


Coronary computed tomography angiography (CTA) is a noninvasive imaging study that allows for the detection of coronary artery stenosis
Contrast medium is injected intravenously, and multidetector technology is used to take an image of the heart during a single breath hold (acquisition time ~8 s for 64 detectors). Blockade is recommended for patients with heart rates faster than 65 beats/min to improve image quality and to reduce exposure to radiation. Because of its coronary vasodilatory effect, nitroglycerin is given sublingually to optimize image quality.1
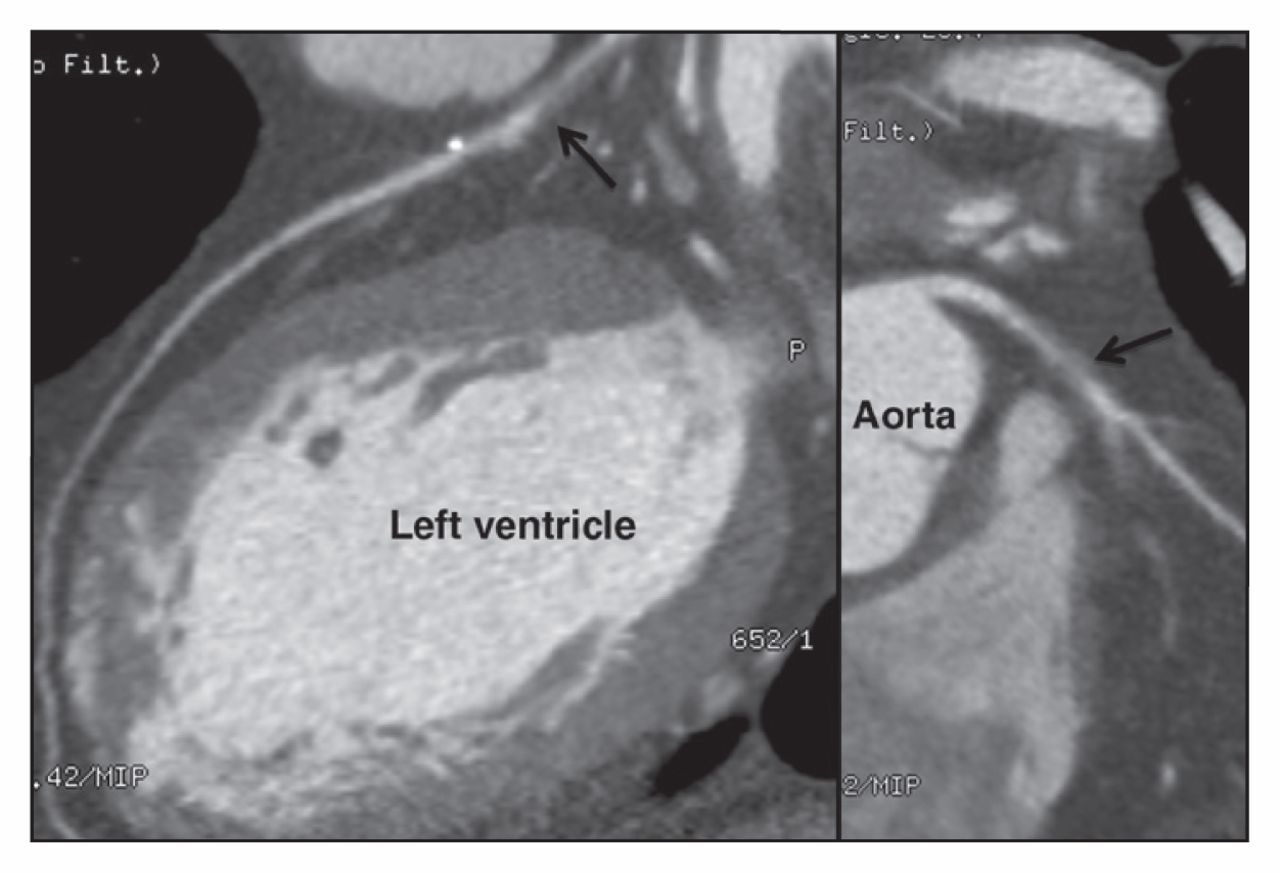
High-grade (70%–99%) stenosis at the proximal left anterior descending artery (arrow) on the basis of predominantly noncalcified plaque.
Coronary CTA has high diagnostic accuracy compared with invasive coronary angiography
Multicentre trials comparing stenosis as seen on coronary CTA with that seen on invasive coronary angiography — the gold standard — have found high sensitivity (85%–99%) and specificity (64%–90%). Coronary CTA is most useful at ruling out coronary artery disease, with a very high negative predictive value (83%–99%).2
Coronary CTA has additional advantages over invasive coronary angiography
Invasive angiography focuses only on the lumen, whereas CTA provides information on the extent and characterization of plaque. In addition, CTA allows evaluation of the course of coronary vessels, congenital abnormalities, cardiac anatomy and extracardiac pathology. Current CT machines and low-dose protocols result in a radiation dose similar to that of annual background radiation (2–4 mSv).3
Coronary CTA used in routine practice does not provide information on coronary blood flow
Routine CTA currently done in clinical practice assesses stenosis severity and plaque burden, but does not provide information as to the hemodynamic significance of the stenosis. Recent advances have resulted in extensive hemodynamic data by integrating computational fluid dynamics into a resting coronary CTA anatomic model, and are showing great promise.4
There are several indications for using coronary CTA in routine practice
Coronary CTA is useful in exercise testing when patients have intermediate risk findings or normal findings with continued symptoms; equivocal stress imaging results; or discordant results on exercise electrocardiography and stress imaging.5 Coronary CTA is not appropriate for patients with symptoms of definite acute myocardial infarction or a high pretest likelihood for coronary stenosis.5
Footnotes
Competing interests: Jonathan Leipsic has received grant funding from GE Healthcare and Heartflow; his institution has grants pending from Edwards Life Sciences, Neovasc and Tendyne. No other competing interests were declared.
In this issue

{kind=link}
Article tools






Jump to section
- Article
- Coronary computed tomography angiography (CTA) is a noninvasive imaging study that allows for the detection of coronary artery stenosis
- Coronary CTA has high diagnostic accuracy compared with invasive coronary angiography
- Coronary CTA has additional advantages over invasive coronary angiography
- Coronary CTA used in routine practice does not provide information on coronary blood flow
- There are several indications for using coronary CTA in routine practice
- Footnotes
- References
- Figures & Tables
- Responses
- Metrics
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

