


See also practice article by Ramadhan and Tamilia on page 205 and at www.cmaj.ca/lookup/doi/10.1503/cmaj.110994
A 37-year-old woman with a 20-year history of primary hypothyroidism was referred by her family physician for assessment of a pituitary macroadenoma. About nine months earlier, a thyroid-stimulating hormone (TSH) level of 7.38 (normal range 0.27–4.20) mIU/L had prompted an increase in the patient’s maintenance dosage of levothyroxine (from 0.2 to 0.25 mg daily). Despite this increase, the patient gradually felt more tired and began to experience headaches, nipple discharge and weight gain.
The patient had a history of hypertension, gout, bipolar disorder and arthritis. Her medication history included atenolol, colchicine, quetiapine, bupropion, escitalopram, pregabalin, topiramate and hydroxychloroquine. She was not taking vitamins or herbal remedies.
The patient’s appearance was consistent with hypothyroidism, with dry skin and a delayed relaxation of her ankle reflexes. Laboratory investigations supported this diagnosis (TSH level > 100 mIU/L, free triiodothyronine level 2.5 [normal 3.0–6.5] pmol/L, free thyroxine level 5 [normal 10–24] pmol/L and prolactin level 79 [normal 3–29] μg/L). Magnetic resonance imaging (MRI) showed that the patient’s pituitary gland was homogeneously enlarged, suggesting hyperplasia (Figure 1). We increased the dosage of levothyroxine to 0.3 mg daily. Over the next few months, the patient’s symptoms improved and follow-up laboratory tests showed more normal results. A follow-up MRI showed that the pituitary mass had decreased in size (Figure 1). We subseqently learned that when our patient’s dosage of levothyroxine had been increased to 0.25 mg daily, her pharmacy had dispensed 0.025 mg daily rather than the prescribed dose.
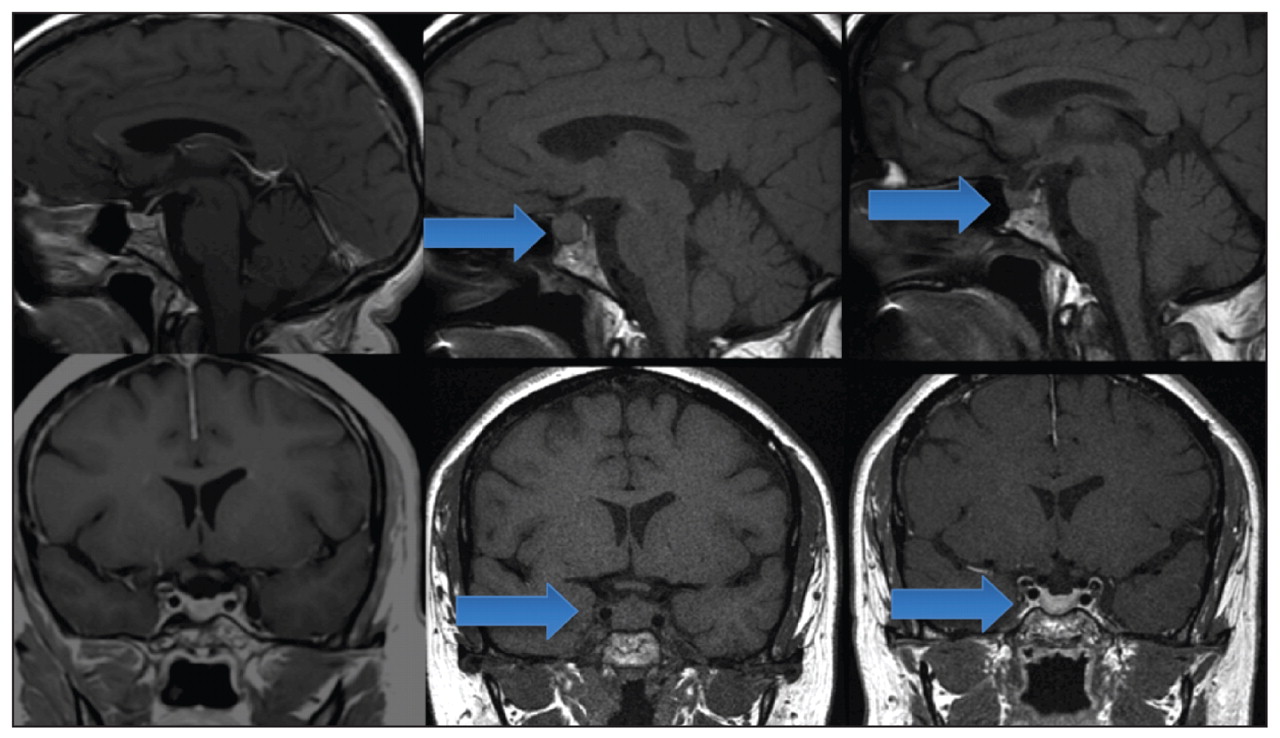
Magnetic resonance images showing sagittal and coronal sections of the head of a 37-year-old woman at baseline (left panel); at presentation, when her pituitary gland was homogenously enlarged (arrows) owing to severe clinical hypothyroidism (middle panel); and after her levothyroxine dosage was corrected (right panel), when the pituitary mass had decreased in size (arrows).
Image courtesy of Courtesy of Dr. Donald Lee
Severe primary hypothyroidism results in pituitary hyperplasia when thyrotropin-releasing hormone overstimulates pituitary thyrotrophs.1 Prolactin may also be secreted. Because imaging studies may not reliably differentiate between hyperplasia and macroadenomas,1 adequate clinical assessment is critical. Appropriate levothyroxine therapy may resolve the hyperplasia, thus avoiding the need for surgical intervention.1
Poor adherence, malabsorption and drug interactions are important causes of subtherapeutic responses to pharmacologic treatment. However, errors in dosing should also be considered, particularly when doses are dispensed in less than one unit.2 To avoid such errors, zeroes should be routinely placed before a decimal and drug units should be clearly written. Electronic prescriptions may improve legibility and facilitate drug calculations.2,3
Footnotes
-
Competing interests: Stan Van Uum sits on advisory boards for Novartis and Abbott Canada; he has received grants from Novartis and Genzyme; he has received payment for lectures and the development of educational presentations from Novartis and Eli Lilly; and he has been reimbursed for travel expenses by Novartis. No other competing interests were declared.
-
This article has been peer reviewed.
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

