did contribute to an RRSP. The crude rate of infant death was higher among women in the lowest 2 family income groups than among those in the highest income group, and adjusted rates were either significantly lower or no different among women in lower family income groups. Similarly, infant death rates were higher among women who did not contribute to an RRSP than among those who did.
Table 5.
Supplementary analyses showed that the effect of using alternative indices for quantifying socioeconomic status (e.g., after-tax v. before-tax income) yielded essentially the same results.
Interpretation
Our study shows that family income and RRSP investment status were weakly associated with preterm birth and more strongly associated with some pregnancy complications such as gestational diabetes and small-for-gestational-age live birth. Rates of perinatal death favoured the lower family income groups, although crude rates of the composite of perinatal death or serious neonatal morbidity did not. Rates of postneonatal death and of infant death were substantially higher in the lower family income groups than in the highest income group. Adjustment for behavioural and lifestyle factors abolished, accentuated, attenuated or unmasked the crude relations between socioeconomic status and perinatal outcomes. These results reveal some of the mechanisms underpinning socioeconomic effects. Thus, the lack of effect of family income on the crude rate of hypertensive disorders in pregnancy and the significant positive effect evident after controlling for smoking and other factors confirms the known protective effect that smoking has on rates of hypertensive disorders in pregnancy.27 On the other hand, higher maternal smoking rates explain a substantial component of the excess in small-for-gestational-age live births seen among women in the lower family income groups. Residual confounding due to smoking or other unmeasured health behaviours may be responsible for the differences that persisted after adjustment.
The magnitude and direction of the socioeconomic differences in perinatal mortality are both intriguing and puzzling. Given the patterns of stillbirth, neonatal death and serious neonatal morbidity, we speculate that the observed differences in perinatal mortality are related to higher rates of obstetric intervention in the lower family income groups than in the highest income groups. We have previously shown that adjusted rates of labour induction and cesarean delivery were higher among women in the lower family income groups than among those in the higher income groups in this study population.14 Higher rates of medically indicated early delivery appear to be responsible for reducing stillbirth rates in the lower family income groups. Such obstetric intervention may also have been responsible for the higher rates of preterm birth and serious neonatal morbidity observed in the lowest family income group. Some of the excess in postneonatal deaths observed in the lower family income groups may also have been because of these differences in serious neonatal morbidity.
We observed some unexpected differences in the direction of socioeconomic effects based on family income versus contribution to an RRSP. Women in the lowest family income group had lower rates of perinatal death and no difference in the crude composite rate of perinatal death or serious neonatal morbidity compared with women in the highest income group. However, rates of these 2 outcomes were significantly higher among women who did not contribute to an RRSP than among those who did. The reason for these contrasting patterns is not immediately obvious, although it is recognized that saving behaviour is associated with health effects that are distinct from those associated with family income.28
The differences in socioeconomic effects with regard to perinatal death and serious neonatal morbidity suggest that reductions in fetal and infant mortality may have occurred at the expense of serious neonatal morbidity. Studies from the United States29 have shown that, although death rates among infants with a birth weight of 500–999 g decreased several fold between 1982–1989 and 1990–1998, the rates of survival with impairment increased, as did the rate of survival without impairment. Recognition of this shift from death to serious neonatal morbidity and the expected increase in prevalence rates of handicap and disability30 suggest the need for increased investment in clinical and community infrastructure and other support.
Our results identify 2 potential gaps related to perinatal health. The substantial differences in postneonatal mortality by socioeconomic status suggests a relative lack of social and other support for socioeconomically vulnerable mothers and families in the first year after birth. The second issue pertains to information about healthy lifestyle choices, especially smoking, increased prepregnancy weight and older maternal age. The last risk factor was highly prevalent among women in the higher family income groups (Figure 1).
The limitations of our study include an inability to link all records. Our supplementary analyses suggest, however, that unlinked records were a random subset of all records with regard to adverse perinatal outcomes. The exclusion of records with missing values in the regression analysis is another limitation of our study. Most of the missing values related to information on prepregnancy weight and smoking. Although it is difficult to assess the impact of these missing values, we do not believe such exclusions had a major effect on the results of regression. We did not have information on educational status, a factor associated with perinatal outcomes,7,11 although we did adjust for various correlates of education. Nevertheless, our indices of socioeconomic status focus more on economic and less on social aspects. Although our study was based on relatively old data, the observed relation between socioeconomic status and perinatal outcomes is probably sufficiently robust to inform current public policy. Also, our study provides a benchmark for socioeconomic differentials: future studies will determine whether socioeconomic disparities in perinatal outcomes increased in the mid to late 1990s, when the Canadian health care system was subjected to severe fiscal duress.31
In summary, our study shows that, despite the availability of essential health care services at no out-of-pocket expense, family income and other socioeconomic factors are strongly associated with some adverse perinatal outcomes, including gestational diabetes, small-for-gestational-age live births and infant death. These findings highlight potential gaps in health information and in social support for socioeconomically vulnerable mothers and families in the year after birth.
Methodological pearl
To assume a middle-income status for a particular household because it happens to be in a neighbourhood with an average middle-income status may be misleading. In reality, the neighbourhood may consist of low-income and high-income households and no middle-income ones. The assumption in this case does not account for the 2 distinct groups and is a simple example of an ecological fallacy that can occur when aggregate data for a group are used for an individual. Joseph and associates avoid this potential pitfall in their determination of socioeconomic status by performing a confidential linkage with individual family income data. This linkage was made possible by the cooperation of the Small Area and Administrative Data Division of Statistics Canada. It is an example of how confidential national data can be successfully linked with data from a provincial database, in this case the Nova Scotia Atlee Perinatal Database, to avoid a subtle but potentially misleading bias. — CMAJ
Footnotes
-
Une version française de ce résumé est disponible à l'adresse www.cmaj.ca/cgi/content/full/177/6/583/DC1
This article has been peer reviewed.
Contributors: K.S. Joseph, Robert Liston, Linda Dodds and Alexander Allen proposed the study. K.S. Joseph carried out the analyses with help from the Small Area and Administrative Data Division of Statistics Canada, and all of the authors reviewed the preliminary and final analyses. K.S. Joseph drafted the manuscript and revised it based on comments from the other authors. All of the authors approved the final manuscript for publication.
Acknowledgements: We thank the Small Area and Administrative Data Division of Statistics Canada, especially Pat Grainger, Eric Olson, Jeffrey Smith, Linda Standish, Bill Steele, Tom Swoger and Kathleen Trudeau, for data linkage and analysis. We also thank the Reproductive Care Program of Nova Scotia for access to the data.
K.S. Joseph is supported by a Peter Lougheed New Investigator award. Linda Dodds is supported by a New Investigator award from the Canadian Institutes of Health Research and a Clinical Scholar award from the Dalhousie University Faculty of Medicine. This study was funded by grant no. MOP-43992 from the Canadian Institutes of Health Research.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Social inequalities in pregnancy metabolic profile: findings from the multi-ethnic Born in Bradford cohort study
- A Scoping Review on Influence of Socioeconomic Status on Antenatal Care Utilization and Pregnancy Outcomes in Sub-Saharan Africa
- Infant born with Robert's syndrome without prenatal care in a developing nation
- Psychosocial deprivation in women with gestational diabetes mellitus is associated with poor fetomaternal prognoses: an observational study
- Increasing educational inequality in preterm birth in Quebec, Canada, 1981-2006
- The effect of neighbourhood income and deprivation on pregnancy outcomes in Amsterdam, The Netherlands
- Approaches to diversity in family medicine: "I have always tried to be colour blind"
More in this TOC Section
Similar Articles

