


A 37-year-old right-handed man presents with a three-month history of worsening tingling, numbness and weakness of the left hand that is beginning to affect his occupation as a manual worker. Examination reveals wasting of the hypothenar eminence and reduced sensation in the little and ring fingers. The Tinel test is positive over the cubital tunnel (i.e., tapping a finger over the cubital tunnel produces altered sensation in the distribution of the ulnar nerve).
What diagnoses should be considered?
The likely diagnosis is cubital tunnel syndrome. Other diagnoses to consider include cervical radiculopathy or compression of the ulnar nerve at another level (Box 1). Carpal tunnel syndrome is a more common compression neuropathy, but it does not usually affect the little finger, and any muscle wasting would involve the thenar eminence. Cubital tunnel syndrome is the second most common compression neuropathy. Its incidence is reported as 23.2 and 18.9 per 100 000 per year for men and women, respectively.1
| Diagnosis | Differentiating factors |
|---|---|
| Carpal tunnel syndrome | Sparing of ring and little fingers, thenar muscle wasting, lack of interossei wasting, positive Phalen test and Durkan compression test |
| Cervical radiculopathy | Neck pain, reduced range of movement in the neck, sensory changes proximal to the wrist crease |
| Guyon canal syndrome | Sparing of sensation on the dorsum of the hand |
| Brachial plexus injury or neuritis | History of trauma, more widespread neurologic symptoms and signs |
| Thoracic outlet syndrome | Pain is a predominant feature; discoloration of the hand; symptoms related to strenuous exercise |
| Syringomyelia | Widespread neurologic symptoms and examination findings; cape-like loss of pain and temperature sensation |
| Pancoast tumour | Substantial smoking history; chest pain, breathlessness; hemoptysis; constitutional symptoms of malignancy; Horner syndrome |
| Less frequent causes include systemic conditions such as Guillain–Barré syndrome, motor neuron disease or polyneuropathy | Bilateral symptoms or unusual patterns of neurologic signs on examination |
In evaluating the cause of numbness in the hand, the handedness and occupation of the patient should be elicited, as well as any history of trauma or surgery to the elbow. A comprehensive systemic enquiry, including any family history of neurologic conditions, should be completed. Numbness and paresthesia are the predominant presenting features early in cubital tunnel syndrome. These symptoms are usually confined to the ring and little fingers, but may be accompanied by pain localized to the medial aspect of the elbow or radiating into the ring or little fingers. Intermittent symptoms, worse at night or with elbow flexion, are suggestive of cubital tunnel syndrome. In severe cases, sensory symptoms may be permanent, and patients may have signs of muscle atrophy and clawing in the hand. Patients may report a range of motor symptoms, including weakness or clumsiness when performing tasks involving fine motor skills.1 Bilateral symptoms, atypical patterns of weakness or altered sensation, and cervical symptoms should be specifically sought and should prompt consideration of alternative diagnoses (Box 1).
What tests for nerve function should be included in the examination?
Examination should include inspection for wasting of the hypothenar muscles and the interossei. Sensation should be tested throughout the hand, with reduced or altered sensation expected in the little finger and the ulnar half of the ring finger. The ulnar nerve may be palpated behind the medial epicondyle. Taking the elbow through a range of movement may unmask any instability or “snapping” of the nerve. Tapping a finger over the cubital tunnel may produce an abnormal Tinel sign, with altered sensation in the distribution of the ulnar nerve.2
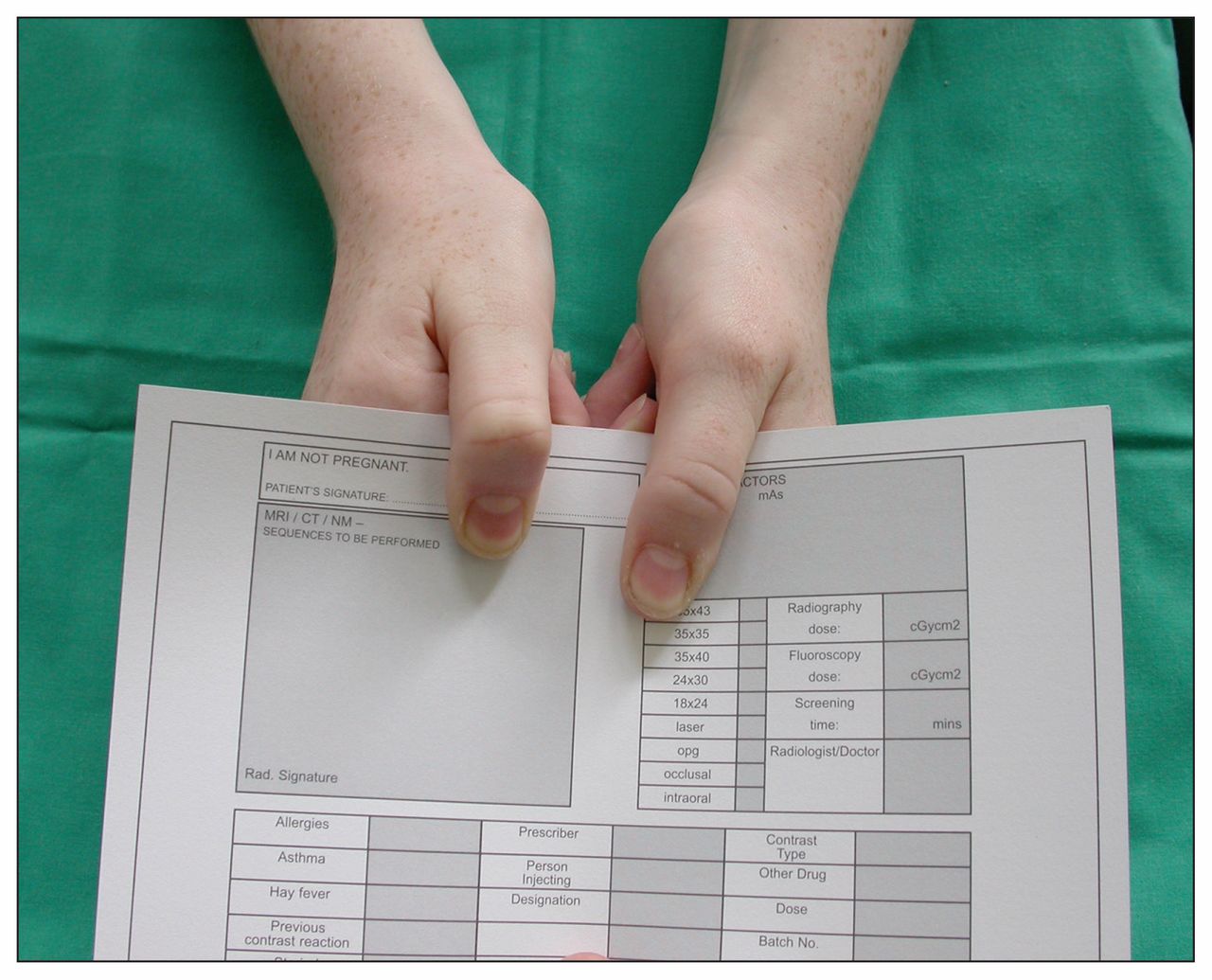
The Froment sign may be abnormal and results from weakness of the adductor pollicis muscle. When asked to grip a sheet of paper between thumb and radial border of the index finger, the patient compensates by flexing the thumb at the interphalangeal joint and recruiting the median nerve–innervated flexor pollicis longus muscle (Figure 1). Other motor signs include subjective or objective evidence of reduced grip strength and weakness of the ulnar nerve–innervated interossei. Asking the patient to cross their fingers is a simple way to elicit weakness of the interossei. When weakness is advanced, the unopposed action of the extensor digiti minimi muscle on the little finger may result in an abducted posture of the little finger. This is referred to as the Wartenberg sign.2

Positive Froment sign of the right hand.
Several additional provocative tests have been described in the literature, including the elbow flexion test and a combined flexion–compression test. A well-designed prospective study found these to be both sensitive and specific for cubital tunnel syndrome.3
Are any investigations required?
The diagnosis is a clinical one; a small prospective cohort study has shown the effectiveness of clinical examination alone in confirming the diagnosis.4 Electrophysiological testing may support the diagnosis, localize pathology and provide information regarding severity. It is particularly useful when there is diagnostic doubt and as part of a specialist assessment. Based on a well-designed systematic review, specificities of 95% or greater can be achieved with electrophysiological testing.5
Plain radiography of the elbow is indicated where there is a history of arthritis, trauma, malalignment or joint instability. It will usually be undertaken after specialist referral. In patients with a substantial smoking history, chest radiography should be performed to rule out a Pancoast tumour.
Should the patient be referred for surgery?
Mild symptoms can often be treated without surgery: simple strategies are effective for up to 90% of patients with only mild symptoms and no motor signs.6 Conservative measures include activity modification, avoidance of prolonged or repeated elbow flexion, nighttime splinting and patient education.6,7 One small cohort study showed that most patients with mild symptoms, followed for a mean of 22 months, experienced resolution of their symptoms within three months with conservative therapy.6 This supports anecdotal evidence that patients with mild symptoms can be safely counselled and managed in a primary care environment.6
In patients with moderate or severe cubital tunnel syndrome, conservative measures are less effective. One long-term prospective study showed that 33% of patients with moderate symptoms (i.e., intermittent paresthesia and measurable weakness) and 62% of patients with severe symptoms (i.e., persistent paresthesia and measurable weakness) did not respond to conservative management and required surgery.8
Early referral to a surgeon specializing in upper-limb surgery should be made for patients with a failure of conservative management, with any motor signs, and in whom activity modification is not feasible or desirable. There are several surgical techniques designed to decompress the ulnar nerve, but no consensus about the optimal treatment. Surgical options include decompression in situ or anterior transposition of the nerve, whether this is subcutaneous, intramuscular or submuscular. Based on the evidence from six small randomized controlled trials and two meta-analyses, a Cochrane review concluded that when surgical treatment is indicated, the reported results for each of these options are equivalent when undertaken by a surgeon experienced in the chosen technique.9
The case revisited
Despite simple measures for conservative management, including nighttime splinting and patient education to avoid provocative activities, the patient’s symptoms worsened. Based on the history and examination findings, the patient underwent in situ decompression of the ulnar nerve. He returned to work four weeks after the surgery and has made a full functional recovery.
Resources for patients
American Academy of Orthopaedic Surgeons online patient resource: www.orthoinfo.aaos.org/topic.cfm?topic=a00069
American Society for Surgery of the Hand online patient resource. Cubital tunnel syndrome: www.assh.org/public/handconditions/pages/cubitaltunnelsyndrome.aspx
British Society for Surgery of the Hand online patient resource. Cubital tunnel syndrome: www.bssh.ac.uk/patients/commonhandconditions/cubitaltunnelsyndrome
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Scott Middleton drafted the article, which both authors revised. Raymond Anakwe provided the figures. Both authors have approved the final version and are willing to act as guarantors for the work.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

