


Abstract
BACKGROUND: Transfer of patient care from an intensive care unit (ICU) to a hospital ward is often challenging, high risk and inefficient. We assessed patient and provider perspectives on barriers and facilitators to high-quality transfers and recommendations to improve the transfer process.
METHODS: We conducted semistructured interviews of participants from a multicentre prospective cohort study of ICU transfers conducted at 10 hospitals across Canada. We purposively sampled 1 patient, 1 family member of a patient, 1 ICU provider, and 1 ward provider at each of the 8 English-speaking sites. Qualitative content analysis was used to derive themes, subthemes and recommendations.
RESULTS: The 35 participants described 3 interrelated, overarching themes perceived as barriers or facilitators to high-quality patient transfers: resource availability, communication and institutional culture. Common recommendations suggested to improve ICU transfers included implementing standardized communication tools that streamline provider–provider and provider–patient communication, using multimodal communication to facilitate timely, accurate, durable and mutually reinforcing information transfer; and developing procedures to manage delays in transfer to ensure continuity of care for patients in the ICU waiting for a hospital ward bed.
INTERPRETATION: Patient and provider perspectives attribute breakdown of ICU-to-ward transfers of care to resource availability, communication and institutional culture. Patients and providers recommend standardized, multimodal communication and transfer procedures to improve quality of care.
The transfer of patients from the intensive care unit (ICU) to a hospital ward is one of the most challenging, high-risk and inefficient transitions of care because the patients are among the sickest in the health care system, they are transitioning from high technological units to less acute environments, and many interprofessional providers are involved in exchanges of information and responsibility. Challenges associated with transfers from ICU, including increased risk of medical errors,1 adverse events,2,3 readmission,4 dissatisfaction with care5 and death,6 have been previously described using primarily quantitative approaches.7 Understanding patient and provider perspectives is vital to guiding efforts to improve transfers from ICU to hospital ward. Previous studies have reported the experiences of individual provider groups (physicians or nurses)8,9 or patients10,11 at single health science centres.12,13 These assessments can inform local initiatives to improve quality targeted to individual stakeholder groups, but have limited transferability and cannot capture the complexity of interprofessional, multidisciplinary and patient-centred transfers of care.
A comprehensive joint assessment of key stakeholders’ perceptions of barriers and facilitators to high-quality transfers across multiple hospitals is needed to inform efforts at quality improvement more broadly. To address this knowledge gap, and to generate recommendations for how transfers of care from the ICU might be improved, we sought the perspectives of a diverse group of patients, their family members, and ICU and hospital ward physicians and nurses (providers) from multiple institutions.
Methods
Study design
This study was part of a multicentre prospective cohort study14 that used standardized surveys and case report forms to provide a 360-degree description of transfers from ICU to hospital ward in 10 hospitals in 7 cities across Canada. The study was conducted from July 2014 to January 2016. For each patient transfer in the study sample, we invited the patient, a family member and 4 providers directly involved in the transfer of care (1 ICU physician, 1 ICU nurse, 1 ward physician, 1 ward nurse) to participate in a survey to describe their experiences with the ICU to hospital ward transfer. Findings from the survey showed that failures of patient flow and communication are common, identifying a need for further qualitative inquiry into barriers and facilitators of high-quality patient transfers.14
Participants
Consecutive consenting patients who were transferred from the ICU to a hospital ward were enrolled in our cohort study. Participants from the cohort study who indicated interest in participating in a follow-up interview were considered for participation. We targeted recruitment of 4 participants (1 patient, 1 family member, 1 ICU provider, 1 ward provider) from each of the 8 English-speaking sites (n = 32) (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.170588/-/DC1) to develop our understanding of transfers of care across institutions further (Figure 1). We invited participants by email or telephone depending on contact information they provided when they indicated their interest in the follow-up interview. Although our team was prepared to expand recruitment if necessary, reviewers identified distinct recurring patterns in the data (i.e., barriers, facilitators and recommendations that were identified by participants) with no new themes emerging before the interviews concluded. Thus, no further recruitment was undertaken.15
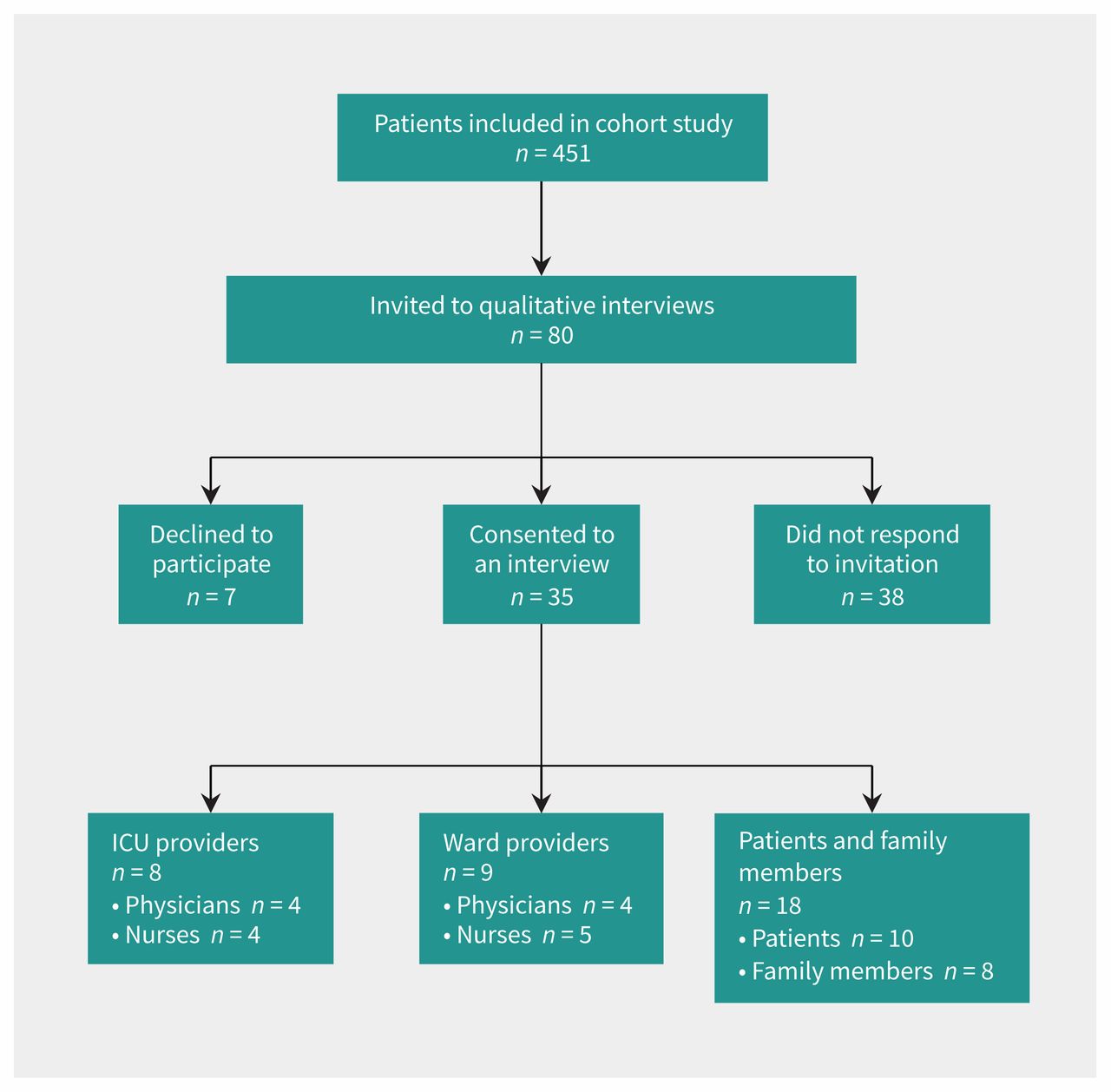
Flow diagram of selection of patients for interview.
Data collection
We developed the semistructured interview guide to explore stakeholder experiences with transfers of care from ICU to hospital ward. The interview guide was loosely informed by domains of inquiry identified in a stakeholder survey that we conducted as part of an earlier phase of this research program.14 The interview guide was pilot tested with 9 local stakeholders (4 providers, 5 patient or family members of patients) and refined based on their feedback. After obtaining informed consent from each participant, we (C.D. and Holly Wong, both with experience in conducting qualitative interviewing) conducted private semistructured telephone interviews in an office (Appendix 2, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.170588/-/DC1). The interviews were concluded by April 2016. Interviews posed questions about participants’ experiences with transfers of care between ICU and hospital ward and their perceptions of perceived barriers and facilitators to high-quality transfers. We audio-recorded and transcribed interviews verbatim.
Qualitative analysis
We used qualitative content analysis16 with Nvivo9 (www.qsrinternational.com/) to analyze interview transcripts and identify themes related to the needs and preferences of 3 categories of participant: patients and their family members, ICU providers (i.e., physicians and nurses), and ward providers (i.e., physicians and nurses) during the transition of care between ICU and hospital ward. Early in the data collection process, 2 experienced researchers (C.D., J.P.L.) analyzed a small sample of the transcripts (n = 5) independently and in duplicate to fracture the data using an open coding methodology,17 identify emerging themes and adjust interview questions and probes to ensure discussion of key themes in subsequent interviews. Researchers met to compare open coding and developed a codebook of emerging themes after they achieved agreement. Each investigator analyzed half of the remaining transcripts using open, axial and selective coding17 to expand and collapse themes. Researchers traded codebooks and analyzed remaining transcripts to ensure that key ideas were not missed. The codebook was iteratively refined using axial coding and finalized by 3 researchers (C.D., J.P.L., J.M.B.). Coded quotes were organized by theme, subtheme and participant type (patient or family member of patient, ICU provider, ward provider).
Ethics approval
The University of Calgary Conjoint Health Research Ethics Board approved this study (Ethics ID no. REB13–0021).
Results
We sent 80 invitations to individuals who had expressed an interest in being contacted for a potential interview. Of these, 35 consented, 7 declined and 38 did not respond. The mean duration of the interviews was 25 minutes (standard deviation: 11 min). Half (51%) of the participants were patients or family members, and the remainder (49%) were ICU and ward providers (Table 1). Nearly two-thirds of the participants (60%) were women (Table 1). Patients and family members were asked to speak about their recent transfer experience from ICU, and providers were encouraged to draw from any of their past experiences with transfers of care from ICU to ward.
Characteristics of participants
Analysis showed 3 overarching themes describing perceived barriers and facilitators to high-quality transfers of patients: resource availability, communication and institutional culture. Themes were common to all participant groups and characterized by subthemes to capture diversity of participant perspectives. Subthemes described by providers were process oriented (i.e., focused on process, protocol and outcomes), whereas subthemes described by patients and their family members reflected personal experiences. Exemplar quotations for subthemes are illustrated in Table 2 and Table 3.
Perceived facilitators and barriers to high-quality transfers from ICU to hospital ward, identified by providers
Perceived facilitators and barriers to high-quality transfers from ICU to hospital ward, identified by patients and families*
Overarching themes
1. Resource availability
Availability of resources was a theme that emerged in all participant groups. We define resource availability as the availability of both physical (e.g., bed) and human (e.g., nurses) resources at the levels of the individual patient (e.g., transfer form) and system (e.g., rushed transfer process owing to timing of breaks; Table 2 and Table 3). Provider concerns were consistent with those of patients and family members in 2 key areas: staff availability and material resources. Participants also described subthemes that were unique to their experiences as a provider (n = 4; e.g., transfer tools) or patient or family member of patient (n = 2; e.g., interprofessional collaboration).
2. Communication
Communication was a dominant theme among all participant groups. We define communication as all forms of consultation and documentation about the patient (e.g., verbal, written, text message, face to face, over the phone) as well as who was involved (provider–provider, provider–patient, provider–family) in these exchanges. Providers described subthemes (n = 4) that were largely focused on the importance of circumventing communication breakdowns during transfer from ICU to ward (e.g., multimodal communication), whereas patients and family members described subthemes (n = 4) related primarily to receiving timely and accurate information (e.g., communication aids).
3. Institutional culture
The concept of institutional culture was the third theme that emerged in all participant groups. We defined institutional culture as the norms, beliefs, values and customs that influence processes and protocols within hospital units (Table 2 and Table 3). Providers described subthemes (n = 3) focused on institutional norms that affected their work flow during transitions of care (e.g., importance placed on transfer by care teams), whereas patient and family subthemes (n = 4) concentrated on attitudes in the clinical environment that affected their sense of well-being during a time of vulnerability (e.g., humanization of patient–provider interactions).
Suggestions to improve transfers of care from ICU to ward
Participants were asked to provide suggestions for how to improve transfer from ICU to hospital ward (Table 4). The following were the most common suggestions provided by participants from more than half of the hospitals:
Implement standardized discharge communication tools to ensure continuity of communication between providers and patients or their families: Patients and providers across all sites stated that implementing a standardized discharge communication tool targeted to patient–provider communication would improve transfers by ensuring continuity of communication. Specific details of the content that should be included in this tool varied across the sites. For example, one provider highlighted the inclusion of the patient’s trajectory and journey in the ICU, whereas a provider at a different site stressed that the tool should prompt conversations about what patients and family members could expect on the ward. Regardless of detail, the perceived level of need for this type of instrument was echoed across participant groups.
Implement standardized discharge communication tools to ensure continuity of communication between providers: Both ICU and ward provider groups across the 8 study sites suggested implementing standardized discharge communication tools. Providers described the importance of discharge communication tools, such as electronic or paper-based tools that travel with the patient during transfer, and the types of information that should be included.
Use multimodal communication to document transfer and ensure continuity of care: Multimodal communication was suggested at 5 sites and across all participant groups. Participants described multimodal communication as verbal communication that is supported with written documentation.
Develop procedures for delays in patient transfer: ICU and ward providers at 5 sites suggested developing procedures to manage delays in patient transfer from ICU (i.e., patients who wait for days for a ward bed). Providers agreed that care must be coordinated and advanced during this period and the patient’s readiness for transfer reassessed daily.
Suggestions to improve transfers from ICU to hospital wards
Interpretation
Patient transfers from the ICU are complex events that can disrupt continuity of patient care,2–4,6 yet little is known about the experiences of key stakeholders. Our study provides a multicentre qualitative report of patient, family member, ICU and ward provider perspectives of why transfers of care break down, and how they can be improved to enhance quality of care and improve stakeholder experiences. The in-depth description of stakeholder experiences with transfers of care presented here adds to the existing literature on transfers of care that has largely been developed using quantitative methods.7,12,18 Main findings of the study include the shared assignment by diverse stakeholders of resource availability, communication and institutional culture as main drivers in the breakdown of transfers of care from ICU to ward, and the call for standardized, multimodal communication and transfer procedures to improve quality of care.
Resource availability
Material and human resources were highlighted by participants as both facilitators (i.e., when available) and barriers (i.e., when lacking) to high-quality transfers of care. Previous studies have shown that bed availability can negatively affect transfers from ICU when patients are transferred before they otherwise would be (e.g., owing to an influx of more acute patients).19,20 Conversely, participants in our study also cited long transfer processes as a barrier to high-quality transfers where patients ready for transfer waited days for a hospital ward bed to become available. They reported variable quality of care during this “waiting period” with confusion or a lack of accountability about who is most responsible for the patient.21,22 Health care organizations that have flow failure (i.e., inefficient movement of patients)23 must develop procedures to minimize transfer delays (e.g., mimic just-in-time manufacturing)24 and strategies to ensure patients receive coordinated care while awaiting transfer (e.g., co-management or graduated management).
Communication
Patients, family members and providers described the importance of using multiple modes of communication to support the exchange of information during transfers of care. Verbal and written communication types serve different purposes. Verbal communication can be used to ensure that accurate information is exchanged in a timely manner, but written communication can ensure the durability of patient information over time, preserving the “patient’s story” for all relevant stakeholders (i.e., current status, relevant history, patterns that emerged during care, and future-oriented care plan).25 It is not surprising that patients recovering from a severe illness26 and family members who are under stress may have difficulty remembering details and retaining verbal information.9 Electronic health records that make information27 available to a broad group of stakeholders may provide a platform for multimodal communication.28 For example, some electronic health records have developed mediums for patient–provider communication such as online portals,29 email30 and instant messaging.31 Although promising, concerns remain about confidentiality breaches when using electronic portals to communicate patient information,32 confusion or anxiety when patient information is accessed in the absence of a care provider, 26 and the potential impact on the frequency and length of face-to-face patient–provider interactions.33
Institutional culture
Reconceptualizing the relative importance of transfers of care from ICU to hospital ward (i.e., where transfers are understood as critical to maintaining the continuity of patient care and are prioritized by sending and receiving care teams) was identified as a key facilitator to high-quality transfers.34 What is more, patient- and family-centred care was a facilitator of high-quality ICU transfers. This is important because health care cultures that promote the active involvement of patients and families in partnered care have been shown to alleviate communication barriers, 35 increase psychological well-being,36 preserve continuity of care,35 and improve patient and family perceptions of care received.37 Partnering with patients and their family members during transfers of care from ICU to ward should be considered a high priority by both sending and receiving care teams. To improve transfers of care, they must be recognized as institutional priorities in which patients, patient families and providers all play key roles.
Limitations
There are limitations to consider when interpreting the findings of our study. First, some participants were interviewed up to 2 years after the relevant ICU admission and, thus, recall bias38 might have affected their recollection of events. It is also possible that some perspectives may have been missed, given that participants may have been motivated to interview as a result of a mostly positive or mostly negative experience. Second, this study is limited to the perspectives of providers most responsible for patient care (i.e., physician and nurse) and did not capture the perspectives of other provider groups (e.g., social workers). Nevertheless, the scope of our sample (i.e., perspectives from 6 key stakeholder groups collected from 8 diverse hospital settings across 7 cities and 3 health systems), as well as the distinct likeness of reported perceived barriers, facilitators and recommendations, lead us to believe that our results are applicable to units across the country as factors worth considering in their specific institutional context.
Conclusion
Transitions of care between the ICU and hospital ward are challenging and high risk. Key stakeholders describe 3 overarching themes perceived as barriers or facilitators to high-quality patient transfers: resource availability, communication and institutional culture. Patients and providers have distinct (e.g., process- vs. experience-oriented) but largely overlapping perspectives. They suggest implementing standardized multimodal communication and procedures to manage common delays in patient transfer.
Acknowledgements
The authors thank Denise Buchner for her support in developing the interview guide and providing supervision in the collection of data, and Holly Wong for help in conducting interviews. At the time of publication, Jeanna Parsons Leigh is affiliated with the Department of Medicine, Schulich School of Medicine and Dentistry, and Division of Critical Care Medicine, Western University, London, Ont.
Footnotes
Competing interests: Sean Bagshaw reports personal fees from Baxter Healthcare, outside the submitted work. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Chloe de Grood and Jeanna Parsons Leigh collected and analyzed data and drafted the manuscript; they contributed equally to the work. Sean Bagshaw, Robert Fowler, Peter Dodek, Alan Forster, Jamie Boyd interpreted the data and critically revised the manuscript for important intellectual content. Henry Stelfox designed the study, interpreted the data, drafted and critically revised the manuscript. All authors read and approved the final version to be published and agreed to be accountable for all aspects of the work.
Funding: Technology Evaluation in the Elderly Network grant number CORE 2013-12A supported this work. Robert Fowler was supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial Office. Sean Bagshaw was supported by a Canada Research Chair in Critical Care Nephrology. Henry Stelfox was supported by a Population Health Investigator Award from Alberta Innovates and an Embedded Clinician Researcher Award from the Canadian Institutes of Health Research.
- Accepted March 9, 2018.
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

