


- © 2004 Canadian Medical Association or its licensors
Abstract
Background: Despite the increase in the number of Aboriginal people with end-stage renal disease around the world, little is known about their health outcomes when undergoing renal replacement therapy. We evaluated differences in survival and rate of renal transplantation among Aboriginal and white patients after initiation of dialysis.
Methods: Adult patients who were Aboriginal or white and who commenced dialysis in Alberta, Saskatchewan or Manitoba between Jan. 1, 1990, and Dec. 31, 2000, were recruited for the study and were followed until death, transplantation, loss to follow-up or the end of the study (Dec. 31, 2001). We used Cox proportional hazards models to examine the effect of race on patient survival and likelihood of transplant, with adjustment for potential confounders.
Results: Of the 4333 adults who commenced dialysis during the study period, 15.8% were Aboriginal and 72.4% were white. Unadjusted rates of death per 1000 patient-years during the study period were 158 (95% confidence interval [CI] 144–176) for Aboriginal patients and 146 (95% CI 139–153) for white patients. When follow-up was censored at the time of transplantation, the age-adjusted risk of death after initiation of dialysis was significantly higher among Aboriginal patients than among white patients (hazard ratio [HR] 1.15, 95% CI 1.02–1.30). The greater risk of death associated with Aboriginal race was no longer observed after adjustment for diabetes mellitus and other comorbid conditions (adjusted HR 0.89, 95% CI 0.77–1.02) and did not appear to be associated with socioeconomic status. During the study period, unadjusted transplantation rates per 1000 patient-years were 62 (95% CI 52–75) for Aboriginal patients and 133 (95% CI 125–142) for white patients. Aboriginal patients were significantly less likely to receive a renal transplant after commencing dialysis, even after adjustment for potential confounders (HR 0.43, 95% CI 0.35–0.53). In an additional analysis that included follow-up after transplantation for those who received renal allografts, the age-adjusted risk of death associated with Aboriginal race (HR 1.36, 95% CI 1.21–1.52) was higher than when follow-up after transplantation was not considered, perhaps because of the lower rate of transplantation among Aboriginals.
Interpretation: Survival among dialysis patients was similar for Aboriginal and white patients after adjustment for comorbidity. However, despite universal access to health care, Aboriginal people had a significantly lower rate of renal transplantation, which might have adversely affected their survival when receiving renal replacement therapy.
In North America and the Antipodes, the incidence of diabetes among adolescent and adult Aboriginals has risen dramatically,1,2,3,4 with corresponding increases in the prevalence of diabetic nephropathy.5,6,7 Aboriginal people in Canada have experienced disproportionately high incidence rates of end-stage renal disease (ESRD), with an 8-fold increase in the number of prevalent dialysis patients between 1980 and 2000.8 Although the incidence of ESRD appears to have decreased in recent years, the prevalence of diabetes mellitus and its complications are rising, especially among young people.9,10,11
Most work evaluating health outcomes among Aboriginal people considers either the general population12or diseases for which interventions are implemented over a short period, such as alcohol abuse,13 injury14 or critical illness.15 Death and markers of poor health are significantly more common among Aboriginal people than among North Americans of European ancestry, perhaps because of the greater prevalence of diabetes mellitus, adverse health effects due to lower socioeconomic status16 and reduced access to primary care.17 Aboriginal patients may also face unique barriers to care, including mistrust of non-Aboriginal providers, institutional discrimination or preference for traditional remedies.18 These factors may be most relevant when contact with physicians is infrequent, which obstructs development of a therapeutic relationship. In contrast, ESRD is a chronic illness that requires ongoing care from a relatively small, stable multidisciplinary team.
Although recent evidence highlights racial inequalities in morbidity and mortality among North Americans with ESRD, most studies have focused on black or Hispanic populations.19We conducted this study to evaluate rates of death and renal transplantation among Aboriginal people after initiation of dialysis in Alberta, Saskatchewan and Manitoba.
Methods
We studied all adult patients who commenced dialysis treatment in Alberta, Saskatchewan and Manitoba between Jan. 1, 1990, and Dec. 31, 2000. We restricted the study to these provinces (where most of the Aboriginal population is from the Cree, Ojibway, Seaulteux and Blackfoot tribes) to increase the homogeneity of the study population. We included only patients treated in centres with kidney transplant programs because differential access to transplantation might affect survival when undergoing dialysis.
Anonymized data were provided by the sole national population-based organ failure registry in Canada, the Canadian Organ Replacement Registry (CORR).20,21 Patient-specific data, including demographic characteristics, initial mode of dialysis and comorbid conditions at the time of first dialysis treatment, are collected by health care professionals (on the basis of personal knowledge of the patient, chart review and, in some cases, direct inquiry) and are submitted annually to CORR by all Canadian dialysis centres. Changes in treatment modality (including transplantation) and dates of allograft failure and death are also recorded.
In CORR, patient race is categorized as white, black, Aboriginal, Asian, Indian subcontinent, Mideast/Arabian, Pacific Islander, other or unknown. The CORR instructions for data collection define Aboriginal race as people of “First Nations, Inuit, or Métis” origin. Race is determined at the discretion of the health care professional, since CORR procedure does not require that patients be asked directly about racial status. Because the focus of this study was on people of Aboriginal race and because nonwhite, non-Aboriginal people requiring renal replacement therapy have lower rates of death than white people,22 the analysis presented here includes only comparisons between white and Aboriginal subjects.
Differences between the groups were compared with χ2 tests for categorical variables and t tests for continuous variables. We estimated socioeconomic status using the neighbourhood income per person equivalent (IPPE), a measure of household income that is adjusted for the size of the household, based on summary data from the 1996 Canadian census. Within each community, the average IPPE was used to rank all subcommunities, and then the population was divided into approximate fifths to create community-specific income quintiles.23 Community size, also obtained from census data, was used as a surrogate for urban or rural location of residence and was characterized by a 4-category variable ranging from small towns with fewer than 10 000 people to large urban centres with more than 500 000 people.
Patients were followed from initiation of dialysis until death, transplantation, loss to follow-up or the end of the study (Dec. 31, 2001). We examined the effect of individual factors, including race, on patient survival using Cox proportional hazards analysis that adjusted only for age as a continuous variable. We then determined whether the effects of race were statistically independent of other factors using Cox proportional hazards analyses that included variables showing an association (p < 0.10) with survival in univariate Cox regression analyses. The following factors were considered: age, sex, Aboriginal race, initial and subsequent modes of dialysis, socioeconomic status (as IPPE), smoking status, year from initiation of dialysis, community size, dialysis centre (to account for regional differences in clinical practice) and comorbid conditions, including coronary disease (angina, myocardial infarction, previous coronary artery bypass grafting), previous or current hypertension, chronic heart failure, stroke, lung disease, peripheral vascular disease, malignant disease and other serious illness anticipated to significantly reduce life expectancy. Missing comorbidity data (representing about 8% of all information on comorbidity) was dealt with in 2 ways: by assuming that the characteristic was absent and by using dummy variables to denote missing data. The results did not differ with these 2 methods, so here we have reported results using the latter method. Cross-product interaction terms were used to determine whether the effect of race was modified by age, sex, diabetes or socioeconomic status. In the primary analysis, follow-up was censored at the time of renal transplantation. We also performed a separate Cox regression analysis in which patient follow-up continued after transplantation.
We used additional proportional hazard models to examine the relation between race and likelihood of renal transplantation. We determined that the proportional hazard assumption was satisfied by examining plots of the log-negative-log of the within-group survivorship functions versus log time as well as comparing Kaplan–Meier (observed) with Cox (expected) survival curves.24 Statistical significance was defined by p < 0.05. The study was approved by the institutional review board at the University of Alberta.
Results
A total of 4840 patients commenced dialysis in Alberta, Saskatchewan and Manitoba during the study period, and for 4333 of these patients, “race” was identified in CORR. Aboriginal patients accounted for 685 (15.8%) of the study population but 8.7% of the total population in the catchment area, which suggests that the unadjusted prevalence of ESRD is approximately twice as high among Aboriginal people as among non-Aboriginals. Although the incidence of ESRD increased over the study period for all racial groups (data not shown), the proportion of incident patients who were Aboriginal remained similar over the study period (p = 0.26). Of the 4333 incident patients, 510 were of non-Aboriginal, nonwhite race and were excluded from further analysis. The demographic characteristics of the remaining 3823 patients appear in Table 1. Of these, 16 (0.4%) were lost to follow-up, and their data were censored after a median period of 21 days.
Table 1.
Aboriginal patients were younger, less likely to be male and more likely to have diabetes mellitus, chronic heart failure and peripheral vascular disease than white patients (Table 1). Aboriginal patients were less likely to have coronary disease, hypertension or known malignancy at the time of commencing dialysis, less likely to start renal replacement on peritoneal dialysis and more likely to be in the lowest quintile of socioeconomic status.
During the study period, the unadjusted rate of death per 1000 patient-years was 158 (95% confidence interval [CI] 144–176) for Aboriginal patients and 146 (95% CI 139–153) for white patients. The age-adjusted risk of death after initiation of dialysis was significantly higher among Aboriginal than among white patients (hazard ratio [HR] 1.15, 95% CI 1.02–1.30). The greater age-adjusted risk associated with Aboriginal race was no longer observed after adjustment for the presence or absence of diabetes mellitus (adjusted HR 1.03, 95% CI 0.91–1.16). Further adjustment for other comorbidity and cause of ESRD further reduced the risk of death associated with Aboriginal race (HR 0.99, 95% CI 0.87–1.12). In the fully adjusted model, Aboriginal race was associated with an 11% lower risk of death than white race, although the difference was not statistically significant (HR 0.89, 95% CI 0.77–1.02) (Table 2, Fig. 1).
Table 2.

Fig. 1: Adjusted survival of patients, by race. The data have been adjusted for age, sex, cause of end-stage renal disease (ESRD), diabetes mellitus, other comorbidity, mode of dialysis, dialysis centre, era effect, socioeconomic status and location of residence (urban or rural).
The result of a test for interaction was statistically nonsignificant, which suggests that socioeconomic status was associated with mortality to a similar extent among Aboriginals and whites. In addition, there was no evidence that dialysis centre, patient age, patient sex or initial mode of dialysis interacted with the effect of Aboriginal race on mortality, which suggests that the effect of race was homogeneous within the study population.
After initiation of dialysis, Aboriginal patients were significantly less likely to undergo renal transplantation than white patients. During the study period, the crude transplantation rate per 1000 patient-years was 62 (95% CI 52–75) for Aboriginal patients and 133 (95% CI 125–142) for white patients. Aboriginal patients were significantly less likely than white patients to receive a cadaveric transplant (12.1% v. 20.5%, p < 0.001) or a living related transplant (4.7% v. 9.2%, p < 0.001).
Using Cox proportional hazard models, we adjusted for other measured variables that might confound the relation between race and transplantation (Table 2). In that analysis, Aboriginal race was independently associated with a reduced likelihood of renal transplantation (HR 0.43, 95% CI 0.35–0.53). The results were similar when patients who received renal transplants from living donors were excluded from the analysis (HR 0.46, 95% CI 0.36–0.58) or when their data were censored at the time of transplantation (HR 0.48, 95% CI 0.38–0.61). Adjustment for socioeconomic status did not affect the likelihood of transplantation by race in any of the models (data not shown). In Fig. 2A, the adjusted incidence of transplantation is plotted against time for these 2 groups, stratified by diabetic status.
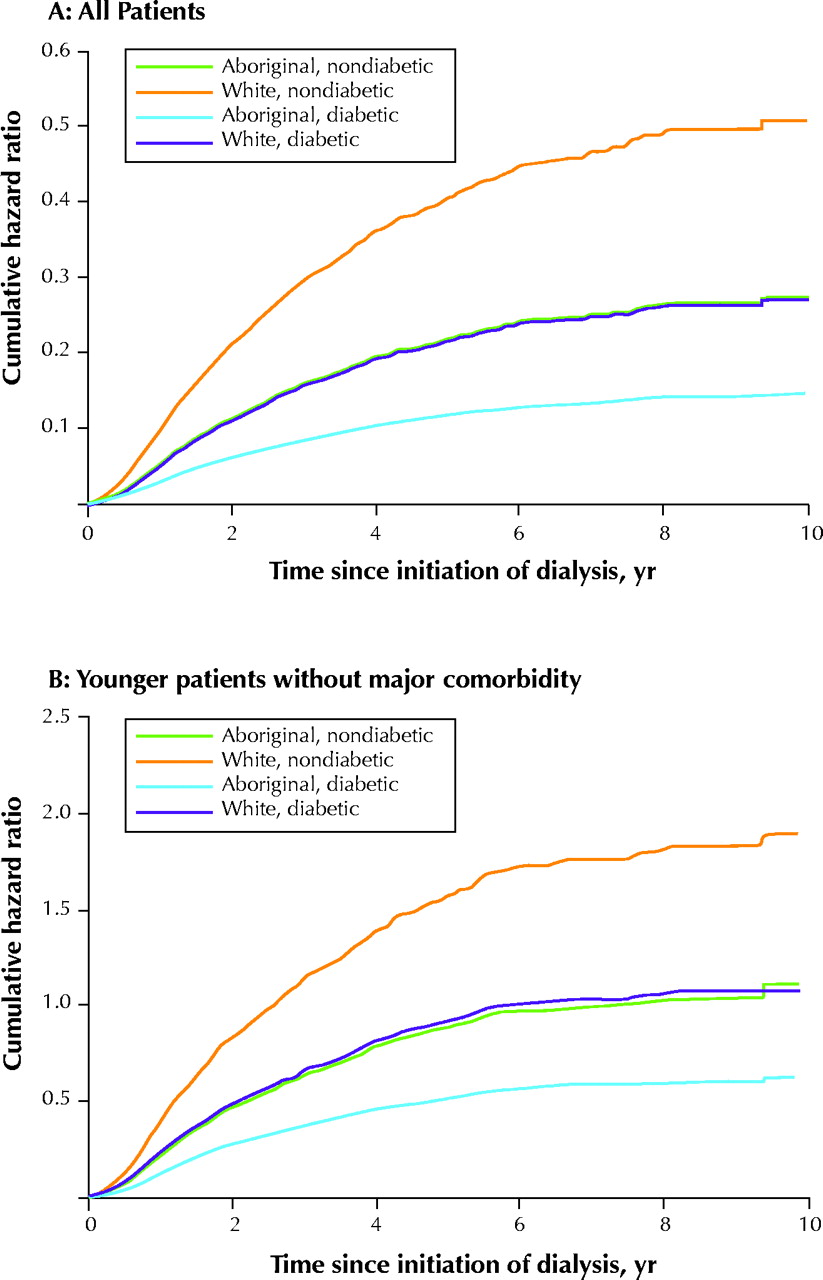
Fig. 2: Likelihood of renal transplantation by race and diabetic status, adjusted for age, sex, cause of ESRD, diabetes mellitus, mode of dialysis, dialysis centre, era effect, socioeconomic status and location of residence (urban or rural), expressed as the cumulative hazard ratio. A: All patients commencing dialysis treatment; these data are also adjusted for comorbidity. B: Younger patients without major comorbidity (age less than 60 years without known coronary disease, chronic heart failure, stroke, chronic lung disease, peripheral vascular disease, malignant or other serious medical illness that would be expected to reduce life expectancy). In both analyses, Aboriginal patients were significantly less likely to receive renal transplants (p < 0.001).
Because we did not have information on patients' transplant wait-list status, it is possible that comorbidity affected eligibility and thus rates of transplantation. We attempted to address this possibility by performing an additional analysis that considered only younger patients with less comorbidity (age less than 60 years without known coronary disease, chronic heart failure, stroke, chronic lung disease, peripheral vascular disease, known malignant or other serious medical illness that would be expected to reduce life expectancy). In these 1167 patients, and after stratification for diabetic status, Aboriginal race was again independently associated with lower rates of renal transplantation (HR 0.47, 95% CI 0.37–0.60) (Fig. 2B).
Because renal transplantation is associated with lower rates of death than dialysis,25 different rates of transplantation would be expected to influence comparative mortality between racial groups. However, such differences would not be apparent in models that end follow-up at the time of transplantation. To address this issue, we developed additional Cox proportional hazard models for all subjects who commenced renal replacement therapy and included survival after transplantation for those who received renal allografts. In these analyses, the age-adjusted risk of death after initiation of dialysis was higher among Aboriginal patients than white patients (HR 1.36, 95% CI 1.21–1.52), although the fully adjusted risk of death was similar in the 2 groups (HR 1.02, 95% CI 0.90–1.16). The risk of death associated with Aboriginal race was higher in both analyses that included follow-up after transplantation than in the analyses that ended follow-up at the time of transplantation (HR 1.15 and 0.89 respectively; Table 2). This result suggests that the lower transplantation rate among Aboriginals may adversely affect their survival when receiving renal replacement therapy.
Interpretation
Although Aboriginal patients treated with dialysis in the Prairie provinces had higher age-adjusted rates of death than white patients, this difference was no longer observed when the analysis was adjusted for other variables associated with survival, especially diabetes mellitus. Contrary to observations from other populations,12,14 the survival of Aboriginals with ESRD appeared to be at least as good as in white patients after adjustment for concomitant illness.
After adjustment for comorbidity, underlying renal disease, location of residence and socioeconomic status, Aboriginal people were less than half as likely to receive renal transplants, which in turn appeared to increase the excess age-adjusted mortality associated with Aboriginal race. This disparity was consistent regardless of donor source (living or cadaveric) and was similar when only young patients without documented comorbidity were considered. Because renal transplantation is associated with lower rates of death,25 higher quality of life26 and lower health care costs than dialysis treatment, the lower transplantation rate among Aboriginal people warrants further investigation.
Our data do not allow us to identify the reasons for the differential access to transplantation by race, but it seems improbable that differences in medical suitability were exclusively responsible. Aboriginal patients might be less likely to be put on waiting lists for transplantation (because of higher rates of comorbidity or perceived poor adherence) or less likely to be matched with a suitable donor (because of lower rates of live kidney donation, less common human leukocyte antigen types or bias in organ allocation). In addition, Aboriginal patients might be less likely to want a renal transplant than white patients, as is the case for other ethnic minorities.27 Because of geographic isolation, Aboriginal people may have reduced access to transplantation services or be less likely to attend appointments or procedures aimed at determining suitability for transplantation. However, in the current study, the lower renal transplantation rate among Aboriginal people was independent of residence location, and our study was restricted to regions served by renal transplant programs. Finally, the reduced rates of transplantation among Aboriginals did not vary by dialysis centre. These findings argue against geographic factors as being responsible for differential rates of transplantation by race.
In previous work, referral rates for renal transplant assessment were similar for Native American and white patients residing in Arizona and New Mexico, but the delay between starting dialysis and transplantation was significantly longer for the Native Americans.28 Similarly, a study conducted in Australia and New Zealand found that indigenous people experienced longer delays than white subjects between starting dialysis and placement on the waiting list for transplantation and between wait-listing and transplantation.5 These findings are similar to those observed for black patients treated for ESRD in the United States.29
Our study had several limitations. First, referral patterns might have influenced differences in mortality or transplantation rates between the racial groups. We did not have information on the timing of nephrology referral or the level of residual renal function at the time dialysis treatment began. Second, it is possible that bias resulted from the exclusion of patients with unknown racial status. However, it is unlikely that these data would be missing more frequently among Aboriginal patients. Information that was missing or incorrect at random would bias our results toward the null, and repeating our analyses classifying all people of unknown race as white did not change any of the findings (data not shown). Similarly, racial status was provided to CORR by dialysis centre personnel, rather than the subjects themselves, and race might therefore have been incorrectly classified in some cases. Although we cannot exclude this possibility, it is unlikely that differential misclassification occurred by race. Again, this suggests that any resulting bias would reduce the statistical power rather than result in spurious findings. Finally, our analyses are limited by the lack of data on transplant wait-list status, which might help to explain how the markedly lower renal transplantation rates among Aboriginal patients could be increased.
In conclusion, we found that Aboriginal patients treated for ESRD in the Prairie provinces had more comorbid illness at initiation of dialysis than white patients. Once established on renal replacement, such patients had higher age-adjusted rates of death, but after further adjustment for diabetes mellitus and other comorbid illness, rates of death were similar for Aboriginal and white patients. However, Aboriginal patients had lower rates of renal transplantation than non-Aboriginals, independent of measured comorbidity and socioeconomic and geographic factors. These findings require further investigation.
Footnotes
-
This article has been peer reviewed.
Contributors: Drs. Tonelli, Gill and Hemmelgarn were responsible for study conception and design. All authors participated in the analysis and interpretation of the data. Dr. Tonelli drafted the article, and all authors helped to revise the article for important intellectual content and approved the final version for publication.
Acknowledgements: We thank Frank Ivis and Kim Badovinac of the Canadian Organ Replacement Register for their assistance in facilitating our data request. Grant support for this work was received from the Alberta Heritage Foundation for Medical Research (through Dr. Tonelli), the Canadian Institutes of Health Research (through Dr. Manns) and the Kidney Foundation of Canada (through Dr. Gill). CORR is funded by Health Canada (15%) and the provincial and territorial departments of health (80%) on the basis of population. The Kidney Foundation of Canada and the health care industry provide the remaining funding (approximately 5%).
Competing interests: None declared.
Correspondence to: Dr. Marcello Tonelli, Division of Nephrology, University of Alberta, 7-129 Clinical Science Bldg., 8440 112 St., Edmonton AB T6G 2G3; fax 780 407-7878; mtonelliualberta.ca
References
In this issue

{kind=link}
{kind=link}
Article tools



Jump to section
Related Articles
Cited By...
- Racism as a determinant of health and health care: Rapid evidence narrative from the SAFE for Health Institutions project
- Le racisme comme determinant de la sante et des soins de sante: Sommaires narratifs des donnees probantes produits par le projet SAFE pour les etablissements de sante
- Issues postoperatoires chez les Autochtones au Canada: revue systematique
- Postoperative outcomes for Indigenous Peoples in Canada: a systematic review
- Association of Modality with Mortality among Canadian Aboriginals
- Management of aboriginal and nonaboriginal people with chronic kidney disease in Quebec: Quality-of-care indicators
- Dialysis and transplantation among Aboriginal children with kidney failure
- AN INTERNATIONAL PERSPECTIVE ON PERITONEAL DIALYSIS AMONG INDIGENOUS PATIENTS
- Peritonitis and Exit Site Infections in First Nations Patients on Peritoneal Dialysis
- Adverse outcomes among Aboriginal patients receiving peritoneal dialysis
- Model for Equitable Care and Outcomes for Remote Full Care Hemodialysis Units
- Similar Outcomes among Black and White Renal Allograft Recipients
- Access to health care among status Aboriginal people with chronic kidney disease
- Prejuges en medecine: Notre role dans les inegalites en matiere de sante
- Prejudice in medicine: Our role in creating health care disparities
- Prevalence of Chronic Kidney Disease and Survival among Aboriginal People
- Quality of Care among Aboriginal Hemodialysis Patients
- Canadian Society of Transplantation: consensus guidelines on eligibility for kidney transplantation
- The ethics of research involving Canada's Aboriginal populations
- The ethics of research involving Canada's Aboriginal populations
- The ethics of research involving Canada's Aboriginal populations
- Health outcomes in Aboriginal populations
More in this TOC Section
Similar Articles
Collections

