

Abstract
Portal hypertension is one of the main consequences of cirrhosis. It results from a combination of increased intrahepatic vascular resistance and increased blood flow through the portal venous system. The condition leads to the formation of portosystemic collateral veins. Esophagogastric varices have the greatest clinical impact, with a risk of bleeding as high as 30% within 2 years of medium or large varices developing. Ascites, another important complication of advanced cirrhosis and severe portal hypertension, is sometimes refractory to treatment and is complicated by spontaneous bacterial peritonitis and hepatorenal syndrome. We describe the pathophysiology of portal hypertension and the current management of its complications, with emphasis on the prophylaxis and treatment of variceal bleeding and ascites.
Portal hypertension is one of the main consequences of cirrhosis. It can result in severe complications, including bleeding of esophagogastric varices as well as spontaneous bacterial peritonitis or hepatorenal syndrome as complications of ascites. We describe in brief the pathophysiology of portal hypertension and review the current management of its complications, with emphasis on variceal bleeding and ascites.
Pathophysiologic background
Portal hypertension
Portal hypertension is defined as an increase in blood pressure in the portal venous system. The portal pressure is estimated indirectly by the hepatic venous pressure gradient — the gradient between the wedged (or occluded) hepatic venous pressure and the free hepatic venous pressure. A normal hepatic venous pressure gradient is less than 5 mm Hg.
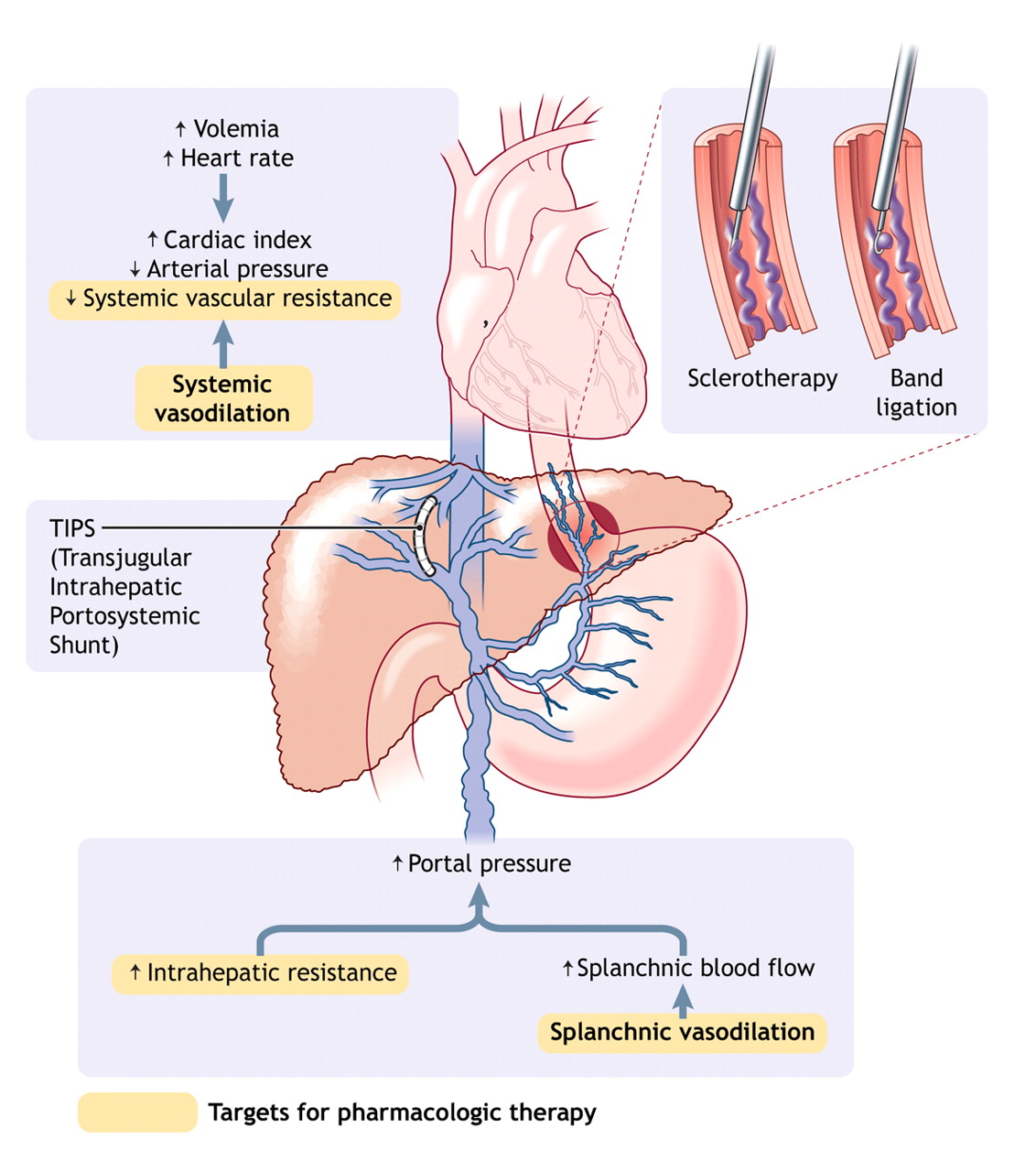
In cirrhosis, portal hypertension results from the combination of increased intrahepatic vascular resistance and increased blood flow through the portal venous system (Fig. 1). According to Ohm's law, portal venous pressure (P) is the product of vascular resistance (R) and blood flow (Q) in the portal bed (P = Q × R). Intrahepatic resistance increases in 2 ways: mechanical and dynamic. The mechanical component stems from intrahepatic fibrosis development; various pathologic processes are thought to contribute to increased intrahepatic resistance at the level of the hepatic microcirculation (sinusoidal portal hypertension): architectural distortion of the liver due to fibrous tissue,1 regenerative nodules,1 and collagen deposition in the space of Disse.2 The dynamic component results from a vasoconstriction in portal venules secondary to active contraction of portal and septal myofibroblasts, to activated hepatic stellates cells and to vascular smooth-muscle cells.3–5 Intrahepatic vascular tone is modulated by endogenous vasoconstrictors (e.g., norepinephrine, endothelin-1, angiotensin II, leukotrienes and thromboxane A2) and enhanced by vasodilators (e.g., nitric oxide). In cirrhosis, increased intrahepatic vascular resistance results also from an imbalance between vasodilators and vasoconstrictors.6
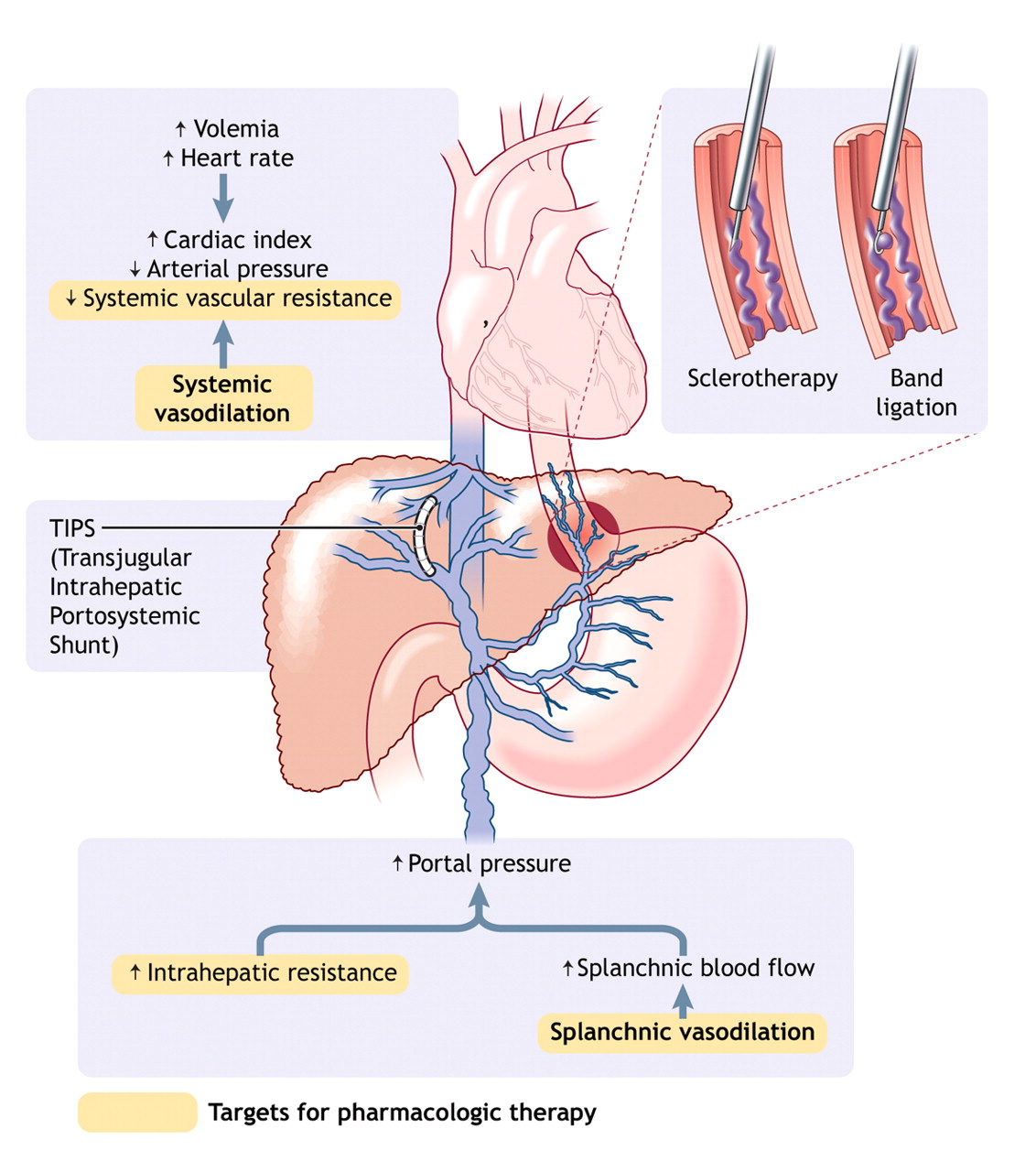
Fig. 1: Pathophysiology of portal hypertension in cirrhosis. Portal hypertension results from increased intrahepatic vascular resistance and portal–splanchnic blood flow. In addition, cirrhosis is characterized by splanchnic and systemic arterial vasodilation. Splanchnic arterial vasodilation leads to increased portal blood flow and thus elevated portal hypertension. An increased hepatic venous pressure gradient leads to the formation of portosystemic venous collaterals. Esophagogastric varices represent the most clinically important collaterals given their associated high risk of bleeding. Treatment consists of pharmacologic therapy to decrease portal pressure, endoscopic treatment of varices (band ligation or sclerotherapy) to treat variceal bleeding, and creation of a transjugular intrahepatic portosystemic shunt (TIPS) to reduce portal pressure if drug therapy and endoscopic treatment fail. Photo by: Lianne Friesen and Nicholas Woolridge
Portal hypertension is characterized by increased cardiac output and decreased systemic vascular resistance,7 which results in a hyperdynamic circulatory state with splanchnic and systemic arterial vasodilation. Splanchnic arterial vasodilation leads to increased portal blood flow, which in turn leads to more severe portal hypertension. Splanchnic arterial vasodilation results from an excessive release of endogenous vasodilators such as nitric oxide, glucagon and vasointestinal active peptide.
An increase in the portocaval pressure gradient leads to the formation of portosystemic venous collaterals in an attempt to decompress the portal venous system. Esophageal varices, drained predominantly by the azygos vein, are clinically the most important collaterals because of their propensity to bleed. Esophageal varices can develop when the hepatic venous pressure gradient rises above 10 mm Hg.8–10 All factors that increase portal hypertension can increase the risk of variceal bleeding, including deterioration of liver disease,11 food intake,12,13 ethanol intake,14 circadian rhythms,15 physical exercice16 and increased intra-abdominal pressure.17 Factors that alter the variceal wall, such as ASA and other NSAIDs, could also increase the risk of bleeding.18,19 Bacterial infection can promote initial and recurrent bleeding.20
Ascites and hepatorenal syndrome
In advanced cirrhosis, splanchnic arterial vasodilation promoted by portal hypertension is pronounced and leads to the impairment of systemic and splanchnic circulation.21 Systemic vasodilation leads to relative hypovolemia, with a decrease in effective blood volume and a fall in mean arterial pressure. States of homeostasis and antinatriuresis are activated to maintain arterial pressure, which results in sodium and fluid retention.21 In addition, a combination of portal hypertension and splanchnic arterial vasodilation alters splanchnic microcirculation and intestinal permeability, facilitating the leakage of fluid into the abdominal cavity.21 As cirrhosis progresses, the kidneys' ability to excrete sodium and free water is impaired; sodium retention and ascites develop when the amount of sodium excreted is less than the amount consumed.21 Decreased free water excretion leads to dilutional hyponatremia and eventually to impaired renal perfusion and hepatorenal syndrome.21
Variceal bleeding
Variceal bleeding is a medical emergency associated with high rates of recurrence and death.22–25 Its management is based on specific treatments, including pharmacologic therapy, endoscopic treatment and antibiotic therapy.
Pharmacologic therapy
Vasopressin and its analogue terlipressin: Vasopressin is a potent splanchnic vasoconstrictor; however, its use was abandoned 25 years ago in most countries because of its severe vascular side effects. Terlipressin, a vasopressin analogue not currently licensed for use in Canada, has similar effects,26 reducing the hepatic venous pressure gradient, variceal pressure and azygos blood flow.27,28 Terlipressin has been found to be superior to placebo in the control of variceal bleeding.29 It has also been found to decrease renal vasoconstrictor system activity and improve renal function in patients with hepatorenal syndrome.30–33 However, terlipressin can induce ischemic complications, particularly in cases of severe hypovolemic shock,34 and it is contraindicated in patients with cardiovascular disease (arterial disease with severe obstruction, cardiac insufficiency, arrhythmias, hypertension).
Somatostatin and its analogues octreotide and vapreotide: Somatostatin significantly reduces the hepatic venous pressure gradient,35–37 variceal pressure38 and azygos blood flow;36 however, because its hemodynamic effect is transient, continuous infusion is required.36 Four placebo-controlled studies showed contrasting results. Somatostatin was more effective than placebo in controlling variceal bleeding,39,40 but its effectiveness in reducing the need for transfusion41,42 and balloon tamponade41 remains unproven. Terlipressin appears to be as effective as somatostatin in the control of bleeding.29
Octreotide and vapreotide have a longer half-life than somatostatin and are useful in the management of portal hypertension. Octreotide decreases the hepatic venous pressure gradient and azygos blood flow43–46 but not variceal pressure.27,47 However, the effect of octreotide is transient43–46 and controversial.48 It prevents the increase in hepatic blood flow after a meal,49 and it seems to be as efficient as terlipressin in treating variceal bleeding and in improving the efficacy of endoscopic therapy.50–52 Only one double-blind randomized controlled trial of octreotide has been published (in brief) to date, and it showed that octreotide was not more effective than placebo in controlling and preventing early recurrent variceal bleeding.53 In a randomized controlled trial, vapreotide, a long-acting analogue of somatostatin not currently licensed for use in Canada, was administered before endoscopic treatment and was found to result in fewer blood transfusions and better control of bleeding than endoscopic treatment alone.54
No major toxic effects and practically no complications are associated with the use of somatostatin or its analogues.
Endoscopic diagnosis and treatment
Endoscopy is useful in the diagnosis and treatment of bleeding esophagogastric varices. Three endoscopic techniques are currently used: endoscopic band ligation, endoscopic sclerotherapy and variceal obturation with glue.
Endoscopic band ligation: Currently, endoscopic band ligation is the first choice of endoscopic treatment for esophagogastric varices. The procedure involves placing an elastic band on a varix, which allows aspiration of the varix in a cylinder attached to an endoscope. A maximum of 5–8 elastic bands should be used per session. Sessions should be performed every 2–3 weeks until the varices have been obliterated or have become so small that ligation is impossible.55 Complications of endoscopic band ligation are fewer than those with endoscopic sclerotherapy. Generally, bleeding from a post-ligation ulcer is moderate.56
Endoscopic sclerotherapy: There are several sclerosant agents (polidocanol, ethanolamine, ethanol, tetradecyl sulfate and sodium morrhuate), and they provide similar results. The treatment involves intravariceal or paravariceal injections of the sclerosant agent (total volume 10–30 mL per session) every 1–3 weeks until the varices have been obliterated.56 Given that varices recur in 50%–70% of cases,57 surveillance endoscopy every 3–6 months is required.57,58 Frequent complications of endoscopic sclerotherapy are retrosternal pain, dysphagia and postsclerotherapy bleeding ulcers. More severe complications, such as esophageal perforation or stricture, have been reported.56
Variceal occlusion with glue: This treatment is especially useful in patients who have had gastric or gastroesophageal variceal bleeding. It consists of embolization of varices by injecting them with the tissue adhesive N-butyl-2-cyanoacrylate; the adhesive polymerizes in contact with blood. One millilitre of adhesive is injected at a time, with a maximum of 3 injections per session. The most serious risk associated with this procedure is embolization of the lung, spleen or brain.59
Transjugular intrahepatic portosystemic shunt
Percutaneous creation of a transjugular intrahepatic portosystemic shunt (TIPS) through a jugular route connects the hepatic and portal veins in the liver. The goal is to reduce portal pressure and thus prevent variceal bleeding.60 TIPS diverts portal blood flow from the liver, but it increases the risk of encephalopathy.61–63 In most cases encephalopathy responds to standard therapy, but in some cases the calibre of the shunt has to be reduced;60 rarely, when encephalopathy does not respond to treatment (in 5% of cases) the shunt should be occluded.60 Thrombosis and stenosis are other complications that can cause TIPS dysfunction.60 Recently, it has been reported that the use of a polytetrafluoroethylene-covered stent decreases the rate of shunt dysfunction.64 The putative increased risk of hepatocellular carcinoma remains to be clarified.
Other treatment options
Balloon tamponade: In cases of massive or uncontrolled bleeding, balloon tamponade provides a “bridge” to definitive treatment with TIPS or portosystemic surgical shunt.55,65 The most frequently used balloon is the 4-lumen modified Sengstaken–Blakemore tube, which employs a gastric and esophageal balloon.56 In cases of bleeding gastric varices, use of the Linton–Nachlas tube with a large gastric balloon is recommended.56
Portosystemic surgical shunt: Its usefulness has dramatically decreased since the advent of TIPS. Moreover, the procedure requires an experienced surgeon. In cases of refractory bleeding and when TIPS is technically impossible, creation of a nonselective portosystemic shunt may be suitable in patients with cirrhosis provided that the liver dysfunction is not too severe (Child–Pugh class A or B, Appendix 1).
Practical management
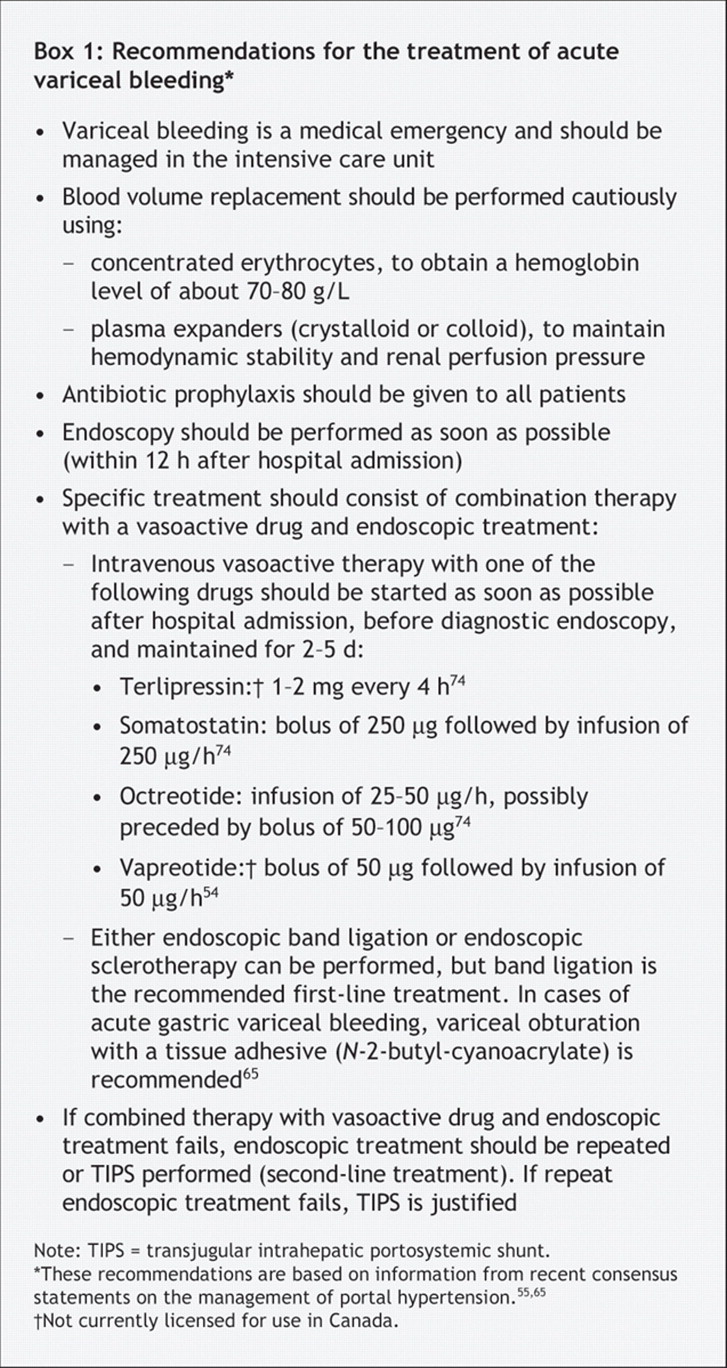
Variceal bleeding should be managed in an intensive care unit.55 Treatment should include nonspecific therapy, such as blood volume replacement and antibiotic prophylaxis, as well as specific treatments, such as pharmacologic therapy and endoscopic treatment (Box 1, Fig. 2).

Fig. 2: Algorithm for the treatment of variceal bleeding. TIPS = transjugular intrahepatic portosystemic shunt. *The therapeutic option depends on what was done in primary prophylaxis.
Nonspecific treatment
Nonspecific treatment aims to correct hypovolemia and to prevent complications. Blood volume replacement should be done cautiously using concentrated erythrocytes to obtain a hemoglobin level of about 70–80 g/L.55,65 Overtransfusion should be avoided given the risk of increased portal pressure37,66,67 and continued or recurrent bleeding.68 Plasma expanders are used to maintain hemodynamic stability and renal perfusion pressure.55,65 Either a crystalloid (isotonic saline solution) or colloid solution can be used, but a crystalloid solution is preferred because it is harmless.55
Infection occurs in 25%–50% of patients with cirrhosis and gastrointestinal bleeding.69 Failure to control bleeding and rates of death are increased in infected patients.69,70 The early administration of antibiotic prophylaxis will benefit all patients with variceal bleeding and improve survival.55,65,71,72 One recommended protocol is oral administration of norfloxacin (400 mg twice daily for 7 days).55,73
The routine use of a nasogastric tube is not recommended. Patients with encephalopathy should be given lactulose;65 however, insufficient information exists to recommend its use in the prevention of hepatic encephalopathy.55,65
Specific treatment
Intravenous therapy with a vasoactive drug should be started as soon as possible following hospital admission, before diagnostic endoscopy, and maintained for 2–5 days (Box 1).54,55,65,74 Vasopressin is not recommended because of its deleterious side effects.
Endoscopy should be performed within 12 hours after hospital admission on an empty stomach, which can be achieved by either intravenous injection of erythromycin (250 mg begun 30–60 minutes before endoscopy) or lavage through a nasogastric tube.55,65 Endoscopy is useful in confirming the source of bleeding and allowing hemostatic treatment. Either endoscopic band ligation or endoscopic sclerotherapy may be used.55,65 However, endoscopic band ligation is the recommended first-line treatment.65 In patients who have bled from gastric or gastroesophageal varices, endoscopic obliteration with the tissue adhesive N-butyl-2-cyanoacrylate should be performed.65 However, endoscopic band ligation is also possible to treat gastroesophageal varices.
If combined vasoactive and endoscopic therapy fails, a second attempt at endoscopic therapy is justified if the bleeding is mild and the prognosis not compromised.55,65,75 TIPS is a second-line treatment option.65 Balloon tamponade can be used as a “bridge” in cases of massive bleeding.55,65 If bleeding persists or compromises prognosis, TIPS or surgical shunt creation should be offered as a rescue therapy.55,65
Esophagogastric varices
At present, there is no satisfactory nonendoscopic indicator to detect the presence of esophagogastric varices.65,76 Endoscopic screening is the best technique.76,77 The goal of management is to prevent variceal bleeding. This is achieved in 3 ways: by preventing the development of varices (preprimary prophylaxis), by preventing a first variceal bleeding episode once varices have developed (primary prophylaxis) and by preventing recurrent bleeding (secondary prophylaxis) (Fig. 3).
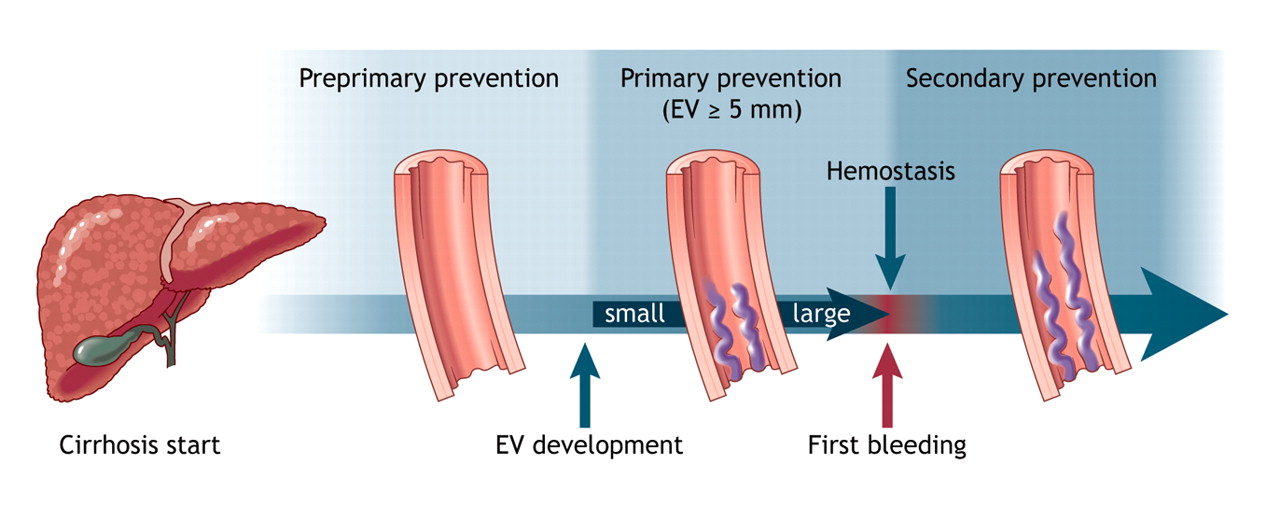
Fig. 3: Prophylaxis of variceal bleeding in cirrhosis. Preprimary prophylaxis is aimed at preventing esophagogastric varices (EV) from developing. The goal of primary prophylaxis is to prevent a first variceal bleeding episode once medium or large varices have formed. Secondary prophylaxis is used to prevent recurrent variceal bleeding. Photo by: Lianne Friesen and Nicholas Woolridge
Pharmacologic therapy
Pharmacologic therapy is used to control and prevent variceal bleeding. The 2 classes of drugs used are β-blockers and nitrates.
β-Blockers: β-Blockers lower portal pressure by reducing portal blood flow. The blood flow is reduced as a consequence of decreased cardiac output (β1 receptor blockade) and arteriolar splanchnic vasoconstriction by an unopposed α-vasoconstrictive effect (β2 receptor blockade).78 Nonselective β-blockers such as propranolol, nadolol and timolol are more effective than selective β1-blockers in reducing the hepatic venous pressure gradient.79,80 The median reduction of the gradient by nonselective β-blockers is about 15%.79,81–84 Nonselective β-blockers reduce variceal pressure85 and azygos blood flow86–88 even in patients who do not exhibit a marked decrease in the hepatic venous pressure gradient (propranolol “nonresponders”).87,89 Propranolol has been found to prevent increases in portal pressure related to physical exercise in patients with cirrhosis90 and to decrease the rate of bacterial translocation.91 It has also been found to reduce postprandial peak in portal pressure;92 however, this effect with long-term use was not confirmed in 2 recent trials.93,94
It has been suggested that the hepatic venous pressure gradient could be measured to evaluate the efficiency of β-blocker treatment.95 Several studies have shown that variceal bleeding does not occur if the gradient is reduced to below 12 mm Hg81,96 or that bleeding occurs at a low rate if the gradient is reduced by at least 20% of the basal value.96–99 However, the prognostic value of the hepatic venous pressure gradient on survival is still controversial.100,101 Besides, the measurement of the gradient is invasive and not cost-effective; its use is not recommended in clinical practice and is limited to selected hospitals.76
Nitrates: The mechanism of the vasodilatory effects of nitrates — vascular tone reduction and decreased intrahepatic resistance — is not completely understood. It likely involves nitric oxide release. Isosorbide mononitrate is the only nitrate that has been tested in randomized trials. It has been found to reduce the hepatic venous pressure gradient102 and to enhance the splanchnic hemodynamic effect of propranolol.103 However, its systemic effects can lead to deleterious arterial hypotension. Nitrates are used in association with vasopressin or its analogue terlipressin.
Preprimary prophylaxis
Three clinical trials have studied this issue, but the results are not concordant.104–106 According to a statement from the Baveno international consensus conference, the use of β-blocker therapy is not recommended for preprimary prophylaxis.65
Primary prophylaxis
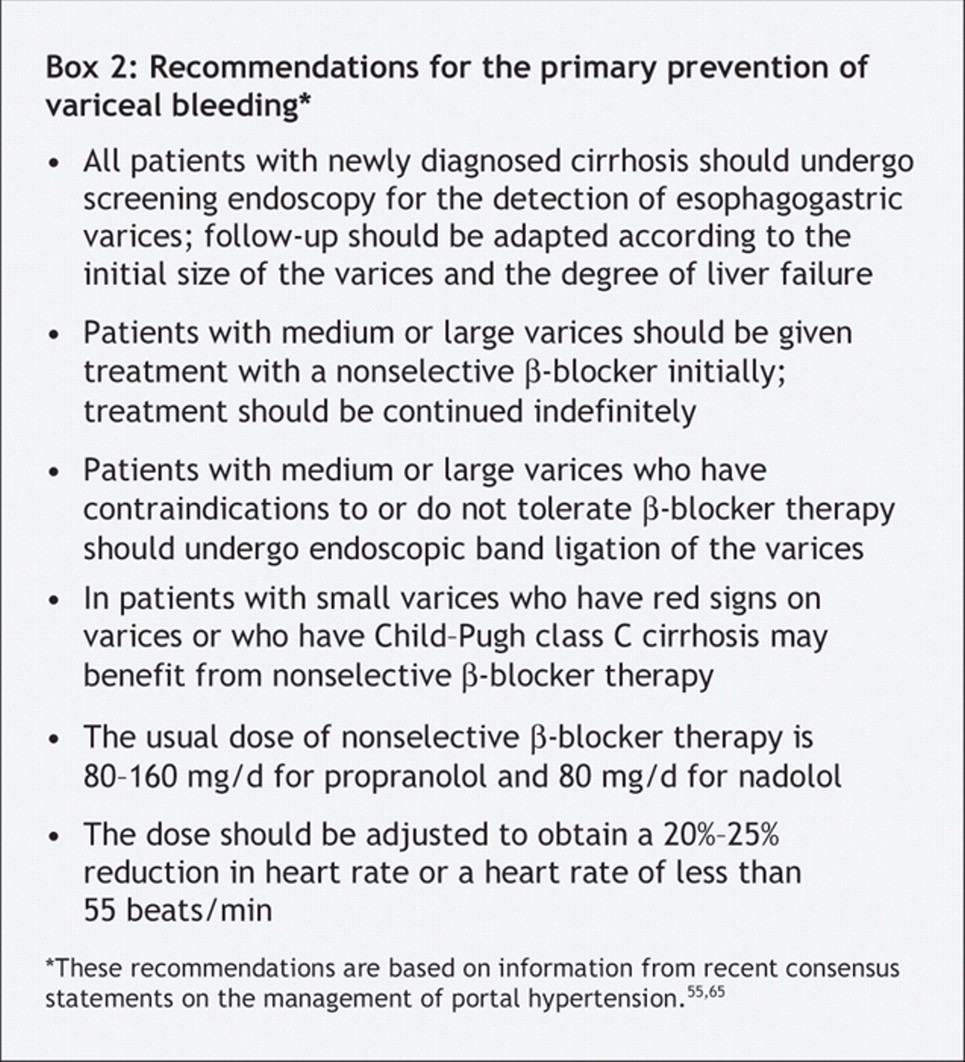
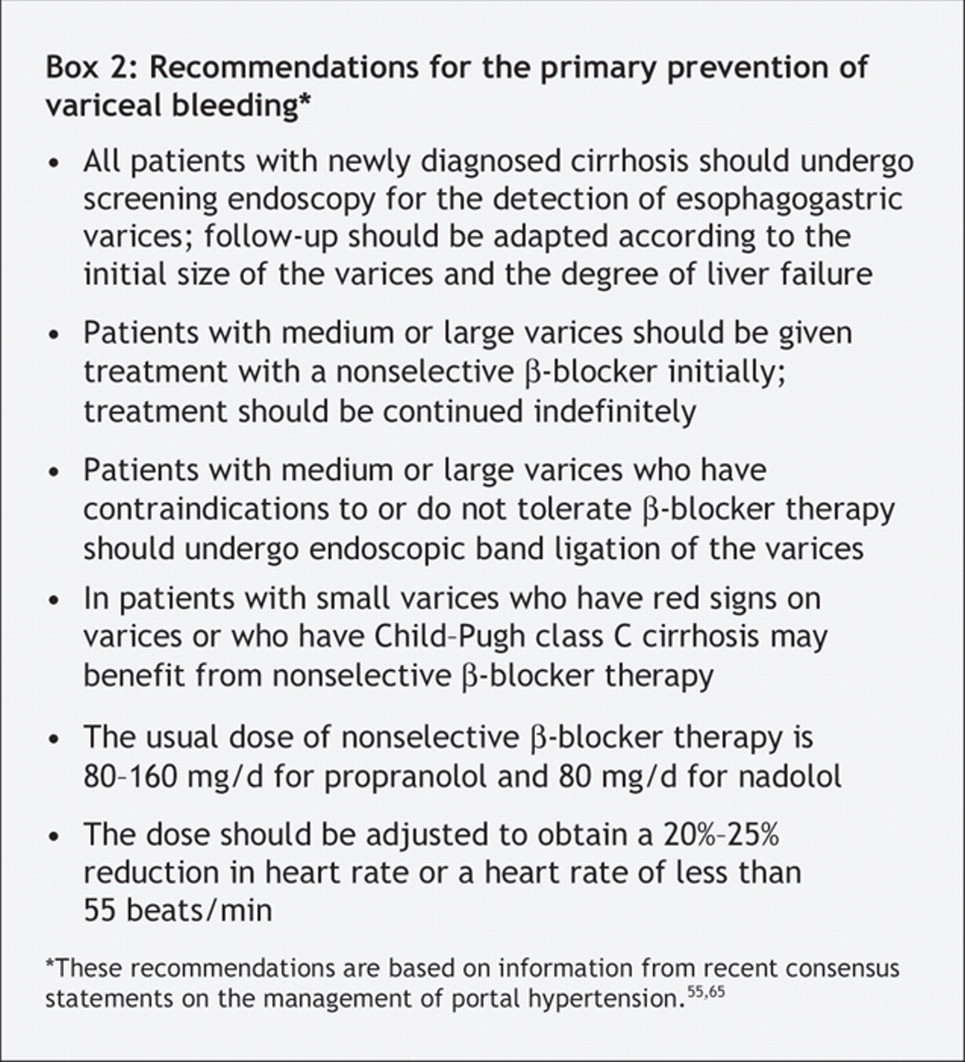
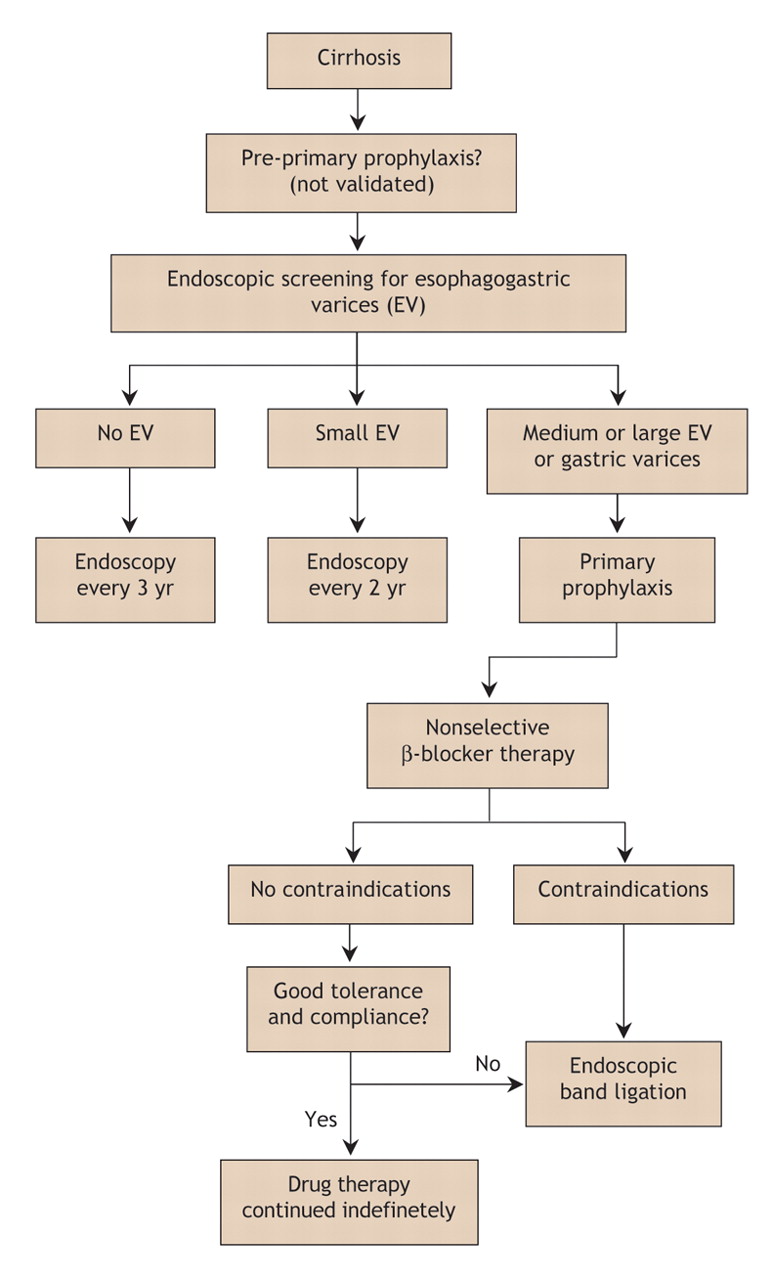
Endoscopic screening for the presence of esophagogastric varices should be done in all patients after the diagnosis of cirrhosis (Box 2).55,65 Screening should be repeated every 3 years in patients without varices and every 2 years in those with small varices (Fig. 4).55 Endoscopic follow-up should then relate to the initial size of detected varices. In case of large varices, endoscopic follow-up is not necessary, and primary prophylaxis with a nonselective β-blocker (propranolol or nadolol) should be started.55 Endoscopic band ligation is useful in preventing variceal bleeding in patients with medium or large varices; however, its long-term benefit requires further research,65 and it is not currently proposed for use in primary prophylaxis unless the patient has contraindications to or side effects from nonselective β-blocker therapy.
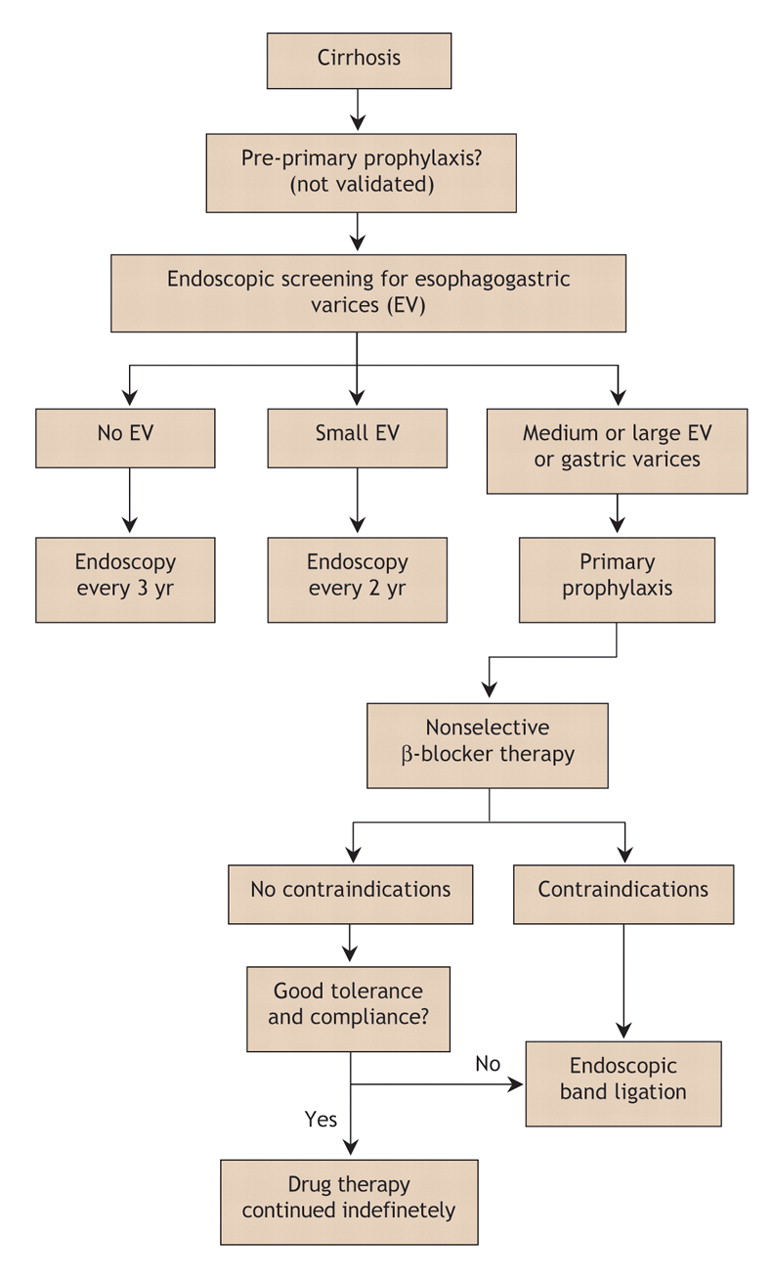
Fig. 4: Algorithm for the primary prophylaxis of variceal bleeding in cirrhosis.
Therapy with a nonselective β-blocker is effective in reducing the risk of a first variceal bleeding episode in patients with medium or large varices.65,107–111 Conventional treatment consists of administering the drug orally twice daily and titrating the dose according to the patient's tolerance and to the treatment objectives based on heart rate response.112,113 However, results of a pharmacodynamic study suggested that a single daily dose of long-acting propanolol is sufficient114 (80 or 160 mg, depending on the available dose in each country115). In all cases, doses should be adjusted to obtain a 20%–25% reduction in heart rate or a heart rate of less than 55 beats/min.55 Propranolol is effective for a few days in cirrhotic patients after the last dose is administered.114 β-Blocker therapy should be maintained indefinitely,55 since late withdrawal can be deleterious on survival despite the lack of an increased risk of bleeding.116 In patients who do not tolerate or have contraindications to β-blocker therapy, endoscopic band ligation is recommended55,65 (Fig. 4). Nitrates (isosorbide mononitrate) are ineffective in preventing variceal bleeding if used alone,117,118 and their use in primary prophylaxis is not recommended.55,65
Secondary prophylaxis
All patients who survive a variceal bleeding episode should receive treatment to prevent recurrent episodes. As a first-line treatment, both pharmacologic and endoscopic treatments can be used to prevent a recurrence. Pharmacologic therapy includes use of a nonselective β-blocker.111,119–122 Although it has been proposed,123 combined treatment with isosorbide mononitrate and propranolol is not recommended.55,65
Eradication of varices by endoscopic procedures is also effective in preventing recurrent variceal bleeding. Only endoscopic sclerotherapy has been compared with placebo, and it was associated with a significant reduction in recurrent bleeding and mortality.56,124 Endoscopic band ligation is currently preferable to endoscopic sclerotherapy,55 since it has been found to be more effective in reducing the risk of recurrent variceal bleeding and the incidence of variceal stricture.125–127 Combined therapy with the 2 endoscopic procedures does not appear to be more effective than endoscopic band ligation alone.128 However, endoscopic sclerotherapy may be effective in preventing the recurrence of varices when endoscopic band ligation is no longer feasible. One trial of endoscopic band ligation with and without therapy with nadolol and sucralfate for secondary prophylaxis showed reduced rates of recurrent variceal bleeding in the group given the combined therapy.129 Such a beneficial effect was not confirmed for combined therapy with endoscopic sclerotherapy and nonselective β-blockers.130,131
If secondary prophylaxis with a nonselective β-blocker or endoscopic band ligation, or both, fails to prevent variceal bleeding, rescue therapies should be considered. Both TIPS and surgical shunt creation are effective in preventing recurrent variceal bleeding.125 TIPS is more effective than endoscopic treatment,132 and surgical shunt creation is more effective than endoscopic sclerotherapy;133 however, neither TIPS nor surgical shunt creation has been found to improve survival, and both are associated with a high risk of encephalopathy.132,133
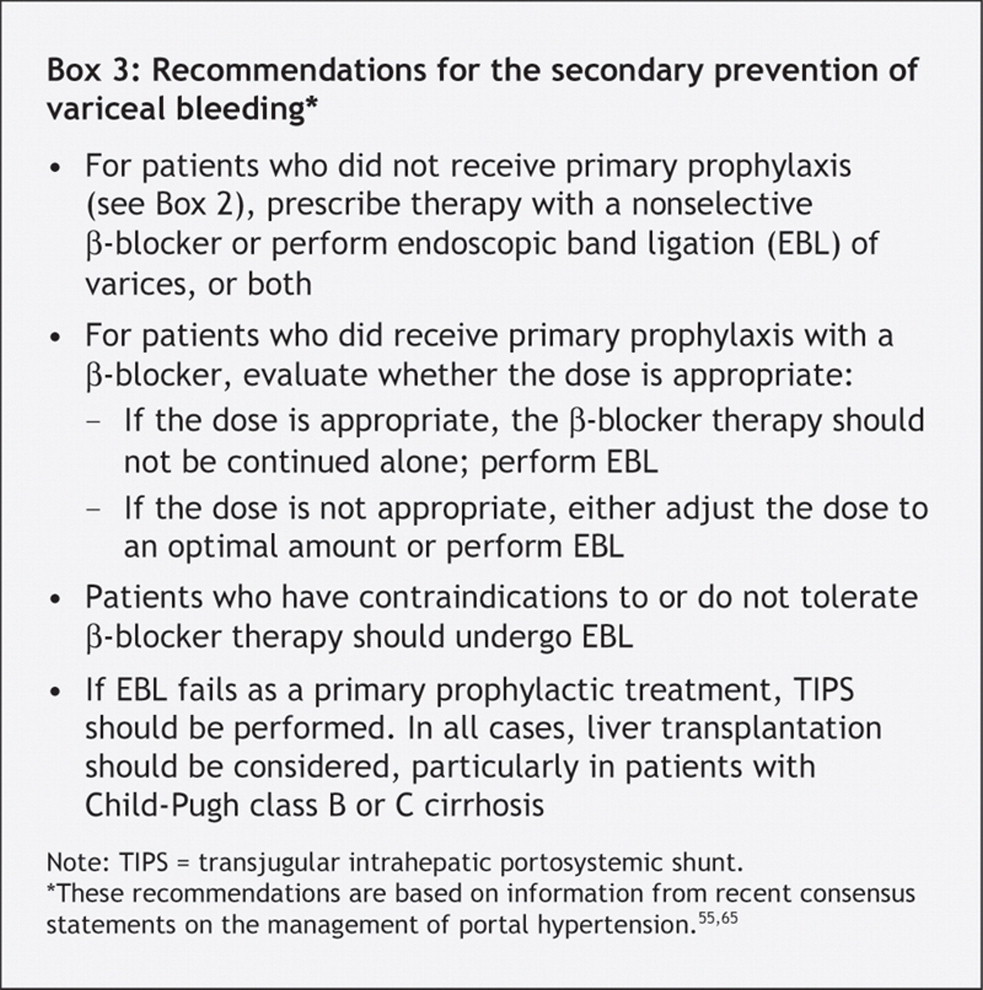
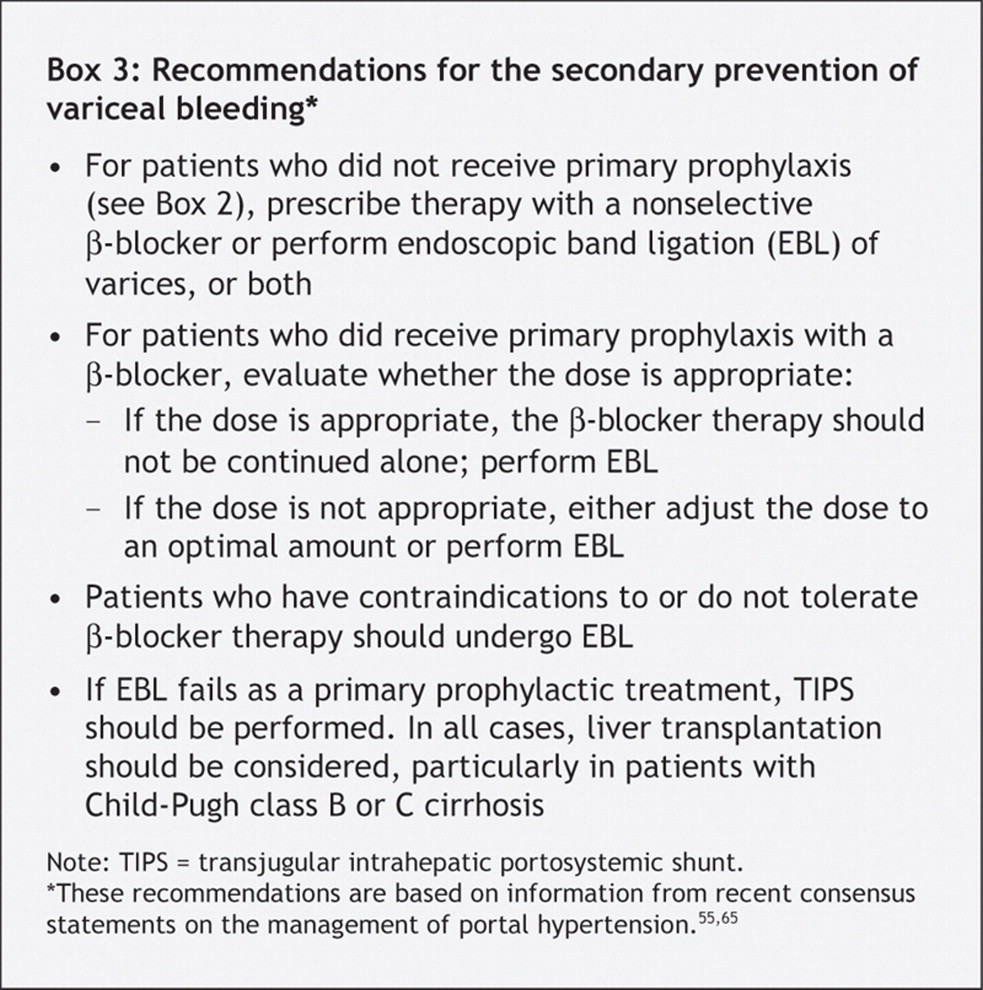
The 2 consensus statements on portal hypertension55,65 have established recommendations on prophylaxis status before variceal bleeding (Box 3). In patients who have not received previous primary prophylaxis, therapy with a nonselective β-blocker or endoscopic band ligation, or both, can be used. If primary prophylaxis with a β-blocker at an appropriate dose fails, the β-blocker therapy should not be continued alone and endoscopic band ligation should be performed. If the β-blocker dose is not found to be appropriate, either changing it to an optimal dose or performing endoscopic band ligation is possible. If endoscopic band ligation fails as primary prophylaxis, TIPS is the next option. Liver transplantation should be considered in all cases, particularly in patients with severe cirrhosis (Child–Pugh class B or C).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Ascites and its complications
Ascites occurs in cases of advanced cirrhosis and severe portal hypertension. The ultimate complications of ascites are refractory ascites, hepatorenal syndrome and spontaneous bacterial peritonitis.
Uncomplicated ascites
All patients with ascites should undergo an evaluation of ascitic fluid content to rule out spontaneous bacterial peritonitis.134,135 The evaluation should include cell count, bacterial culture in blood culture medium, measurement of protein concentration and cytologic examination in cases of suspected malignant ascites.134,135 The use of leukocyte reagent strips has been recently proposed for the early detection of leukocytes in ascites and spontaneous bacterial peritonitis.136–139
For subclinical ascites detectable only by ultrasonography, no specific treatment is necessary.135 However, a reduction in daily sodium intake (to 90 mmol/d) is recommended.
In cases of moderate ascites, renal function is usually preserved and treatment can be administered on an outpatient basis.134 Moderate dietary sodium restriction (90 mmol of sodium per day) should be imposed.135 Spironolactone, an anti-mineralocorticoid, is the drug of choice at the onset of treatment because it promotes better natriuresis more often than loop diuretics.140 It blocks the aldosterone-dependent exchange of sodium in the distal and collecting renal tubules, thus increasing the excretion of sodium and water.141 The initial dose is about 100–200 mg/d.134,135 About 75% of patients respond to treatment after only a few days.135 Side effects of spironolactone are gynecomastia, metabolic acidosis, hyperkalemia and renal impairment.135 In the presence of edema, treatment with furosemide (20–40 mg/d) may be added for a few days to increase natriuresis.134,135 Loop diuretics act by increasing sodium excretion in the proximal tubules. In cirrhosis, the effect of loop diuretic monotherapy is limited and therefore is more commonly used as an adjunct to spironolactone therapy.135 The side effects of furosemide include hypokaliemia, metabolic hypochloremic alkalosis, hyponatremia, hypovolemia and related renal dysfunction.135 Amiloride (5–10 mg/d) may be used when spironolactone is contraindicated or if side effects such as gynecomastia occur.134,135 It also acts in the distal tubule.135 Diuretic therapy should be monitored by measuring the patient's weight and levels of serum electrolytes, urea and creatinine daily.135 Maximum weight loss should not exceed 500 g/d in patients without peripheral edema and 1000 g/d in those with it.135 If the therapeutic effect is insufficient, urinary sodium excretion should be determined to identify nonresponsive patients (characterized by a urinary sodium excretion below 30 mmol/d).135
Patients with severe ascites will have marked abdominal discomfort. In such cases, higher diuretic doses are needed (i.e., up to 400 mg of spironolactone and 160 mg of furosemide daily).134,135 However, in some patients, free-water excretion is impaired and severe hyponatremia may develop.134 Frequently, large-volume paracentesis should be done.135 Paracentesis should be routinely combined with plasma volume expansion. If the volume of ascites removed is less than 5 L, a synthetic plasma substitute may be used.135,142 If more than 5 L of ascitic fluid is removed, albumin should be given at a dose of 8 g per litre of fluid removed.135
Refractory ascites develops in about 10% of cases.143 In such cases, liver transplantation should be considered.55,135 In the meantime, therapeutic strategies can involve repeated large-volume paracentesis and plasma volume expansion with albumin or TIPS.55,134,135 TIPS improves renal function and sodium excretion60,144,145 and is more effective than paracentesis in removing ascites.61,63 TIPS has a mortality not significantly differerent from that associated with paracentesis.63 Nevertheless, a recent meta-analysis has reported a tendency toward improved survival with TIPS.61
Hepatorenal syndrome
Hepatorenal syndrome is the most serious circulatory renal dysfunction in cirrhosis21 and is the most severe complication of portal hypertension. It occurs in up to 10% of patients with ascites.146 The syndrome is defined by a serum creatinine concentration greater than 1.5 mg/dL (> 133 μmol/L).134 Type 1 hepatorenal syndrome involves the rapid impairment of renal function, characterized by a doubling of the initial serum creatinine concentration to more than 2.5 mg/dL (> 221 μmol/L) within 2 weeks.146 In type 2 hepatorenal syndrome, renal impairment is stable or progresses at a slower rate than that in type 1.146
The ideal treatment of hepatorenal syndrome is liver transplantation.55 Besides transplantation, vasoactive drug therapy in combination with albumin (20–40 g/d for 5–15 days) can be used.55,134 The efficiency of terlipressin (0.5–1 mg intravenously every 4–12 hours) has been reported in several uncontrolled trials.31–33 Therapy with norepinephrine (0.5–3.0 mg/h intravenously)147 or midodrine (7.5–12.5 mg orally 3 times daily) in association with octreotide (100–200 μg subcutaneously 3 times daily)148 has been suggested to improve hepatorenal syndrome, but its effectiveness remains to be confirmed. TIPS has been found to be effective in the management of hepatorenal syndrome by improving renal function, particularly in patients with a Child–Pugh score of 12 or less and a serum bilirubin level below 85 μmol/L.149
Spontaneous bacterial peritonitis
Spontaneous bacterial peritonitis, an infection of the ascitic fluid, occurs in 10%–30% of patients with ascites.73 All cases in which the neutrophil count is at least 250 × 106/L in ascitic fluid should be treated empirically, since ascites culture yields negative results in about 40% of patients with symptoms suggestive of spontaneous bacterial peritonitis.55,73 Empirical treatment should also be started if leukocytes are detected in ascitic fluid at a significant level on reagent strips.136–139
Because most cases of peritonitis are due to gram-negative bacteria (e.g., Escherichia coli),134 therapy with a third-generation cephalosporin is the treatment of choice (cefotaxime 2–4 g/d, intravenously, for 5 days).55,73 Alternative treatments include combination therapy with amoxicillin and clavulinic acid (1 g and 0.125 g respectively, given intravenously or orally 3 times daily) or norfloxacin (400 mg/d, orally) for 7 days.55,73 Antibiotic therapy should be used in conjunction with albumin infusion (1.5 g/kg on day 1 and 1 g/kg on day 3)55 to prevent renal failure and death.150 Treatment efficacy should be assessed by means of evaluating clinical symptoms and determining the neutrophil count in ascitic fluid after 48 hours.55,73 If treatment fails, antibiotic therapy should be shifted toward a broader-spectrum drug or to one adapted to the organism's antibiogram.55,73
Primary prophylaxis of spontaneous bacterial peritonitis with continuous oral norfloxacin therapy (400 mg/d) in hospital patients with cirrhosis who have a low ascitic protein concentration (< 10 g/L) is still debated.55,73 The same treatment is recommended for secondary prophylaxis of spontaneous bacterial peritonitis until the ascites resolves, a treatment option that is more easily accepted by clinicians.55,73
Summary
Portal hypertension can lead to severe outcomes in patients with cirrhosis, including bleeding of esophagogastric varices and complications of ascites.
Variceal bleeding is a clinical emergency and requires blood volume replacement, early vasoactive drug therapy, prophylactic antibiotic treatment and endoscopic treatment. Prophylaxis of variceal bleeding involves the use of β-blocker therapy (first-line treatment in primary and secondary prophylaxis) and endoscopic treatment, especially band ligation (second-line step in primary and first-line step in secondary prophylaxis).
Treatment of ascites includes diuretic therapy and dietary sodium reduction. Main complications of ascites are refractory ascites, hepatorenal syndrome and spontaneous bacterial peritonitis. In refractory ascites, repeated large-volume paracentesis (with volume expansion using albumin) and TIPS can be proposed. In hepatorenal syndrome, the most serious complication of ascites, liver transplantation should be considered; vasoactive drug therapy in combination with albumin infusion can be given in the meantime. All patients with ascites should be screened for spontaneous bacterial peritonitis; if detected, treatment consists of antibiotics and albumin infusion to prevent hepatorenal syndrome.
Footnotes
-
This article has been peer reviewed.
Contributors: All of the authors made substantial contributions to the conception and design of the study, the acquisition, analysis and interpretation of the data, the drafting of the article and the critical revision of it for important intellectual content. All gave final approval of the version to be published.
Acknowledgment: We thank Myriam Brian for her help with English-language revisions.
Competing interests: None declared for Nina Dib, Frédéric Oberti. Paul Calès has received honoraria for clinical research from Debiovision, Montréal.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.
- 32.
- 33.
- 34.
- 35.
- 36.
- 37.
- 38.
- 39.
- 40.
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.
- 115.
- 116.
- 117.
- 118.
- 119.
- 120.
- 121.
- 122.
- 123.
- 124.
- 125.
- 126.
- 127.
- 128.
- 129.
- 130.
- 131.
- 132.
- 133.
- 134.
- 135.
- 136.
- 137.
- 138.
- 139.
- 140.
- 141.
- 142.
- 143.
- 144.
- 145.
- 146.
- 147.
- 148.
- 149.
- 150.
- 151.
- 152.