

A58-year-old woman presented to the emergency department. She had been vomiting and feeling confused for three days, and she had fallen several times.
Three months before her presentation, the patient had been admitted to the intensive care unit at another hospital for profound dehydration, acute kidney injury (creatinine 690 [normal 61.9–115] μmol/L) and a serum sodium level that the laboratory had reported as “undetectable.” Under the direction of a nephrologist, the patient’s metabolic abnormalities were corrected to near-normal values with intravenous administration of fluids.
The patient’s medical history included rectal prolapse of two years’ duration and a worsening, clear rectal discharge of four years’ duration. The discharge had become so profuse that she required wearing adult briefs 24 hours each day. She had previously undergone evaluation by a general surgeon and urogynecologist. A flexible sigmoidoscopy performed one year before her current presentation was of limited quality owing to stool and liquid in the rectum but was reported as “grossly normal to 10 cm.”
On physical examination, the patient was alert and oriented, but her verbal responses were delayed. She had a laceration and ecchymosis over the forehead. Her vital signs were as follows: blood pressure 97/54 mm Hg, heart rate 70 beats/min, respiratory rate 18 breaths/min, oxygen saturation 97% on room air, body temperature 36.3°C), and her jugular venous pulse was not visible above the clavicle. Cardiovascular, respiratory and neurologic examinations were normal. An examination of the patient’s perianal region showed copious leakage of a clear, colourless fluid, but no other abnormalities were identified. On digital examination, however, a soft, fleshy mass 4–5 cm in diameter was palpated.
Laboratory investigations identified hyponatremia (104 [normal 136–145] mmol/L), hypokalemia (1.8 [normal 3.5–5.0] mmol/L), hypochloremia (< 45 [normal 98–106] mmol/L) and acute kidney injury (creatinine 392 [61.9–115] μmol/L). Her bicarbonate level was normal (24 [24–32] mmol/L), and her serum osmolality was low (261 [275–295] mmol/kg). A urine analysis showed a sodium level of less than 10 mmol/L, chloride less than 10 mmol/L and an osmolality of 367 mOsm/kg. Analysis of the patient’s rectal effluent showed a sodium level of 118 mmol/L, a potassium level of 24 mmol/L and chloride level of 118 mmol/L.
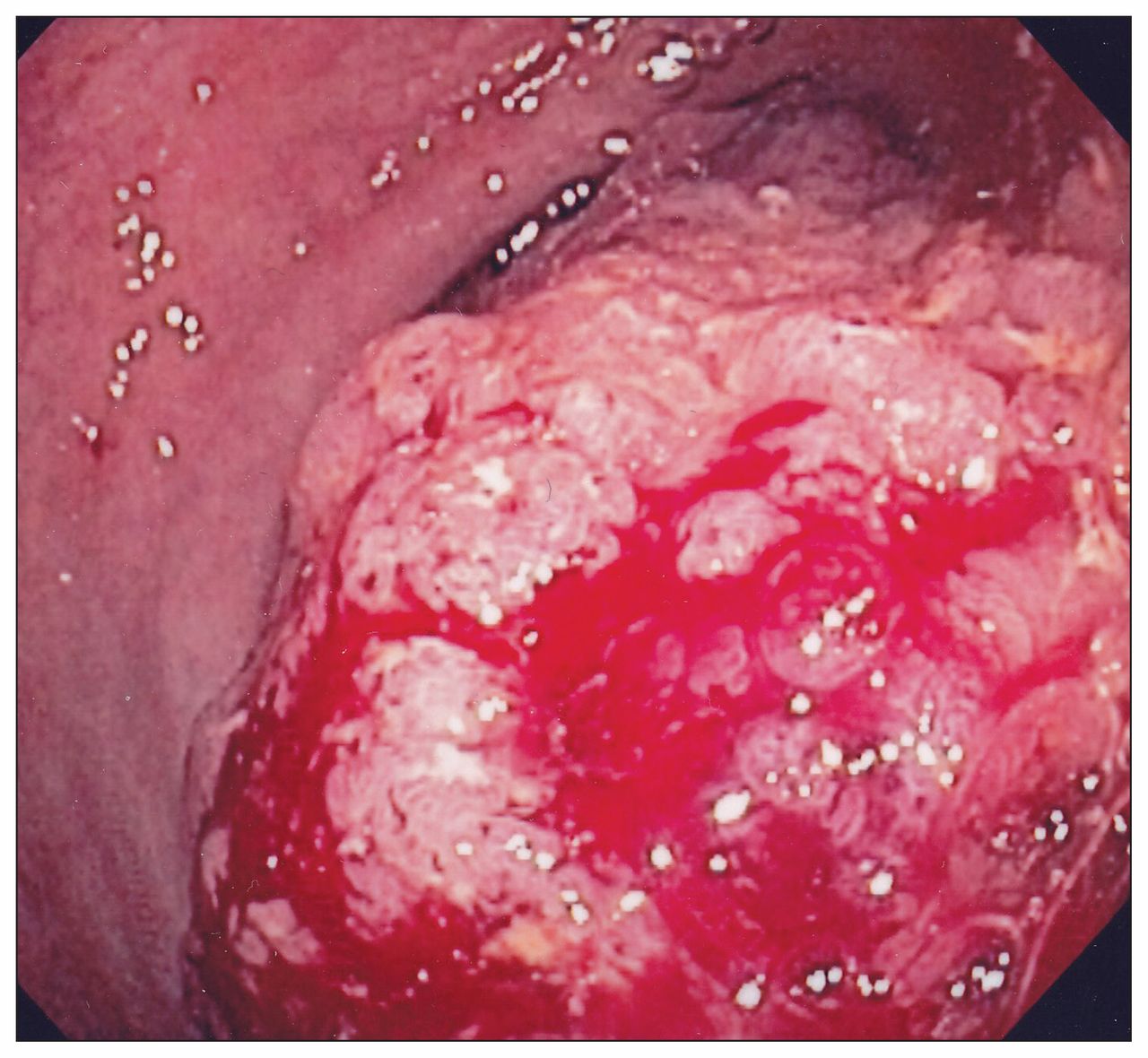
The patient’s serum sodium was slowly corrected over the next 60 hours (Appendix 1, available at www.cmaj.ca/lookup/suppl/doi:10.1503/cmaj.141195/-/DC1). We performed a flexible sigmoidoscopy, which identified a massive rectal lesion at 5 cm that could not be bypassed with the colonoscope (Figure 1). Multiple biopsy samples were taken, and pathology identified a tubulovillous adenoma with no evidence of high-grade dysplasia. A computed tomography scan of the abdomen and pelvis showed a large frond-like rectosigmoid tumour, with transient intussusception into the lower rectum and no clear radiographic evidence of extramural invasion (Figure 2). The patient was taken to the operating room where an open, low-anterior resection with coloanal anastomosis and a defunctioning loop ileostomy was performed. Surgical pathology identified a 10.7-cm obstructing tumour located below the peritoneal reflection. Most of the tumour comprised tubulovillous adenoma, but multiple foci of high-grade dysplasia and a single focus of invasion into the submucosa were seen. One of 27 lymph nodes resected with the specimen was positive for adenocarcinoma. Therefore, the final pathologic diagnosis was rectal adenocarcinoma.

Massive rectal lesion seen on flexible sigmoidoscopy in a 58-year-old woman with dehydration. The lesion was unable to be bypassed with the colonoscope. Note that the visible bleeding is the result of multiple biopsy samples taken at the time of sigmoidoscopy.

{kind=link}
{kind=link}
Computed tomography image of the patient’s abdomen and pelvis showing the large rectosigmoid mass with intussusception into the lower rectum.
The patient was discharged in stable condition five days after her surgery. She was seen for follow-up by the medical oncology service, which recommended that she receive adjuvant chemotherapy. The patient elected to defer this decision to a later date. Follow-up at three months showed a completely normal electrolyte profile and normal creatinine with full resolution of symptoms.
Discussion
Adenomas are dysplastic, premalignant growths of the colon and rectum found in 30% of all screening colonoscopies.1 They are classified according to their pathologic glandular architecture as tubular, villous or tubulovillous. Although small adenomas are typically asymptomatic, they may ulcerate as they grow, resulting in gastrointestinal bleeding, tenesmus or intestinal obstruction. Large villous adenomas may develop a unique symptomatology — McKittrick–Wheelock syndrome — when they produce large quantities of mucin that contains electrolytes.2
First described in 1954, McKittrick–Wheelock syndrome is characterized by a large volume of secretory diarrhea, dehydration, prerenal acute kidney injury and severe electrolyte abnormalities secondary to a hypersecretory villous adenoma.2 This hypersecretory function is reported to occur in 2%–3% of large villous adenomas, typically greater than 3–4 cm in diameter and located in the rectosigmoid colon where the surface area for normal reabsorption is limited.3–5 Rarely, as seen in our patient’s case, intussusception and rectal prolapse can occur owing to the large size and distal location of the adenoma.6
The hydroelectric derangements associated with hypersecretory villous adenomas can be striking. The masses may produce a rectal discharge in excess of 4.0 L/day with an average reported sodium content of 120 mmol/L, potassium content of 4.4 mmol/L and chloride content of 123 mmol/L.7,8 Renal adaptation and increased oral intake may initially compensate for the fluid and electrolyte losses. Patients may have mucinous diarrhea for several years before an acute presentation of confusion, altered consciousness and circulatory collapse.9 In one of the earliest case series, the average time from symptom onset to circulatory collapse was 5.5 years.10
In addition to a thorough history and physical examination, measurement of urinary electrolytes can provide important diagnostic information when a patient presents with hyponatremia and hypochloremia. In the setting of decreased total effective circulating volume, a low urinary chloride concentration (< 10 mmol/L) limits the differential diagnosis to vomiting, excessive nasogastric suctioning, diuretic use, cystic fibrosis and hypersecretory villous adenoma. All but the last of these conditions may be diagnosed by history alone.11 Classically, patients with these conditions will also present with a metabolic alkalosis.
McKittrick–Wheelock syndrome heralds the presence of an underlying large villous adenoma, which carries a substantial risk of invasive cancer. Adenoma size and the extent of villous architecture are the two major risk factors associated with high-grade dysplasia, the immediate precursor to invasive carcinoma.12 Villous pathology, compared with tubular pathology, carries a 10-fold increase in risk of invasive carcinoma for tumours less than 1 cm. Fifty percent of villous adenomas that are larger than 2 cm harbour invasive cancer.13
Conclusion
Our patient presented with a four-year history of mucinous diarrhea, a two-year history of rectal prolapse and two episodes of profound volume depletion with life-threatening electrolyte abnormalities. Investigations identified a large rectal villous adenoma secreting a high volume of electrolyte-rich fluid: a classic case of McKittrick–Wheelock syndrome. Although uncommon, this is an important differential diagnosis in patients presenting with electrolyte abnormalities and secretory diarrhea, because correct identification will lead to definitive endoscopic or surgical treatment that can be life-saving.
The section Cases presents brief case reports that convey clear, practical lessons. Preference is given to common presentations of important rare conditions, and important unusual presentations of common problems. Articles start with a case presentation (500 words maximum), and a discussion of the underlying condition follows (1000 words maximum). Visual elements (e.g., tables of the differential diagnosis, clinical features or diagnostic approach) are encouraged. Consent from patients for publication of their story is a necessity. See information for authors at www.cmaj.ca.
Severe hyponatremia and hypochloremia in the context of low urine chloride can signal the presence of a hypersecretory villous adenoma.
McKittrick–Wheelock syndrome occurs when large villous adenomas produce large volumes of electrolyte-containing mucin.
Distal villous adenomas are more likely to cause McKittrick–Wheelock syndrome owing to the limited mucosal surface area available for fluid reabsorption.
Removal of the hypersecretory villous adenoma is the definitive treatment for McKittrick–Wheelock syndrome and can be life-saving.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.
Contributors: Michael Raphael prepared the initial draft of the manuscript. All of the authors revised the manuscript and had full access to, and verify the accuracy of, the data presented. All of the authors approved the final version submitted for publication. Allan Detsky has agreed to act as guarantors of the work.