


- © 2007 Canadian Medical Association or its licensors
Trichinellosis, or trichinosis, is acquired by eating raw or undercooked meat that contains larvae of the tissue-dwelling nematode Trichinella. Historically, pigs were considered to be the main reservoir of Trichinella, but a recent Canadian survey showed no evidence of Trichinella infection in domestic swine populations.1 Wild hosts have been associated with outbreaks of trichinellosis in Canada, including farmed wild boars, bears and walruses. Most outbreaks of trichinellosis in Canada have been due to Trichinella nativa, which is generally found in hosts from Arctic and subarctic regions and is resistant to freezing. Game animals commonly hunted in Canada that may be infected with T. nativa include black bears, grizzly bears, polar bears and walruses. In some areas of Canada, foxes, wolves and wolverines are eaten and may also be infected.2 Recent Canadian outbreaks occurred after recreational game hunters ate the meat of a black bear that was shot in northern Quebec3 and after 78 people in a northern Saskatchewan community ate bear meat.4
In 2005, we investigated an outbreak of trichinellosis in Victoria that was linked to the consumption of black bear meat. The bear was shot in Port Renfrew, 107 km northwest of Victoria, and the meat was frozen for at least 3 days before being barbequed, fried or stewed at 3 separate events. The first patient presented with a fever of unknown origin. The diagnosis of Trichinella infection was confirmed by serologic testing but not until the following month, when a second case was diagnosed. Among the 42 people who reported eating the bear meat, 26 probable cases were identified (62%). Probable cases were identified as people who had consumed the bear meat and reported clinical symptoms consistent with trichinellosis, including gastrointestinal symptoms, fever, muscle pain, headache and rash (Fig. 1). Of the 26 probable cases, 14 were confirmed by serologic testing. Drug therapy was prescribed to 17 people and included mebendazole (14 patients), albendazole (2) or amoxicillin (1).

Fig. 1: Rash from Trichinella nativa infection in Saskatchewan outbreak. Photo courtesy of Schellenberg and colleagues.
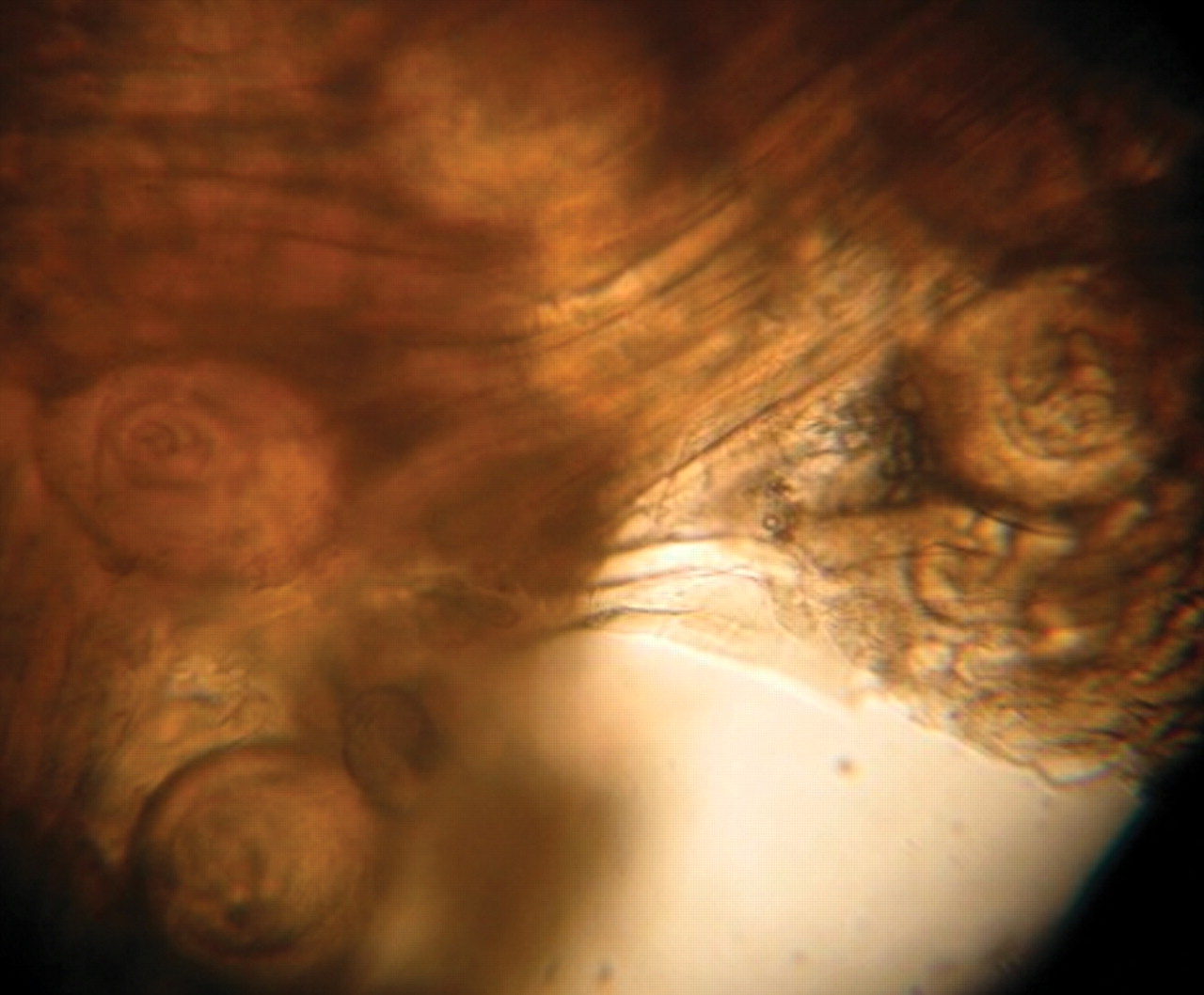
The leg muscle of the bear contained over 300 Trichinella larvae per gram (Fig. 2), and polymerase chain reaction identified the species as T. nativa.5,6 The bear meat had been frozen for up to 72 hours before being eaten; however, freezing is not adequate to prevent Trichinella transmission. Data collected from people who attended all 3 events indicated that infection occurred regardless of how often the meat was consumed (at 1 or more events), how much meat was consumed, the cooking method used or how well the meat was cooked. It is possible that other foods or surfaces were contaminated with raw meat during food preparation because infection occured in people who ate very well cooked (stewed) bear meat.
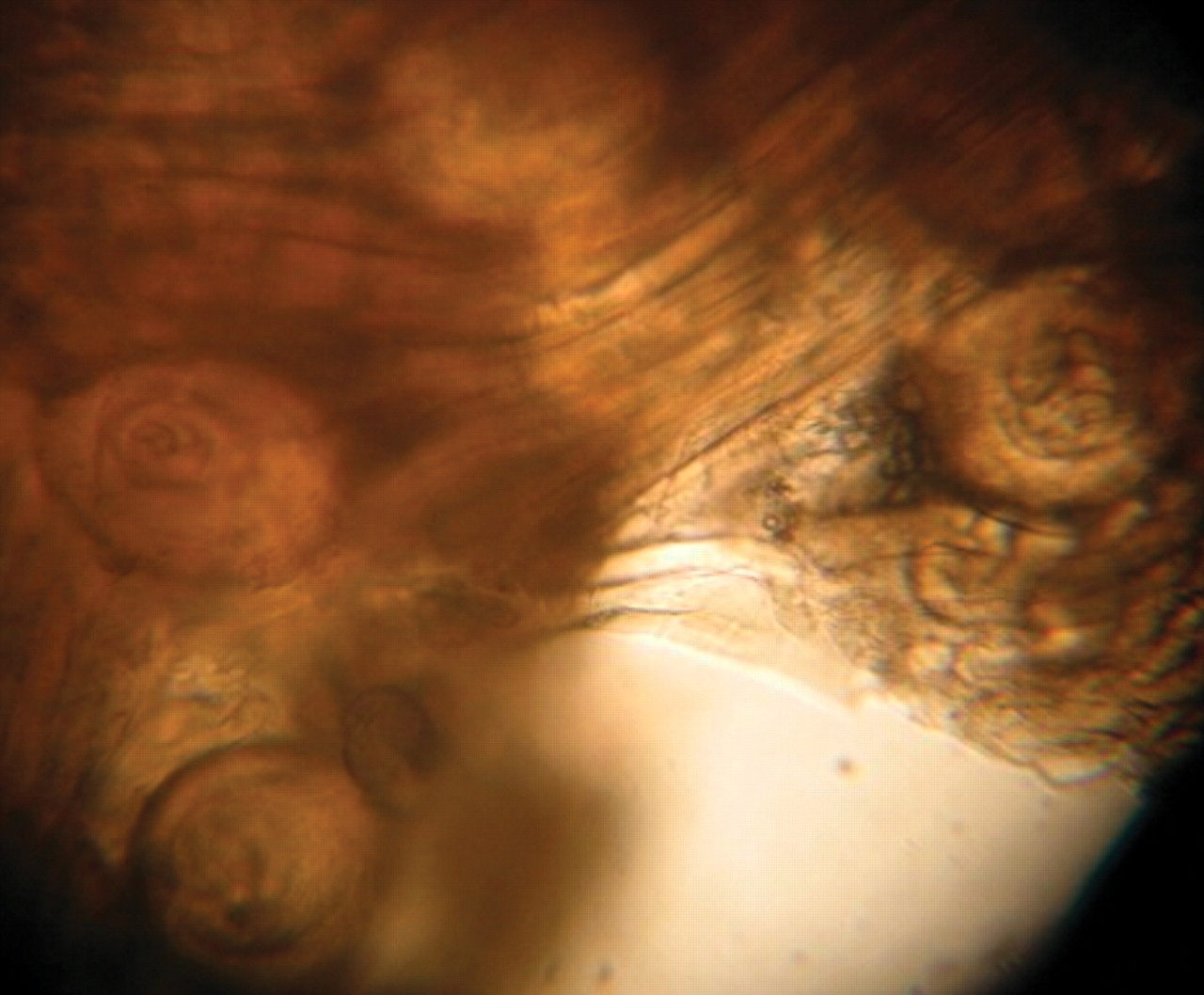
Fig. 2: Four encapsulated Trichinella larvae in muscle tissue of bear leg (original magnification × 100).
Clinical management
The incubation period for trichinellosis symptoms to appear is 7–21 days. Although an infected person may be asymptomatic, ingestion of a higher parasite load usually correlates with a shorter incubation period and with more severe symptoms. If clinical symptoms appear, they usually begin with several days of mild, nonbloody diarrhea, nausea, vomiting and abdominal discomfort (Table 1). Two to 8 weeks later, the host's immunologic reaction to larval migration into tissues can result in persistent fever, sweating, chills, periorbital edema, urticarial rash and conjunctival or subungual hemorrhages. Long-term effects depend on parasite load and site of infection. Myalgia is often present, and cardiac manifestations (e.g., myocarditis) may rarely occur later in the infection in moderate to severe cases. Eosinophilia is often substantial and appears early in the infection. Later, when larvae encapsulate in muscle tissue, increased serum creatine kinase and lactic dehydrogenase levels may be detected. Infection is confirmed when serologic testing identifies IgG antibodies against Trichinella; however, false-negative results may be obtained if serum is taken early in the infection, before antibodies have developed. A muscle biopsy is generally not required for diagnosis.7
Table 1.
Once Trichinella larvae become enclosed in cysts within muscle, the patient's clinical symptoms will begin to disappear, and antiparasitic and anthelmintic medications are ineffective. If trichinellosis is considered early in the differential diagnosis and is confirmed by serologic testing as soon as possible, anthelmintic agents such as mebendazole or albendazole may be useful in eradicating larvae-producing worms. Treatment of the patient's symptoms (e.g., corticosteroid therapy) may be required in some cases.8 If left untreated, the parasites will die within 2–5 years and become calcified. The long-term effects of trichinellosis include persistent or chronic muscle pain and impaired muscle strength.9
Prevention
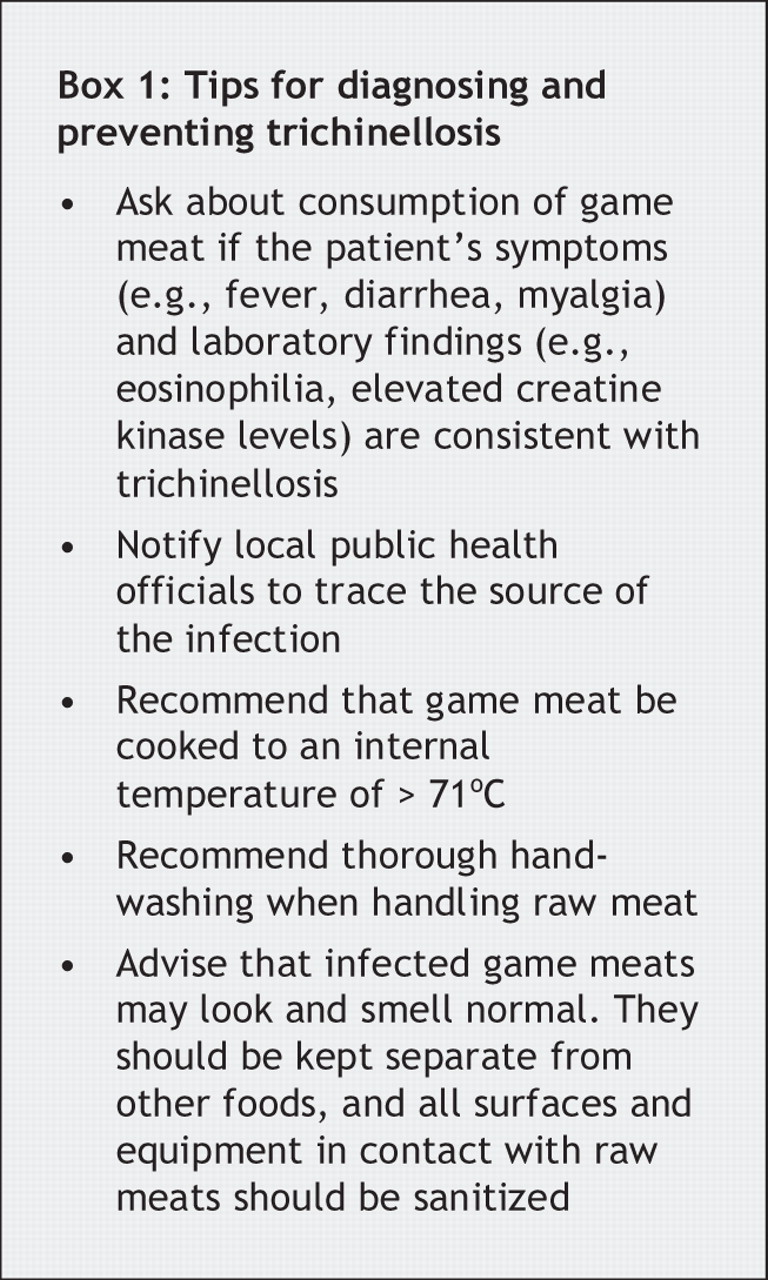
In the Victoria outbreak, the primary care physician of the index case did not enquire about bear meat consumption, and serologic testing was not performed until a second patient presented with similar symptoms and a history of bear meat consumption. The differential diagnosis should include trichinellosis if a patient reports a history of hunting or eating wild game and has symptoms and laboratory findings consistent with trichinellosis (Box 1). Serologic testing should be performed to confirm the presence of Trichinella. Antiparasitic and anthelmintic therapy should be started quickly because these medications do not affect parasite larvae once in muscle tissue. Freezing meat is not sufficient to prevent trichinellosis. Meat should be cooked thoroughly at a temperature of at least 77°C to achieve an internal temperature of 71°C. Public health officials should be notified if trichinellosis is diagnosed, and follow-up investigations are required to determine the source of this foodborne infection and to prevent further cases.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
More in this TOC Section
Similar Articles
Collections

