

Background: This spring marks the fifth year since the first outbreak of West Nile virus (WNV) in North America in 1999. As in previous years, the strategy at the national, provincial and local levels is focused on surveillance, education and mosquito control.
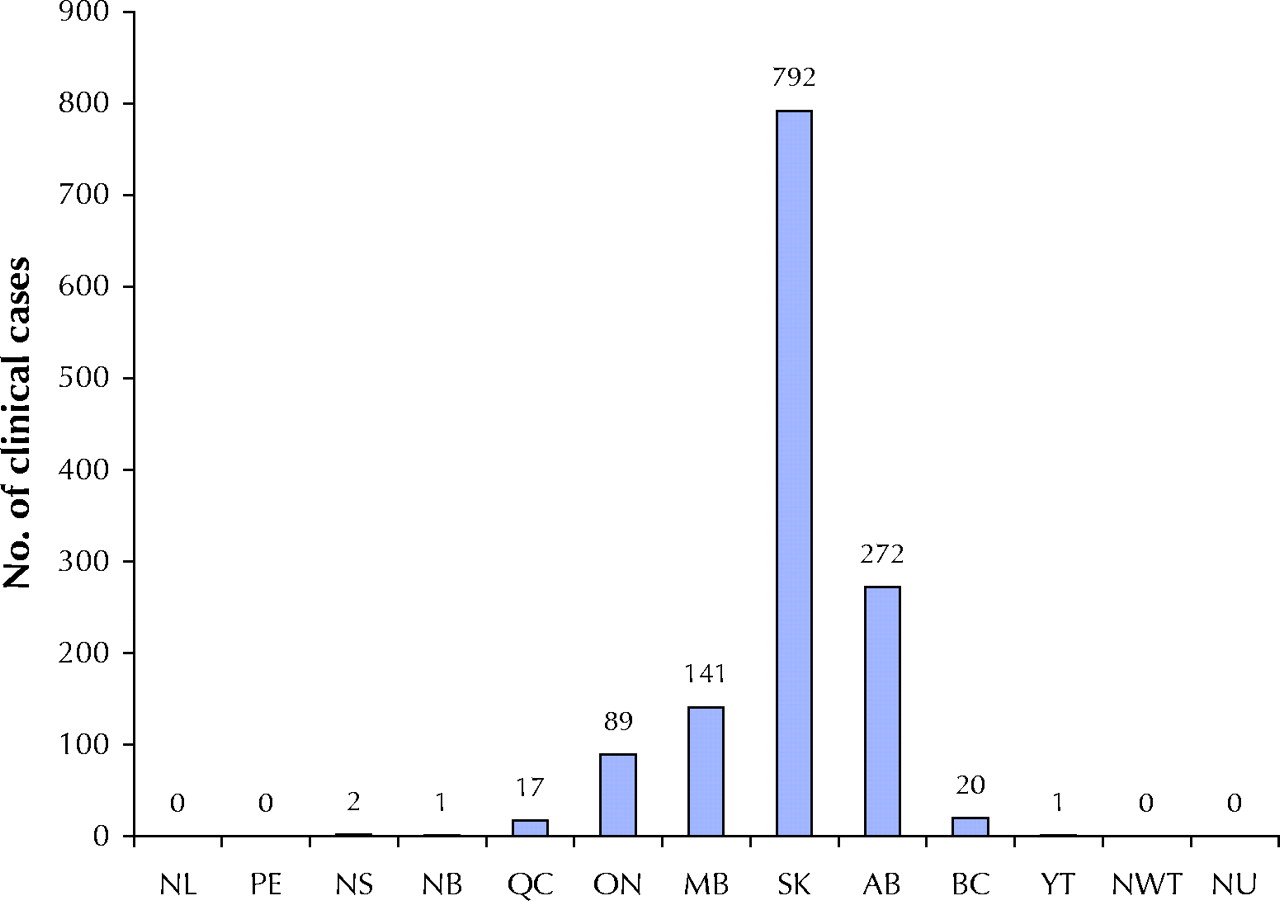
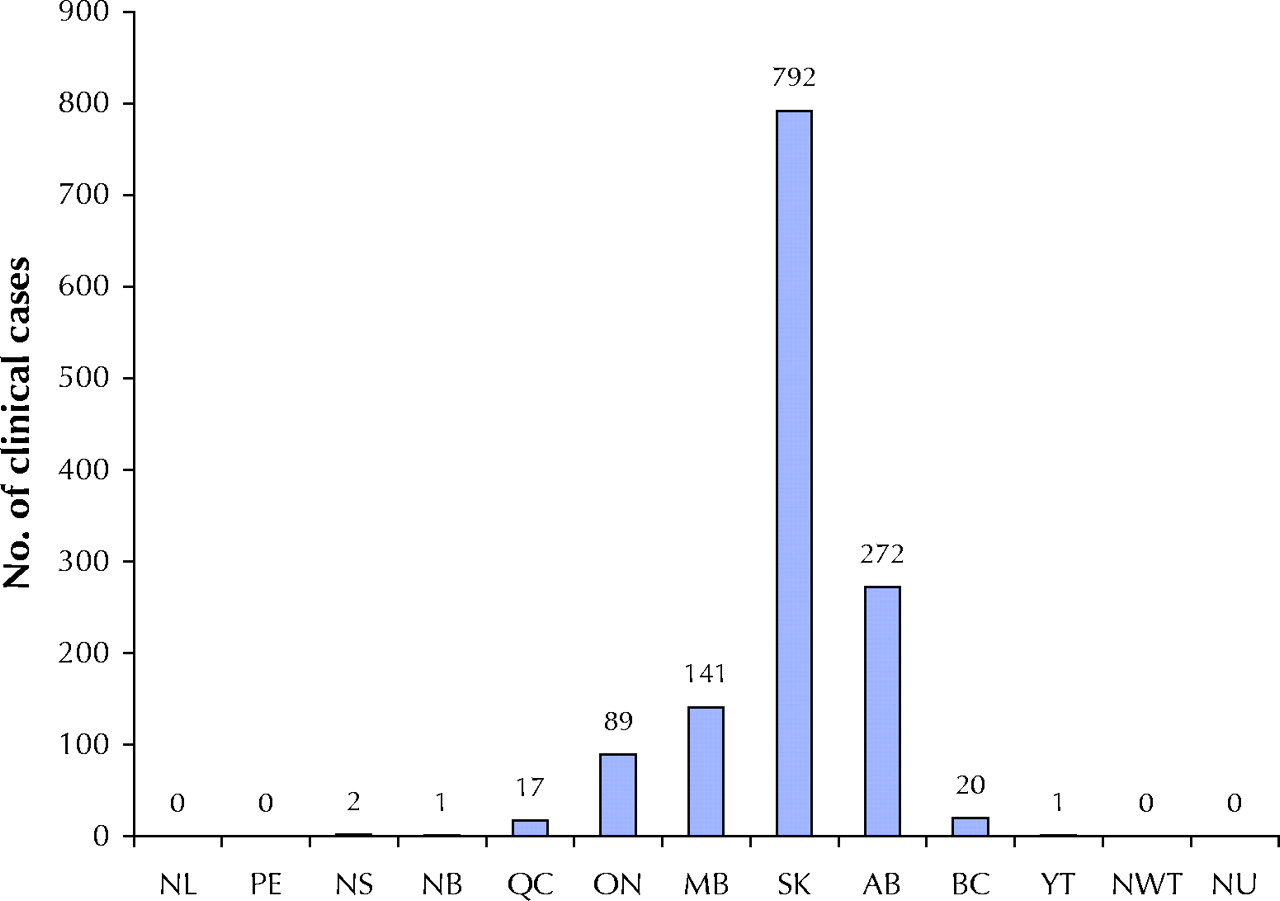
WNV infection first appeared in Canada, in Ontario, in 2001. Since then it has rapidly spread to other provinces, with the Prairies reporting the highest numbers of human cases in 2003 (Fig. 1). So far, the epidemiology of the disease is consistent with our understanding of epizootic diseases. Regional hot spots of WNV activity erupt when ecological conditions favour amplification of the virus between birds and mosquitoes. Culicine mosquitoes are the most important carrier for WNV given their preference for feeding on birds and ability to transmit the virus. As the season progresses, the level of virus in birds and mosquitoes increases until it reaches a point of spillover into mosquitoes that bite people as well as birds. Although 130 native North American bird species and a number of mammals (e.g., squirrels) have been identified as having WNV infection, corvids (e.g., crows, ravens, blue jays) are the best indicator species because of their high mortality rates. Surveillance activities include monitoring dead bird density and testing mosquitoes for the virus. A sharp rise in bird deaths has often presaged an outbreak of WNV infection; however, this may not be a reliable indicator after the first year owing to the decimation of the local crow population.
{kind=link}
Fig. 1: Total number of clinical cases of West Nile virus infection across Canada in 2003.
At least 4 seroprevalence studies have been conducted in the past 4 years in WNV hot spots. The results are consistent. About 1%–4% of people in areas with high WNV activity have antibody (IgM) evidence of recent WNV infection.1 The majority of infected people (80%) experience no discernible symptoms. About 20% experience the less severe form of infection (WNV fever), and 1 in 80–150 experience severe disease with neurological manifestations. Age appears to be the most significant risk factor for severe disease. The incidence of neuroinvasive disease begins to increase at about age 40 and increases with successive age groups. Rates of WNV fever are relatively constant across age groups.
Clinical management: The incubation period ranges from 3–14 days. WNV infection should be considered in the evaluation of any adult with fever and rash presenting from July to the end of September, or at other times if the patient has travelled to an area where WNV is circulating. The most common symptoms of WNV fever are fever, myalgia, fatigue, headache and joint pain. Neuroinvasive WNV also often begins with a prodromal fever, but it progresses to a decreased level of consciousness. Lower motor neuron dysfunction is a hallmark of severe WNV disease.2
An enzyme-linked immunosorbent assay test conducted on blood serum collected in the acute phase of illness (within 8 days after symptom onset) has a sensitivity of 95% and specificity of 90%.2 Confirmatory testing by means of the plaque reduction neutralization test takes longer and is usually more informative if performed on convalescent serum (collected 10–14 days after symptom onset) because of late induction of neutralizing antibodies. Nucleic acid amplification tests of cerebrospinal fluid may also be indicated if the patient is immunocompromised, since such patients often fail to mount an antibody response sufficient for detection.
Treatment is supportive. WNV fever appears to be self-remitting. People with neurological manifestations experience a more protracted course, often involving intensive care in hospital and home care upon discharge.2
Prevention: Prevention is aimed at modifying personal behaviour to reduce the risk of mosquito exposure, modifying mosquito habitat to reduce the number of breeding sites and, in some jurisdictions, applying larvicides and adulticides to control the mosquito population. Personal protective measures include wearing light-coloured long-sleeved clothing, using a DEET-based insect repellent (no greater than 30% for adults and 10% DEET for children) and ensuring that window screens are intact and snug. According to a seroprevalence study that compared behaviours between infected and noninfected people, practising 2 or more personal protective behaviours reduced the risk of infection by half (adjusted odds ratio [OR] 0.47, 95% confidence interval [CI] 0.23–0.86, p = 0.014). Spending time outdoors at dusk or dawn increased the risk of infection (adjusted OR 1.47 per hour, 95% CI 1.22– 1.77, p = 0.006).1
Mosquitoes breed near stagnant water, so emptying outdoor containers such as old tires, wheelbarrows and pool covers can reduce local exposure. The use of larvicides, placed in stagnant water where mosquito larvae are found, is a lengthy process and the decision to apply them is based on general assessment of risk for the upcoming season. The use of adulticides (sprayed from truck- or plane-mounted equipment) is used to mitigate a more immediate risk of illness in the subsequent days or weeks. Use of pesticides, especially adulticides, is not without controversy. A number of factors influence the use of pesticides in different jurisdictions. These include the level of local WNV activity and public acceptance of and familiarity with pesticide application.
Erica Weir Associate Medical Officer of Health Kingston, Frontenac and Lennox & Addington Health Unit Kingston, Ont. Howard Shapiro Associate Medical Officer of Health Peel Health Brampton, Ont.
References
- 1.
- 2.