


- © 2004 Canadian Medical Association or its licensors
Abstract
Background: The Greater Toronto Area (GTA) was considered a “hot zone” for severe acute respiratory syndrome (SARS) in 2003. In accordance with mandated city-wide infection control measures, the Hospital for Sick Children (HSC) drastically reduced all services while maintaining a fully operational emergency department. Because of the GTA health service suspensions and the overlap of SARS-like symptoms with many common childhood illnesses, this introduced the potential for a change in the volumes of patients visiting the emergency department of the only regional tertiary care children's hospital.
Methods: We compared HSC emergency department patient volumes, admission rates and length of stay in the emergency department in the baseline years of 2000–2002 (non-SARS years) with those in 2003 (SARS year). The data from the prior years were modeled as a time series. Using an interrupted time series analysis, we compared the 2003 data for the periods before, during and after the SARS periods with the modeled data for significant differences in the 3 aforementioned outcomes of interest.
Results: Compared with the 2000–2002 data, we found no differences in visits, admission rates or length of stay in the pre-SARS period in 2003. There were significant decreases in visits and length of stay (p < 0.001) and increases in admission rates (p < 0.001) during the periods in 2003 when there were new and active cases of SARS in the GTA. All 3 outcomes returned to expected estimates coincident with the absence of SARS cases from September to December 2003.
Interpretation: During the SARS outbreak in the GTA, the HSC emergency department experienced significantly reduced volumes of patients with low-acuity complaints. This gives insight into utilization rates of a pediatric emergency department during a time when there was additional perceived risk in using emergency department services and provides a foundation for emergency department preparedness policies for SARS-like public health emergencies.
SARS, caused by a novel coronavirus,1,2 claimed 43 lives of the 251 probable cases in Canada in 2003.3According to the World Health Organization, SARS can be defined if certain clinical characteristics are present in conjunction with specific risk factors.4,5,6,7,8
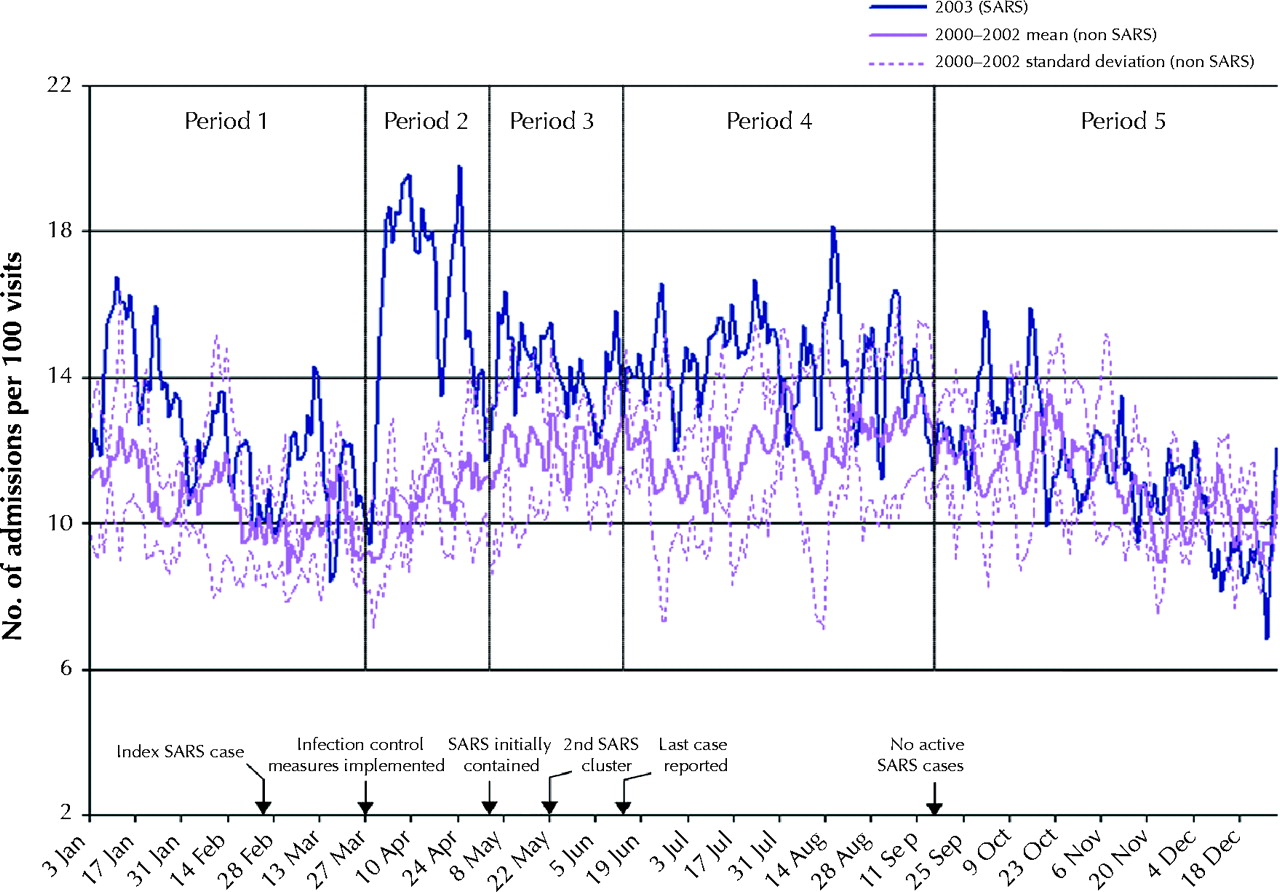
The Greater Toronto Area (GTA) was the “hot zone” for SARS in Canada, as the overwhelming majority of cases in the country and all of the SARS-related deaths occurred there.4 Strict infection control measures were mandated in the Toronto regional hospitals on Mar. 27,9 and although an initial containment was achieved by May 4, a second cluster of SARS cases appeared in the GTA on May 2210 (Fig. 1).

From Mar. 27 to May 12, 2003, Canada's largest pediatric hospital, the Hospital for Sick Children (HSC), cancelled all nonurgent services for 3.5 weeks and operated below capacity for a further 3 weeks. Compared with 2002 statistics, about 3000 outpatient clinic visits, at least 200 surgical cases and 2000 visits for diagnostic services were cancelled by the hospital.13 The HSC emergency department acted as the referral centre for screening all suspected pediatric SARS cases in the GTA. All pediatric cases identified from the HSC and any of the other GTA hospitals were admitted to the newly established SARS ward at the HSC. The ward treated 24 SARS cases: one-third came from the HSC emergency department and the remainder were transferred from other hospitals directly to the ward. The most severely affected patient with SARS required minimal oxygen supplementation and was 17 years of age, reinforcing the experience in China that children usually present with a mild form of the disease.14 Therefore, the impact of SARS on the pediatric population, unlike that on the adult population, resulted almost exclusively from indirect effects on health care delivery rather than from direct disease effects.
Emergency departments across the GTA anticipated increased patient volumes, similar to those in influenza epidemics.15,16,17 Indeed, the heightened awareness of SARS symptoms among the general public and the overlap of these symptoms with many common illnesses contributed to public response. For example, in April 2003 a Toronto-based tertiary care teaching hospital screened more than 1000 concerned members of the public, 70 of whom met the case definition of suspected or probable SARS (unpublished data). An emergency department at another tertiary care hospital in the GTA found that, early in the SARS outbreak, up to 50% of presenting patients had concerns that their symptoms were SARS-related (unpublished data).
Since children are susceptible to frequent upper respiratory tract infections, the overlap of presenting symptoms of these common pediatric illnesses with those of SARS may therefore be especially relevant to children. As a result, the potential concern among parents of children with respiratory tract infections with respect to SARS may have been reflected in increased visits to the HSC emergency department. Therefore, we conducted this study to examine the changes in the number and types of visits to the HSC emergency department observed during the SARS outbreak in the GTA. The aim was to gain insight into the patient use of a tertiary care pediatric emergency department when it was perceived that seeking medical attention was associated with an increased risk of contracting disease and to contribute clinical information for the preliminary foundation of emergency department preparedness policies for SARS-related and SARS-like public health emergencies.
Methods
This was a retrospective, interrupted time series study conducted at a single centre. The HSC emergency department is the only pediatric tertiary care emergency department in the GTA and treats 55 000 patients annually. This study was given approval from the hospital's Research Ethics Board.
The study period was from Jan. 1 to Dec. 31, 2003 (SARS period), and the control period was from Jan. 1 to Dec. 31 in the years 2000–2002 inclusive (non-SARS period). We examined outcome-relevant patient statistics, including total daily visits, daily median length of stay (LOS) in the emergency department (from time of registration to discharge from the emergency department) and hospital admission rates (the number of admissions from the HSC emergency department relative to the total number of visits). The relevant data were obtained from the HSC emergency department's patient database and extracted by the HSC database team.
Total visits included all children who presented to the HSC emergency department during the study and control periods. Hospital admissions included all those of children assessed at the HSC emergency department who subsequently required inpatient care.
For our analysis, we divided the SARS outbreak period in the GTA into 5 clinically relevant periods. Period 1 (Feb. 15 to Mar. 26) represented the time when there were only a few cases of SARS in the GTA and there was relatively little public awareness. Period 2 (Mar. 27 to May 4) represented the time when the strictest city-wide infection control measures were in place and reflected the peak of SARS cases to initial containment of SARS on May 4. Period 3 (May 5 to June 12) reflected both the initial containment of SARS and the second, smaller SARS cluster, which occurred during the last 3 weeks of this period, from May 23 to June 12. Period 4 (June 13 to Sept. 15) represented the time when there were still active SARS cases but no new SARS cases and there was continued screening at HSC. Period 5 (Sept. 16 to Dec. 31) reflected the time when there were no SARS cases in the GTA.
The data from all of the study years (SARS and non-SARS years) were modelled as a time series.18,19 The 5 defined periods were used as comparison periods. Any differences in 2003 (SARS year) in the 3 outcomes of interest (daily visits, admission rates and LOS) during these periods were determined by the time series analysis. Seasonal exponential smoothing was used to account for the random shift of mean levels and seasonality. Based on the autocorrelation and partial correlation plots of the residuals, a first-order moving-average model was fitted to account for the residual autocorrelation. Indicators for the different periods were investigated for deterministic shift of the mean levels from baseline. For all 3 models, the moving-average estimate was significant (daily visits: –0.51, standard error 0.023, p < 0.001; admission rates: –0.11, standard error 0.53, p < 0.001; and LOS: –0.30, standard error 0.023, p < 0.001). After fitting the exponential smoothing model with the moving-average component, the Ljung–Box goodness-of-fit measure showed that there was no evidence to reject the model. The variance accounted for in the models was 0.72 for daily visits and 0.30 for LOS and for admission rates.
Results
The mean age (and standard deviation) of the children seen in the HSC emergency department during the control and study periods was 4.8 (4.8) and 5.0 (5.1) years respectively. In both periods, 55.0% of the patients were male.
Details of the time series analysis appear in Table 1. During period 1, there were no significant differences from expected estimates in the number of visits, the admission rates and the LOS in the emergency department. However, during periods 2, 3 and 4 (when there were new and active SARS cases), there were significant differences from expected estimates for all outcomes except for the LOS in period 3. From the estimated baseline of 133 visits per day to the emergency department, the number was found to decrease by 48, 35 and 25 patients per day on average during periods 2, 3 and 4 respectively (p < 0.001). Admission rates increased significantly from the estimated baseline of 11.4% by a mean of 4.7% in period 2 and by 3% in periods 3 and 4 (p < 0.001). Compared with the estimated baseline of 3.0 hours, LOS in the emergency department was significantly lower during the initial height of SARS cases (period 2) by a mean of 0.5 hours (p < 0.001), and when there were active SARS cases but no new cases (period 4) by a mean of 0.3 hours (p < 0.002). During period 5, when there were no cases of SARS in the GTA, there were no significant differences in any of the outcomes.
Table 1.
Descriptive data are depicted in Figs. 2, 3 and 4. Mean and standard deviations of the number of emergency department visits, admission rates and LOS for the non-SARS years and the absolute values for the SARS year are displayed. Values were smoothed using a 5-point moving-average algorithm.

Fig. 4: Length of stay in HSC emergency department for patients seen from Jan. 1 to Dec. 31, 2003 (SARS year), compared with those seen in 2000–2002 (non-SARS years).

Fig. 3: Hospital admission rates (per 100 visits to the HSC emergency department) from Jan. 1 to Dec. 31, 2003 (SARS year), compared with rates in 2001–2002 (non-SARS years).

Fig. 2: Number of patient visits per day to the Hospital for Sick Children (HSC) emergency department from Jan. 1 to Dec. 31, 2003 (SARS year), compared with number of visits in 2000–2002 (non-SARS years). Period 1 (Feb. 15 to Mar. 26) = only a few cases of SARS in GTA and relatively little public awareness. Period 2 (Mar. 27 to May 4) = strictest city-wide infection control measures in place and peak of SARS cases to initial containment of SARS on May 4. Period 3 (May 5 to June 12) = initial containment of SARS and second, smaller SARS cluster, which occurred during last 3 weeks of this period. Period 4 (June 13 to Sept. 15) = still active SARS cases but no new SARS cases, and continued SARS screening at HSC. Period 5 (Sept. 16 to Dec. 31) = no SARS cases in GTA.
Interpretation
Our study data demonstrate a significant reduction in the total number of visits to the HSC emergency department during the SARS outbreak in the GTA and a significant increase in the proportion of patients admitted. The decrease in visits was probably due primarily to fewer patients than would normally present with lower acuity problems.
This drop in pediatric visits during the SARS period is in contrast to the increased number of patient visits during influenza epidemics.15,16,20 However, unlike the well-characterized and familiar symptoms and cause of influenza, SARS emerged as a new infection caused by a poorly understood virus. Furthermore, its rapid local and international spread and its ability to infect large numbers of healthy hospital staff,5,21 some of whom required intensive care, generated much attention in the global media. In response, people in the GTA limited their activities associated with risk of exposure. For example, the Toronto Transit Commission noted a decrease in ridership by 500 000 between Mar. 23 and Apr. 4, 2003.22 Because of its status as the referral centre for all pediatric cases of SARS, the HSC emergency department may have been perceived by the public as a site of potential exposure. Furthermore, the Ontario Public Health department advised people with SARS-like symptoms to stay home, regardless of their history of contact with SARS.23 This advice and the fear of contracting SARS probably accounted for the most part to the reduced patient volumes.
For some of the children who did not visit the HSC emergency department during the study period, their parents may have received telephone advice. Telehealth Ontario is a provincial telephone advice line staffed 24 hours a day, 7 days a week by registered nurses. About 40% of the calls they receive are related to pediatric illness. Telehealth Ontario reported a 2-fold increase in pediatric calls during period 2 compared with the volume in the previous year, and about half of the increase was related to non-SARS-related calls (Laurie Poole, Telehealth Ontario: personal communication, 2003). Furthermore, in response to a reported increase in telephone advice given by the primary care physicians, the Ontario Ministry of Health and Long-term Care introduced a reimbursement system for phone consultations.24 As a result, the SARS outbreak encouraged the general public to use an alternative way to address medical complaints. The increased use of phone consultation supports the need to pursue strategies other than emergency department services to address nonurgent medical issues.
Our study has several limitations. It was conducted in a single, urban, pediatric tertiary care emergency department, and therefore the generalizability of these findings is limited to comparable institutions. In addition, how the public used the HSC emergency department during the SARS outbreak may not reflect future use.
In conclusion, during the period when there were active SARS cases and heightened public awareness in the GTA, the HSC emergency department experienced significantly reduced volumes of patients presenting with low-acuity problems. This decrease in patient volume together with the government's mandated suspension of services encouraged the use of alternative strategies (e.g., telephone consultation) to address nonurgent issues. This study not only provides information for future SARS-related public health preparedness policies, it may also provide a foundation for research into strategies other than emergency services to address nonurgent pediatric medical issues.
Footnotes
-
This article has been peer reviewed.
Contributors: Kathy Boutis supervised and contributed to the conception and design of the study, the acquisition of data, the drafting and critical revision of the manuscript for important intellectual content, and offered administrative, technical and support material. Derek Stephens and Kelvin Lam were responsible for statistical expertise analysis, interpretation of the data and critical revision of the manuscript for important intellectual content. Wendy Ungar contributed to the conception and design of the study, drafting and critical revision of the manuscript for important intellectual content. Suzanne Schuh contributed to the conception and design of the study, analysis and interpretation of the data, and critical revision of the manuscript for important intellectual content. All of the authors gave final approval of the submitted version.
Acknowledgements: We thank Martin Pecaric of Contrail Consulting Services for his work on database and graphic design.
Competing interests: None declared.
Correspondence to: Dr. Kathy Boutis, Division of Emergency Medicine, The Hospital for Sick Children, 555 University Ave., Toronto ON M5G 1X8; fax 416 813-5043; boutissympatico.ca
References
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Impact of adapting paediatric intensive care units for adult care during the COVID-19 pandemic: a scoping review
- Influence of epidemics and pandemics on paediatric ED use: a systematic review
- Service provision and utilisation in German paediatric primary care practices during public health crises: Protocol of the mixed-methods COVID-19 PedCare Study
- Patterns of presentations of children to emergency departments across Europe and the impact of the COVID-19 pandemic: retrospective observational multinational study
- 'Do I, dont I? A qualitative study addressing parental perceptions about seeking healthcare during the COVID-19 pandemic
- Impact of COVID-19 on Pediatric Emergency Department Visits: A Retrospective Cohort Study
- Paediatric ED utilisation in the early phase of the COVID-19 pandemic
More in this TOC Section
Similar Articles
Collections

