

A 72-year-old man presented to the emergency department with a 3-week history of fever, dysuria and rectal pain, along with urinary frequency and urgency. The patient had a 10-year history of type 2 diabetes and benign prostatic hypertrophy, which had been treated with metformin and finasteride, respectively. His examination was remarkable for a palpable, tender fluctuant mass on digital rectal examination of the prostate. He had a white blood cell count of 13.5 (normal range 4–10) × 109/L and a serum creatinine level of 141 (baseline 114) μmol/L. Urine microscopy showed moderate bacteria; large positive leukocyte esterase and positive nitrite results were seen on urine dipstick testing. He was admitted to hospital with a diagnosis of prostatis and started on ceftriaxone administered intravenously (1 g/d).
Because the patient remained febrile for more than 48 hours after treatment was started, we obtained contrast-enhanced computed tomography (CT) of the abdomen and pelvis, which showed heterogeneous attenuation of the prostate gland suggestive of prostatic abscesses (Figure 1; Appendix 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.200470/tab-related-content). A urine culture identified Klebsiella pneumoniae. Results for blood culture were negative. A few days after admission, he had difficulty urinating, which required insertion of an indwelling urethral catheter. He underwent a transurethral resection of the prostate and abscess drainage. Histopathology of a biopsy specimen showed inflammation with necrosis and abscess formation. Urinary retention developed after the resection; we prescribed ciprofloxacin administered orally and discharged our patient to home with an indwelling catheter that was removed after 2 days. At a follow-up visit 6 weeks later, he reported no symptoms.

{kind=link}
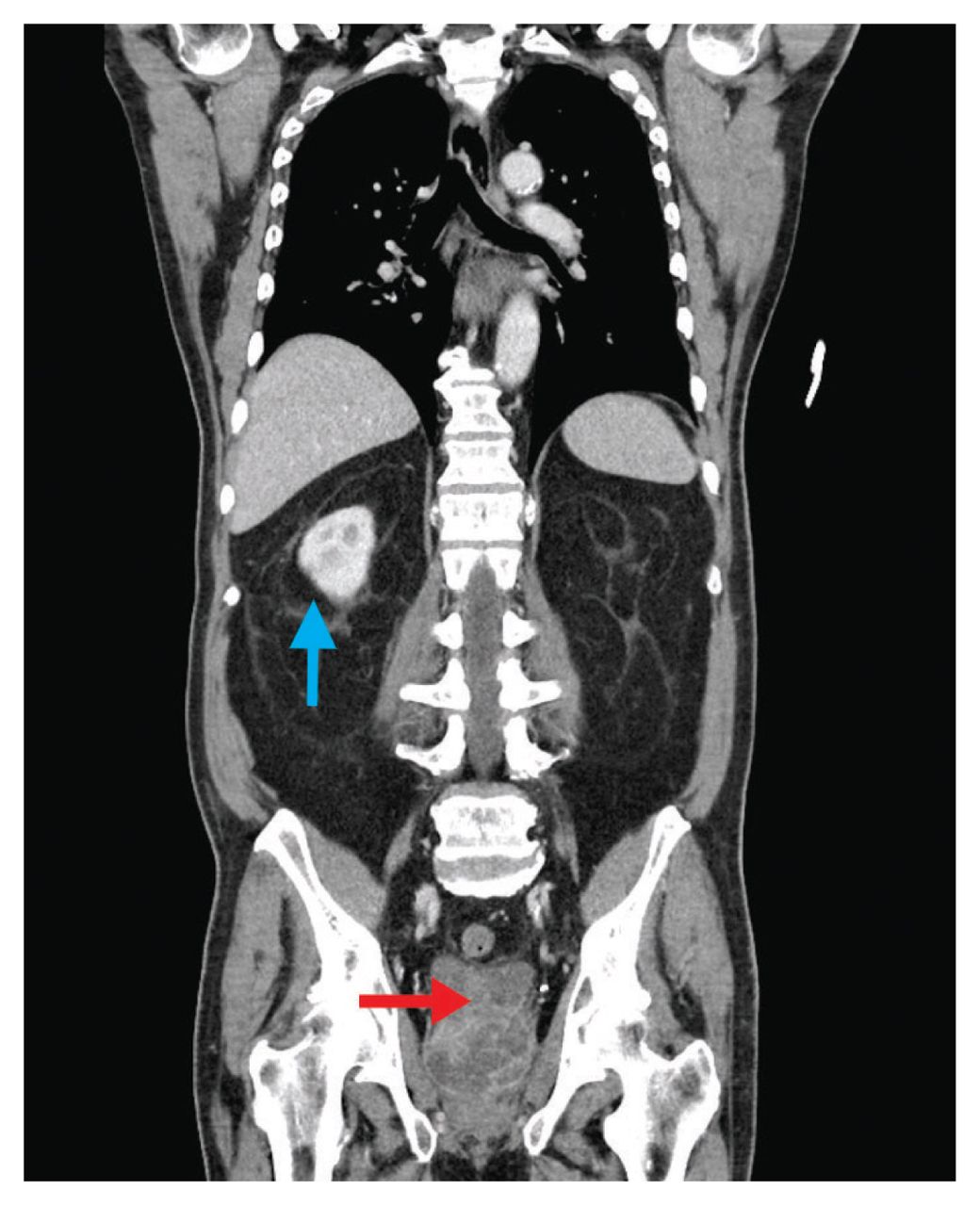
Coronal computed tomography scan of the abdomen and pelvis in a 72-year-old man with rectal pain and fever, showing prominent right perinephric stranding (blue arrow). Enlargement (7 cm in diameter) and heterogeneous attenuation of the prostate gland with nonenhancing fluid-density collections are suggestive of prostatic abscesses (red arrow).
Prostatic abscesses occur in 2.7% of patients with acute bacterial prostatitis,1 which occurs most commonly in older patients with diabetes mellitus. Other predisposing factors include long-term catheterization, prostatic manipulation, urethral obstruction and an immunocompromised state.1 Gram-negative bacilli and Enterococcus are most frequently involved.1 The presentation of a prostatic abscess is similar to that of bacterial prostatitis;1 however, fluctuance of the prostate on digital rectal examination can suggest the presence of an underlying abscess. Findings on CT include enlargement and heterogeneous attenuation of the prostate with nonenhancing fluid-density collections. Management options include antibiotics (abscesses < 1 cm),2 transrectal ultrasonography-guided aspiration, transurethral resection of the prostate and open drainage.3,4 Transrectal ultrasonography-guided aspiration is preferred because of its low risk of complications and may be repeated. However, failure is common for aspiration of abscesses greater than 3 cm or with an anechoic or heterogeneous appearance; for these lesions, transurethral resection of the prostate is preferred.4 Older age, high-grade fever, urinary retention, positive results for blood cultures and benign prostatic hyperplasia are associated with poor outcomes.1
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/