


Case 1: Eleven-year-old Alan has had problems at school for the last 18 months. He has severe problems with inattention and an inability to concentrate, and he cannot sit still for any length of time. Attention deficit hyperactivity disorder (ADHD) was diagnosed 10 months ago by his family physician, but treatment with escalating doses of methylphenidate (now 10 mg at breakfast and lunch) has been unsuccessful; he still experiences a continual and disruptive need to move about. For example, when watching television, he usually steps up and down continuously on the lowest step of the staircase adjoining the family's living room. He also seems unable to stay seated during dinner with his family. The problem is worse at the end of the day, and his mother describes him as having „restless legs” that make it difficult for him to get to sleep. He's often not rested the next morning, and his mother worries that, unless something is done, he may fail his school year.
Case 2: Scott, previously well and 17 years old, is referred back to his family physician from the emergency department to check a wound on his forehead received during a fight at a pub. Apparently 5 police officers were required to restrain him. He was kept in custody over the weekend, but he seems untroubled by this, saying he managed to sleep through most of the incarceration period. Scott denies using any street drugs and claims to have consumed only one drink the night of the fight. A normal blood alcohol level and negative toxicology screen result at the time of his emergency visit support this. He recalls having fallen asleep at his table at the pub and being woken up by a bouncer. He also recalls feeling briefly very confused, starting a fight and feeling out of control. Such a scenario — falling asleep suddenly and waking up in a state of confusion — has occurred several times in the past 2 years. Having dropped out of school in grade 10, he works helping to unload delivery trucks. He hopes to be allowed to drive on his own soon, but he is frankly worried about his frequent problems with somnolence.
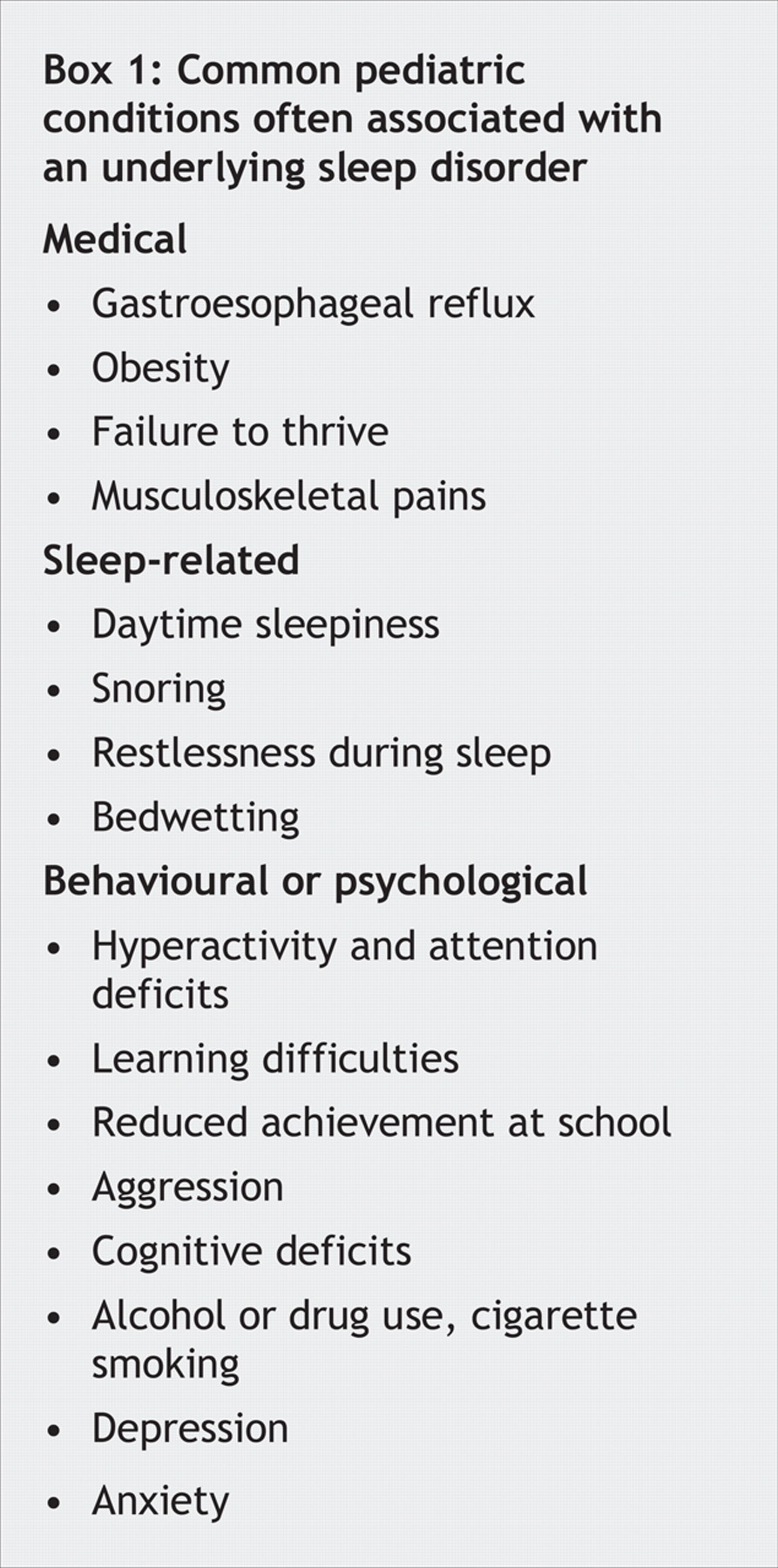
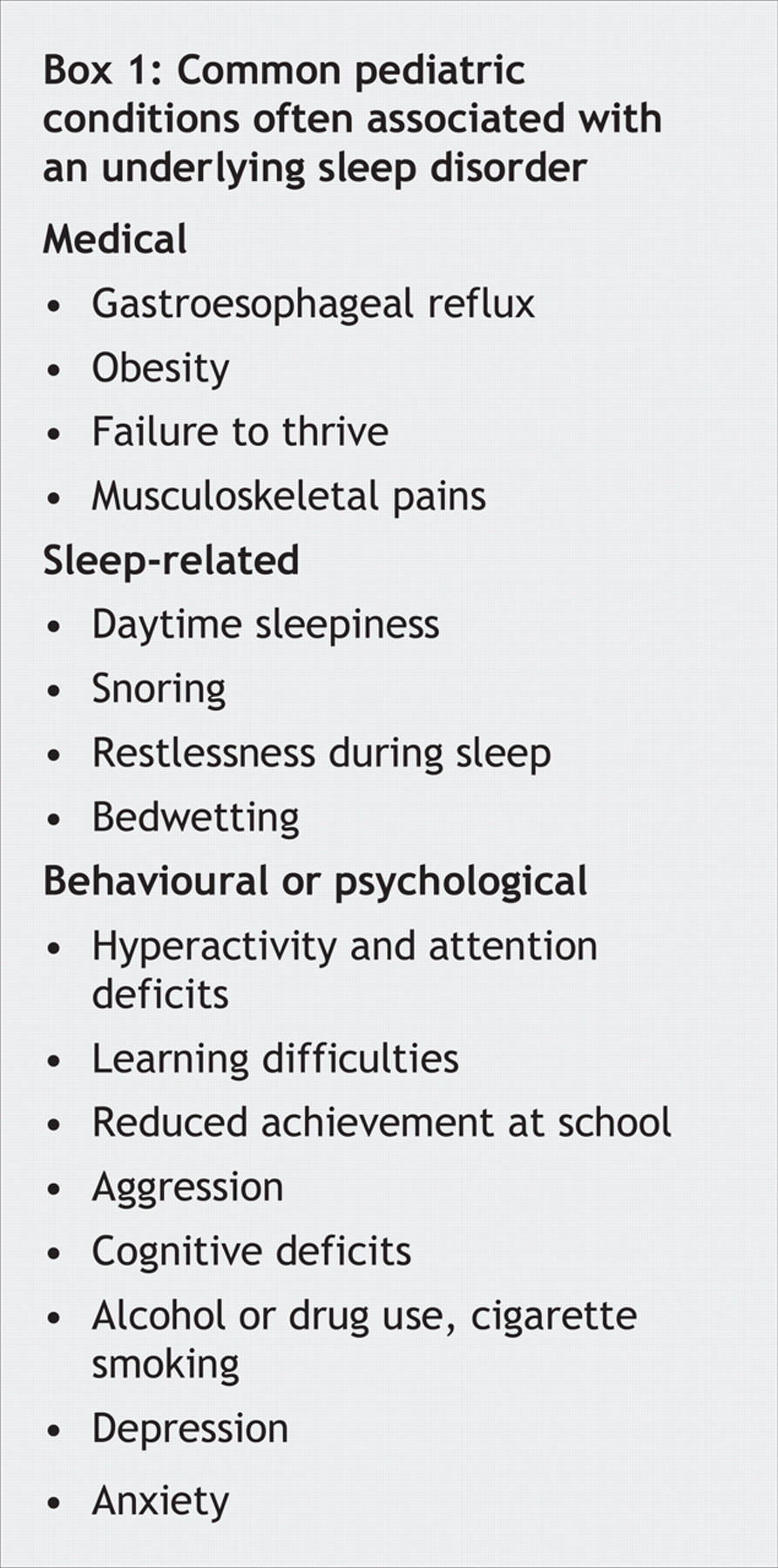
Insomnia and fatigue are common sleep-related problems in adult general practice. Sleep disorders are also common in pediatrics, with as many as 17% of adolescents having unrestorative sleep.1 However, many of these children may report seemingly unrelated problems. In one study of children ultimately found to have sleep disorders, almost a quarter initially presented with seemingly unrelated problems ranging from hyperhydrosis to academic deterioration.2 This echoes our experience in an academic sleep clinic, where many children present with a variety of problems that are often ultimately found to be related to an underlying sleep disorder (Box 1). A detailed history (Box 2), physical examination, laboratory tests and a sleep assessment involving polysomnography are usually required to help rule out other disorders and unmask these sleep disorders. We aim to highlight a few key sleep disorders that masquerade as common, nonspecific pediatric conditions, including behavioural problems and excessive daytime sleepiness.

Behavioural problems and symptoms of attention deficit hyperactivity disorder
Restless legs syndrome (RLS) and obstructive sleep apnea syndrome (OSAS) (Box 3) are 2 sleep-related problems that can lead to behavioural symptoms often misdiagnosed as an attention deficit disorder. Patients with RLS or OSAS have impeded restorative sleep and can experience increased daytime sleepiness and problems with inattention, inability to focus and distractability.3 These children may present with learning difficulties, aggression, cognitive deficits and bedwetting. Indeed, children who seek mental and motor stimulation to cope with their excessive daytime sleepiness may appear hyperactive but are quite refractory to pharmacologic therapy for ADHD such as stimulants.

Off-label pharmacologic treatments for pediatric RLS include dopaminergic agents (such as selegiline) (for a complete list see p. 31 in Fighting Fatigue and Sleepiness, listed in Additional Reading at the end of this article). These agents appear to reduce limb movements during sleep, which allows restorative sleep to occur and many children's secondary ADHD-like symptoms to improve. OSAS is often treated with measures including weight loss (for obese children) and correcting sleep position. Adenoidectomy or tonsillectomy is sometimes helpful and may also help to alleviate concurrent ADHD-like symptoms in some children with OSAS.3
Excessive daytime sleepiness
Although excessive daytime sleepiness is commonly perceived as simple „teenage laziness” or even depression, it may actually herald an underlying sleep disorder. Children who experience excessive daytime sleepiness often have reduced academic and extracurricular performance, so identifying and correcting the underlying problem is often desired by parents and teens alike. Two disorders that usually emerge in the teenage years and can cause excessive daytime sleepiness include delayed sleep phase syndrome (DSPS) and narcolepsy.
DSPS is a disorder of the circadian rhythm characterized by difficulties in falling asleep. Sleep onset may occur only in the early hours of the morning. If an affected person needs to awaken at a specific time in the morning (e.g., for school), sleep deprivation often results, and excessive daytime sleepiness is observed. The prevalence of DSPS is not known. It appears to be caused by an irregularity in the secretion patterns of melatonin, the hormone that controls the body clock. A sleep study can help to delineate the condition, but more definitive tests include a Dim Light Melatonin Onset study. In this test the patient's melatonin secretion rate is typically monitored using saliva samples taken in a dark room from 7 pm to 3–4 am. The usual increase in melatonin levels at 8–9 pm is delayed in adolescents with a phase delay disorder.
Narcoleptic patients can experience sleep attacks, and often cataplexy (characterized by episodes of a few seconds to a few minutes in duration of sudden loss of muscle tone) and hypnagogic hallucinations. The sleep attacks are experienced as excessive daytime sleepiness with irresistible urges to sleep for a few minutes (up to half an hour). The urge to sleep is not relieved by any amount of sleep taken the night before, but affected people may feel briefly refreshed after an attack. The prevalence of the condition varies according to ethnicity: around 1 in 3000 Europeans but 1 in 600 Japanese will experience the condition. Predispositions to narcolepsy are inherited, and although the exact cause is not clear, rapid eye movement (REM) sleep is abnormally regulated. Affected people may have chronic excessive daytime sleepiness between attacks. Attacks are sometimes prevented by staying mentally and physically active.
DSPS can be managed with melatonin therapy and behavioural strategies. Narcolepsy is often treated with stimulants such as methylphenidate and dextroamphetamine, the α-1 adrenergic agent modafinil (which increases alertness), antidepressants if the patient experiences cataplexy, or hypnotic agents (e.g., zopiclone) to help fragmented nocturnal sleep. Treating these underlying sleep disorders often corrects secondary problems of excessive daytime sleepiness and its associated academic and behavioural problems.
Case 1 resolved: Alan was referred to a sleep psychiatrist, who suggested the diagnosis of RLS. A sleep study confirmed the diagnosis. Alan's stimulant medication was withdrawn, and he was given with the antiparkinsonian agent selegiline. The restlessness in his legs improved dramatically, and he was able to sit for extended periods and pay attention during class. His academic performance correspondingly improved.
Case 2 resolved: By sleeping excessively and at inappropriate times, Scott was recognized as having classic signs of a sleep disorder. A sleep study showed that Scott had narcolepsy. Of particular note, he had REM-onset episodes in 3 of 5 Multiple Sleep Latency Tests carried out the day after his overnight sleep study. A test result for the HLA-DR2 DQw1 genetic markers found in almost all narcoleptic patients was positive. Although Scott had performed poorly at school, he was a talented mechanic. An intelligence test was conducted, and Scott displayed an IQ in excess of 120. On reflection he admitted that he had „slept through school.” His job loading and unloading vans allowed him to sleep in the truck en route to each delivery. Treatment of his narcolepsy with methylphenidate and subsequently modafinil relieved Scott's daytime somnolence problems. He joined an adult education program and eventually learned to read and write properly for the first time.
ADDITIONAL READING
• Shapiro CM, Ohayon MM, Huterer N, et al. Fighting fatigue and sleepiness. Toronto: Joli Joco Publications;2005
• Schapira AH. Restless legs syndrome: an update on treatment options. Drugs 2004;64:149-58
• Chervin RD, Archbold KH, Dillon JE, et al. Associations between symptoms of inattention, hyperactivity, restless legs, and periodic leg movements. Sleep 2002b;25:213-8
• Montgomery-Dorrns HE, Jones VF, Molfese VJ, et al. Snoring in preschoolers: associations with sleepiness, ethnicity and learning. Clin Pediatr (Phila) 2003;42:719-26
• Martinez-Salcedo E, Lloret-Sempere T, Garcia-Navarro M, et al. Narcolepsy in children. Rev Neurol 2001;33:1049-53
Footnotes
-
This article has been peer reviewed.
Acknowledgements: We thank Dr. Inna Voloh for her assistance.
Competing interests: None declared.
REFERENCES
In this issue

{kind=link}
{kind=link}
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

