

Abstract
Background: In clinical trials, cholesterol-lowering medications have been proven to decrease mortality and morbidity and are strongly recommended as secondary prevention for patients with established coronary artery disease. Whether physicians and patients follow this recommendation is unknown. Our objective was to determine the rate at which patients fill at least one prescription for cholesterol-lowering medications after coronary revascularization.
Methods: Using the computerized administrative databases of the Régie de l'assurance maladie du Québec, we identified all elderly patients (older than 65 years) who had a coronary revascularization procedure (percutaneous coronary intervention or coronary artery bypass graft) between Apr. 1, 1995, and Dec. 31, 1997, and who survived until hospital discharge. We also determined the percentage of these patients who filled one or more prescriptions for cholesterol-lowering drug therapy before Dec. 31, 1999, or death, whichever date came first. We used multivariate logistic regression models to examine the independent associations between filling a prescription for a cholesterol-lowering drug, patient characteristics and the type and year of coronary revascularization.
Results: We identified 11 958 elderly patients who had a coronary revascularization between Apr. 1, 1995, and Dec. 31, 1997. During a follow-up period that averaged 3 years, 4443 (37.2%) patients did not fill a prescription for a cholesterol-lowering medication. Patients who were male, of advanced age, who had diabetes or congestive heart failure were less likely to fill a prescription for a cholesterol-lowering medication. Patients whose initial revascularization procedure was coronary artery bypass grafting were also less likely than those who had angioplasty to start cholesterol-lowering medication (relative risk [RR] 0.77, 95% confidence interval [CI] 0.73 – 0.81). Use of cholesterol lowering medications before the revascularization procedure was very strongly associated with future drug use (RR 7.20, 95% CI 6.83–7.58).
Interpretation: In this population-based study of revascularized patients, we observed a substantial underutilization of cholesterol-lowering medications after revascularization. Our observations suggest an important role for continuity of care in the treatment of cardiovascular patients undergoing revascularization procedures.
The important role of cholesterol in the development of coronary atherosclerosis has been appreciated for decades.1,2,3 Epidemiologic data were so compelling that national guidelines have encouraged lipid-lowering therapy for the treatment of people at high risk since the early 1990s.4 Subsequently, randomized clinical trials5,6,7,8 have affirmed the soundness of this secondary prevention, even for those who have coronary revascularization.9,10
Coronary revascularization procedures are widely used to treat coronary artery disease and have been shown to improve quality of life and longevity in specific situations. As the population ages and indications expand, more revascularization procedures are performed each year. Patients who undergo coronary revascularization, particularly the elderly, nevertheless remain at high risk of repeat coronary events. Therefore, according to current guidelines,4 this group should be targeted for secondary prevention strategies.
The goals of this study were to determine the rate and predictors of the filling of one or more cholesterol-lowering drug prescriptions in a well-defined cohort of elderly patients who had recently undergone coronary revascularization.
Methods
We conducted this population-based study with data from the computerized administrative databases of the Régie de l'assurance maladie du Québec. These databases were developed in the context of the universal health insurance program provided to all residents of Quebec, Canada, and capture all physician visits, procedures, hospitalizations, outpatient prescription drugs dispensed and vital status. Outpatient prescription data include information on the nature, quantity, strength, dosage and dispensing date of all drugs. The hospital database contains information on all in-hospital procedures as well as patient demographics, admission and discharge dates, and up to 15 discharge diagnoses coded with the 9th revision of the International Classification of Diseases (ICD-9).
All databases were linked through the use of a unique and anonymous identifier, thereby creating a longitudinal history of each patient's clinical outcomes and patterns of drug use after their revascularization procedure. The prescription drug database is complete only for those over the age of 65. Cohort entry was defined as the discharge date for the hospitalization that included the revascularization procedure.
We followed patients from the first revascularization procedure they had during the period Apr. 1, 1995, to Dec. 31, 1997, until Dec. 31, 1999, or until they died, whichever came first. Patients may have had previous revascularization procedures before Apr. 1, 1995. The only patients excluded from the cohort were those less than 65 years of age at the time of their revascularization procedure, non-Quebec residents and those who died in the hospital during their initial revascularization.
We confirmed the validity of the physician services dataset that we used to identify revascularized patients by cross-linking with the hospital admission and discharge dataset. We were unable to locate a corresponding hospital record for less than 1% of patients, and these cases were discarded. The reliability of the hospital administrative databases in recording the number of coronary revascularizations has been previously validated.11 Moreover, the coding accuracy of primary and secondary discharge diagnoses in the Quebec hospitalization database for elderly persons with cardiovascular disorders has also been demonstrated,12 as has the accuracy of the pharmaceutical database.13
The primary outcome measure was the dispensing of a cholesterol-lowering drug prescription, and we defined exposure as patients who filled at least 1 prescription after their revascularization procedure.
We analyzed the univariate associations of numeric and categorical variables with the post-revascularization use of cholesterol-lowering medications with t-tests and 𝛘2 respectively. We developed fully adjusted multivariate logistic regression models to assess the independent associations between the start of cholesterol-lowering drug use and patient demographics, geographic region, year and type of coronary revascularization, disease severity, comorbidities, use of other medications and the intensity of medical follow-up. We used the incidence of previous myocardial infarction and congestive heart failure as markers of disease severity. We assessed the severity of the associated comorbidities collectively with the Charlson index,14 a weighted index of the seriousness of hospital diagnoses that has previously been validated.
Results
Between Apr. 1, 1995, and Dec. 31, 1997, 31 520 patients had a revascularization procedure and 12 759 were aged 65 years or older when they had their first procedure. We excluded 661 (5%) who died in hospital and a further 140 (1%) patients for whom it was impossible to locate complete records, leaving a final cohort of 11 958 patients.
The baseline characteristics of these patients are given in Table 1. The average age was 71 years (standard deviation 4.7, range 65 to greater than 85) and 64.6% were males. As expected, diabetes, hypertension and prior myocardial infarctions were highly prevalent conditions. The initial revascularization procedure was percutaneous coronary intervention (angioplasty) in 5385 patients and bypass surgery (coronary artery bypass grafting) in 6573. In the 3 months before their coronary revascularizations, 3698 patients (31%) had filled a prescription for cholesterol-lowering medications.
Table 1.
The total number of patients who filled at least one prescription for a cholesterol-lowering medication after their initial revascularization procedure was 7515 (62.8%), including 4033 (33.7%) who were new users. The median time to filling the first prescription after revascularization was less than 1 month for continuing users, but was over 8 months for new users. For most (6613) patients (88%) their first prescription was for a statin. There were 4227 patients (35.4% of the total cohort) who never filled a prescription for any cholesterol-lowering medication, and 216 (1.8%) patients who had used a cholesterol-lowering medication before their revascularization did not, at any time after the procedure, refill a prescription. Therefore, during an average follow-up period of over 3 years after their revascularization procedure, 4443 (37.2%) did not fill a single prescription for cholesterol-lowering therapy.
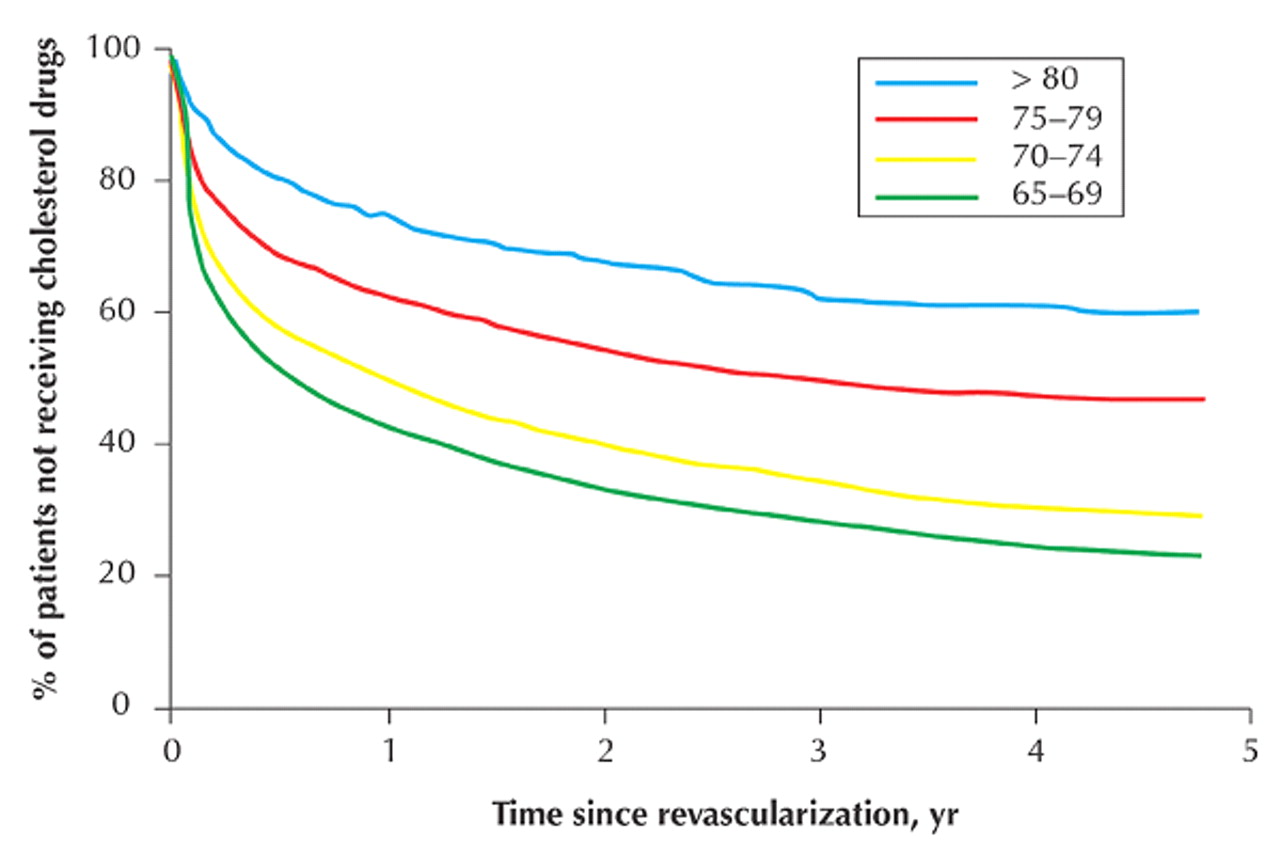
Non-users generally had a higher risk profile than users, with increased disease severity, more comorbid illness and more advanced age (Table 1). We identified several variables that were independently associated with the dispensing of a cholesterol-lowering drug after revascularization (Table 2). Men were less likely to fill a prescription (relative risk [RR] 0.87, 95% confidence interval [CI] 0.83–0.92). There was a strong inverse relationship between drug exposure and increasing age (Fig. 1). For example, patients between 75 and 79 years old were 39% (95% CI 35%–43%) less likely to be treated than the reference group of patients aged 65 to 69 years. Patients whose initial revascularization procedure was bypass surgery were less likely to be treated than those undergoing angiography (RR 0.77, 95% CI 0.73–0.81). Higher risk patients with diabetes (RR 0.89, 95% CI 0.84–0.94) and congestive heart failure (RR 0.81, 95% CI 0.76–0.87) were also less likely to be treated. Prior use of cholesterol-lowering medications was very strongly associated with future drug use (RR 7.20, 95% CI 6.83–7.58). Patients who entered the cohort more recently had an increased chance of receiving therapy (p = 0.02). Those patients with hypertension, previous myocardial infarction, prior use of aspirin and an increased Charlson score were no more likely to fill a cholesterol drug prescription than those without these conditions.
Table 2.
{kind=link}
Fig. 1: Patients not receiving cholesterol-lowering medication after initial revascularization as a function of age.
Interpretation
We have demonstrated an important underutilization of cholesterol-lowering medications among patients who have had revascularization procedures despite guidelines, published before the inception of this cohort, that emphasize that similar high-risk patients are suitable candidates for drug therapy.4 There is a pronounced association of underutilization with increasing age. Whether patients used prescriptions for cholesterol-lowering medication before coronary revascularization was the best marker of whether they would start using them again after the procedure. This suggests an important role of continuity of care in overall quality of care.
As early as 1994, practice guidelines supported by the large randomized 4S trial5 argued for secondary prevention of adverse coronary events by lowering cholesterol. A natural question is why the drug patterns observed in this study do not seem to conform to these standards. The improving prescribing patterns observed over the period of the study suggest that perhaps physicians were awaiting additional scientific evidence. A meta-analysis published only late in the follow-up period did confirm these advantages for elderly patients.15
It is disconcerting to note that patients with the highest risk of death or myocardial infarction (the very elderly, those with diabetes and those with congestive heart failure) are the same patients who have the lowest likelihood of receiving cholesterol-lowering medications. Recent trials published after the time period of this study have confirmed the benefits of extending cholesterol-lowering therapy to the elderly.16,17 The elderly have previously been identified as a patient group prone to underutilization of other proven cardiac therapies.18 It is odd that a medical system appears willing to provide invasive and expensive revascularization techniques, without compelling evidence of benefit in the very elderly, but seems less eager to follow up with a proven low-technology intervention such as cholesterol-lowering drug therapy.
Is it possible that this underutilization of a proven therapy is a phenomenon restricted to our study area? This appears unlikely because studies19,20,21 in other countries have also shown a low prevalence of secondary prevention with lipid-lowering drugs in other populations. Moreover, Quebec physicians have been shown22 to follow evidence-based medicine at least as readily as their American colleagues, if not more so. However, to further clarify this issue, others may consider examining this question in their local region or country.
Our study does have some potential limitations. First, we chose an inaugural prescription as our primary endpoint because we were interested in assessing the intent to introduce this therapy. Our data would not permit an adequate ascertainment of the interplay of physicians' or patients' characteristics ( e.g., cost, side effects) that might influence long-term adherence. Although compliance was, therefore, not assessed in this study, it is clearly an important issue because low adherence rates have been observed previously in elderly populations.23,24 Second, we have no biochemical lipoprotein measurements. However, local and international evidence 25,266 suggests that the great majority of revascularized patients have clinically significant dyslipidemias that need pharmacologic treatment according to current guidelines. As well, the suggestion that the pleiotropic properties of statins (improving endothelial function, diminishing inflammation and improving plaque stability) are important further argues that virtually all revascularized patients should be treated regardless of their cholesterol level.17 Third, we have information only on the dispensing of drugs, not on actual prescription rates.
In conclusion, this study has shown an underutilization of cholesterol-lowering therapy in a cohort of revascularized elderly patients. We have identified subgroups who are especially likely to be neglected. Continuity of care is likely to be an important process in assuring improved quality of drug therapy in this population. Although some improvement in prescription patterns was observed over time, more research is needed to confirm and extend these findings. A simple approach to addressing this identified gap in care may be to systematically introduce cholesterol-lowering drugs on hospital discharge and to later reassess the need for long-term continuation.
Footnotes
-
This article has been peer reviewed.
Contributors: All authors contributed fully to the design and conduct of the study.
Acknowledgements: Dr. Brophy receives financial support from le Fonds de la Recherche en Santé du Québec. Dr. Brassard is a Canadian Institutes of Health Research (CIHR) funded scholar. This study was funded by the Réseau d'utilisation des médicaments du Fonds de la Recherche en Santé du Québec. Although data were provided by the Régie de l'assurance maladie du Québec and by the Ministère de la santé et des services sociaux du Québec, the statements contained herein do not necessarily represent those of the Quebec government.
Competing interests: None declared.
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.