Article Text

Abstract
Aims—To characterise the skeletal muscle changes in the neuroleptic malignant syndrome (NMS).
Methods—Detailed light and ultrastructural examination was carried out on skeletal muscle from three cases of NMS, two associated with recreational drugs (3,4-methlenedioxymethylamphetamine (MDMA, Ecstasy) and lysergic acid diethylamide (LSD)) and one with antipsychotic drugs (fluoxetine (Prozac) and remoxipride hydrochloride monohydrate (Roxiam)).
Results—The muscles were grossly swollen and oedematous in all cases, in one with such severe local involvement that the diagnosis of sarcoma was considered. On microscopy, there was conspicuous oedema. In some fascicles less than 10% of fibres were affected whereas in others more than 50% were pale and enlarged. There was a spectrum of changes: tiny to large vacuoles replaced most of the sarcoplasm and were associated with necrosis. A striking feature in some fibres was the presence of contraction bands separating segments of oedematous myofibrils. Severe endomysial oedema was also detectable. There was a scanty mononuclear infiltrate but no evidence of regeneration.
Conclusions—The muscle changes associated with NMS are characteristic and may be helpful in differential diagnosis.
- myopathy
- neuroleptic malignant syndrome
- fluoxetine
- remoxipride hydrochloride monohydrate
- Ecstasy
- LSD
Statistics from Altmetric.com
The therapeutic administration of neuroleptic drugs (antipsychotic agents and major tranquillisers) may cause a potentially fatal idiosyncratic response called the neuroleptic malignant syndrome (NMS), characterised by four signs—hyperpyrexia, extrapyramidal rigidity, alterations in consciousness, and autonomic instability.1–4 NMS occurs in 0.5–1% of all patients exposed to neuroleptics, but the mortality, which was more than 70% in the 1960s, has now fallen to 11.6% or less, because of increased awareness of the syndrome accompanied by immediate cessation of the offending drug, general supportive measures, and the therapeutic use of dopamine agonists and dantrolene.5 NMS may, however, also be associated with so called recreational drugs—especially 3,4-methylene dioxymethylamphetamine (MDMA), commonly known as Ecstasy—and the fall in deaths from neuroleptic drugs has been paralleled by a rise in deaths from MDMA.6–13 NMS is familiar to most psychiatrists but is not so well known to general physicians and surgeons.
Muscle involvement is a key component of NMS: intense muscle contraction is present from the onset of the condition1–4,14 and is responsible for respiratory or renal failure in fatal cases.1,3,15 The single most useful diagnostic criterion is an increased serum creatine kinase (CK), and values up to 100 000 IU/litre have been reported15 (normal is < 100 IU/litre). Myoglobinuria is one of the most useful prognostic indicators and when associated with renal failure there is a 50% risk of mortality.5 Nonetheless, the muscle changes in this syndrome have attracted very little attention; a large recent review concluded that non-specific atrophy of type 2 fibres is the main feature.16
We have recently examined skeletal muscle by light and electron microscopy in three acute cases of NMS, one associated with antipsychotic medication and the others with drugs of misuse. We describe here a characteristic picture of acute damage in which fibre oedema is the main feature, ranging from mild to severe, sometimes accompanied by contraction bands and necrosis and invariably associated with oedema of the endomysium.
Case histories and pathological findings
CASE 1
A 63 year old woman admitted to a psychiatric ward with depression and poor fluid and energy intake was given Roxiam (remoxipride hydrochloride monohydrate) and Prozac (fluoxetine hydrochloride). Three months after admission she developed transient tremors and twitches thought to be caused by anxiety or agitation. Twelve days later she was noted to have severe and generalised clonic movements. She rapidly became comatose. Her temperature was more than 40°C but there were no signs of infection. A diagnosis of possible NMS was made and she was transferred to a medical ward where she was found to be unresponsive, hypotensive, and to have a pyrexia of 39.1°C. She was transferred shortly afterwards to the intensive therapy unit but developed disseminated intravascular coagulation, severe hypoxaemia, and acute renal failure, dying 15 days after presentation.
Laboratory results and necropsy findings
The abnormal laboratory findings are given in table 1. At necropsy there was severe jaundice. The right and left vastus lateralis and forearm muscles were conspicuously pale and oedematous. Other muscles showed only mild oedema. The right lung weighed 1000 g and the left 900 g, with massive intra-alveolar haemorrhage and an organising fibrinous exudate on the pleurae. The kidneys were pale and swollen. Microscopy of the kidneys revealed acute renal tubular necrosis with conspicuous myoglobin detectable in renal tubules. There was an early bronchopneumonia and widespread features of adult respiratory distress syndrome (ARDS). Massive perivenular hepatic necrosis with cholestasis was also present.
Laboratory investigations
Muscle biopsies
Biopsies were taken from both vastus lateralis and forearm muscles at necropsy six hours after death. The tissue was surrounded by Arcton, cooled in isopentane, and frozen immediately in liquid nitrogen. It was stored at -90°C until use. Sections were cut at 8 μm and stained using haematoxylin and eosin, Gomori's trichrome, van Gieson, and histochemical stains (adenosine triphosphatase at pH 9.4 and 4.3, succinic dehydrogenase, and nicotinamide dehydrogenase).
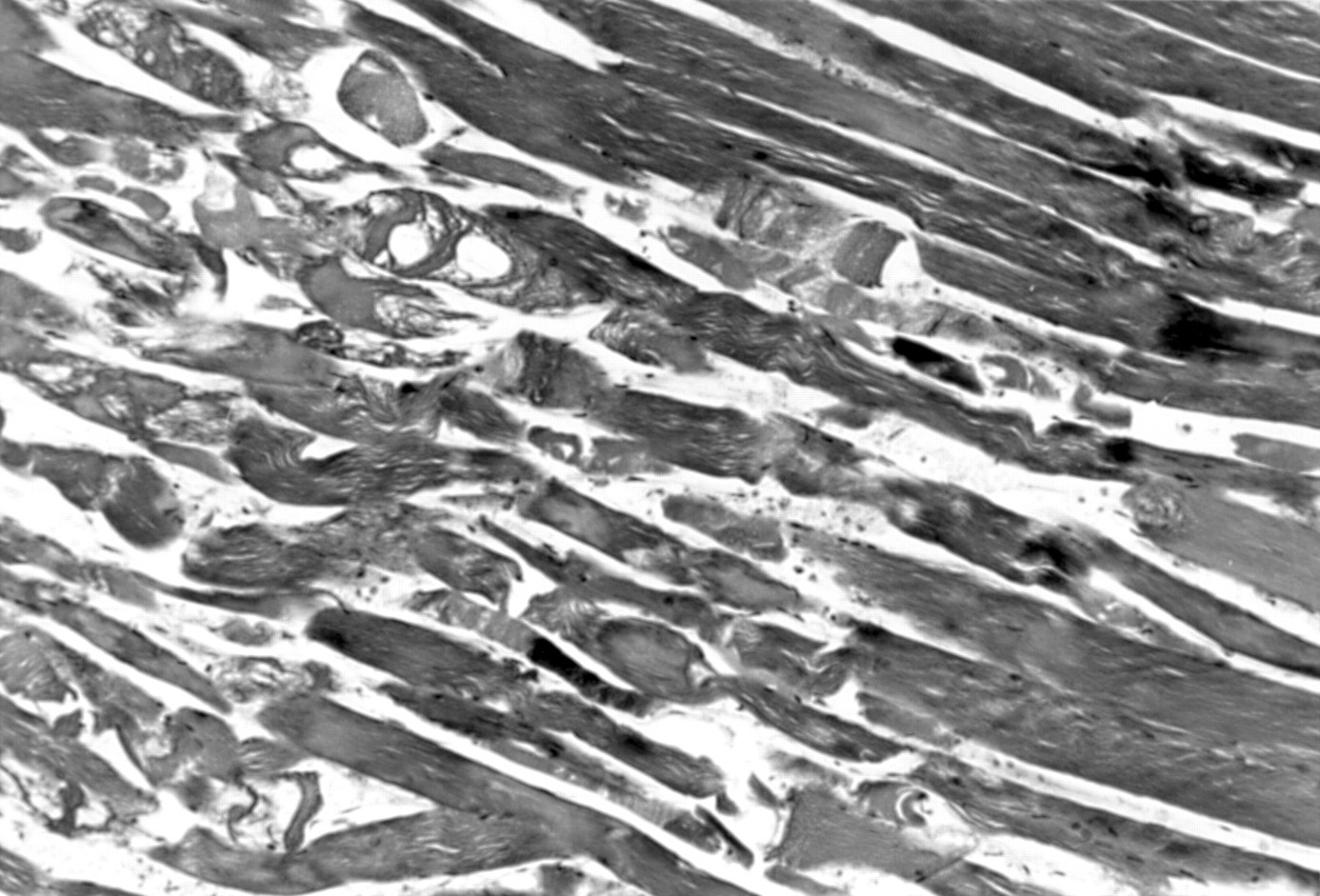
The amount of damage varied. In some parts whole fascicles were affected, while in others small groups amounting to approximately 10% of the area, or occasional single fibres, showed severe involvement (figs 1 and 2). It can be seen that the principal feature was oedema, with some fibres showing innumerable tiny vacuoles while in others a large vacuole occupied more than half the sarcoplasm. There was severe disruption of the intermyofibrillar network with the appearance of contraction bands (fig 2) and “ring-binden” (figs 3 and 4). The intrafibre oedema was associated with severe endomysial and perimysial oedema and a scanty mononuclear cell infiltrate (fig 5). No inclusions were present; lipid and glycogen were not increased.

Gross fascicular damage with severe disruption and necrosis of fibres in the left half of the field, associated with endomysial and perimysial oedema. There is relative lack of involvement on the right. Vastus lateralis, Mallory's trichrome, ×96.

Severely damaged fibre showing intermyofibrillary oedema and a band-like appearance (arrow) is seen adjacent to less damaged fibres. Vastus lateralis, Mallory's trichrome, ×94.

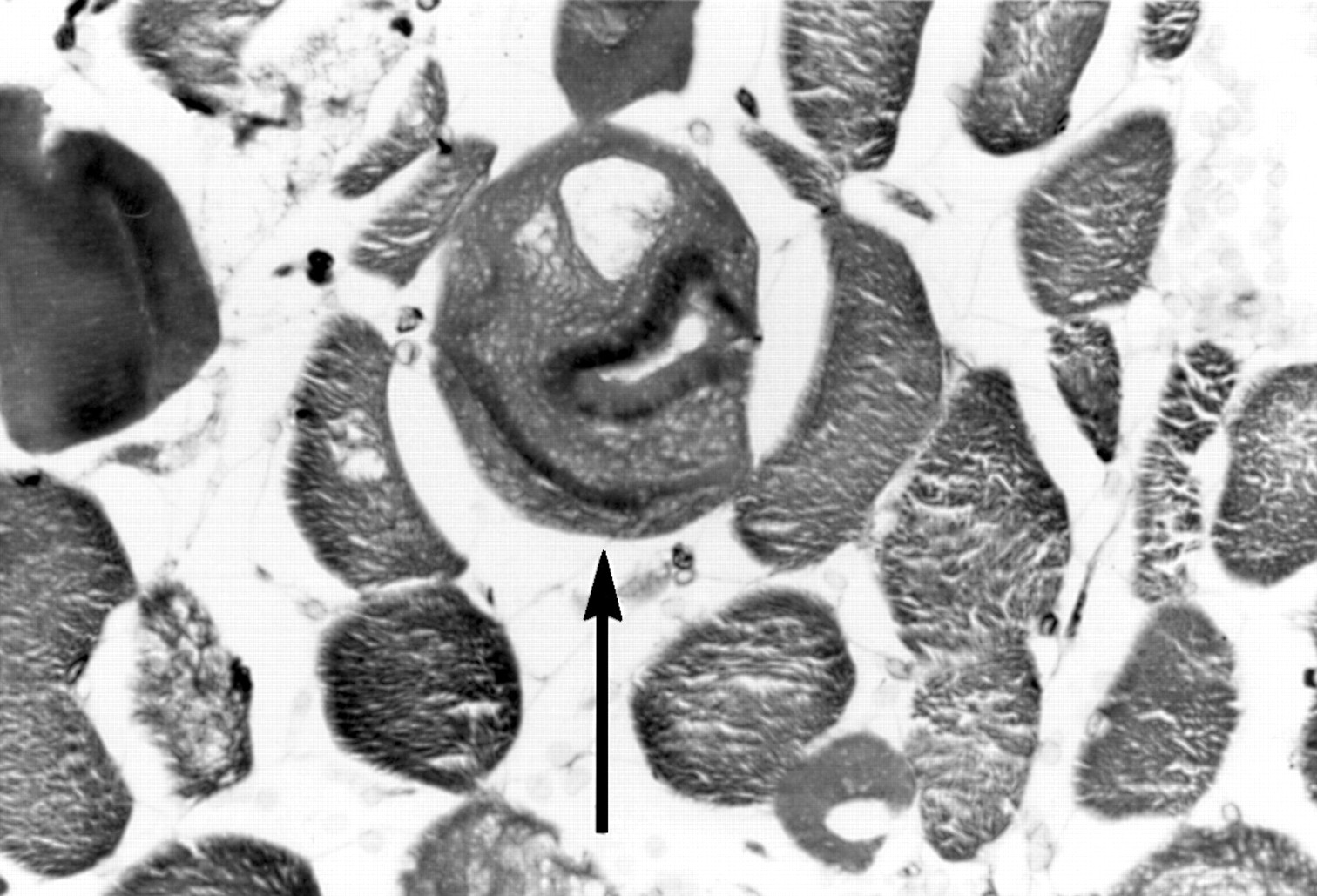
Central fibre (arrow) shows a large vacuole and myofibrillary disarray with a “ring-binden” effect. There is severe endomysial oedema. Mallory's trichrome, ×193.

Two fibres show a hyaline appearance (arrowhead) while in one (arrows) there is oedema and myofibrillary disarray with a “ring-binden” effect. Mallory's trichrome, ×193.

Central fibre (arrow) shows vacuoles of varying size, band-like appearance of disrupted myofibrillar network, and severe surrounding oedema with a few mononuclear cells. Mallory's trichrome ×382.
In the damaged areas both fibre types were involved. In unaffected fascicles, the usual mosaic pattern of type 1 and 2 was seen, with mild focal atrophy of type 2 fibres.
CASE 2
A 20 year old man was admitted complaining of pain and swelling of the left buttock and numbness of the left lower limb, which had been present for 24 hours. He also reported oliguria. He was a regular user of Ecstasy and had taken one tablet the evening before at a nightclub, followed by two units of beer and 60 mg of oral temazepam. He denied taking intravenous drugs. There was no relevant past medical history.
On examination, a large firm swelling was present over the left greater trochanter. He was unable to move his left leg or bear weight on it and hip flexion was reduced. Decreased power and absent ankle reflexes were noted and sensation was diminished below the left knee. The plantar response was equivocal. His temperature was 38.2°C. Abnormal laboratory results are given in table 1.
He was catheterised and started on intravenous fluids with dopamine infusion at 2 ml/hour and 100 ml of 10% mannitol. His chest x ray showed aspiration pneumonia of the right upper zone. An ultrasound scan of the buttock mass suggested the possibility of a tumour and a biopsy was taken. He was transferred to a renal unit for haemodialysis. Fifteen days later, by which time his condition had improved markedly, he took his own discharge. He did not complain of any residual symptoms during the ensuing two years. He then died of a drug overdose.
Muscle biopsy
A muscle biopsy was taken from the left buttock on the day of his admission. Since the lesion was thought to be a tumour, the fragments received, amounting to a 4 mm long core, were not frozen. Most of the tissue was fixed in 4% buffered formalin and processed routinely before staining with haematoxylin and eosin, Mallory's trichrome, and van Gieson. Tiny fresh fragments were placed in cold (4°C) 2% EM grade glutaraldehyde in Sorensen's buffer (pH 7.4) and left at 4°C overnight. Then, after washing and treatment with 1% OsO4, the tissue was dehydrated using graded alcohols, impregnated with Araldite resin, and polymerised in fresh resin mixture overnight at 60°C using a standard protocol. Sections (80–90 nm) were cut, stained in the conventional manner using uranium and lead, and examined in a Philips CM10 electron microscope.
Microscopy features were like those in the previous case, with up to 50% of fibres affected by a similar range of changes caused by oedema. Again oedema of endomysium and perimysium, with a scanty mononuclear cell infiltrate, was seen in the same areas. There was no evidence of any tumour. Ultrastructural examination (fig 6) confirmed the presence of severe architectural disturbance of the fibres, with areas of myofibrillary degeneration and a haphazard arrangement of fibrils. A range of features associated with oedema was present, from vacuolation of intracellular organelles (mitochondria, endoplasmic reticulum, T tubules) through lakes of oedema to complete disruption. Most mitochondria were normal, although a few were vacuolated. Intrafibrillar glycogen was abundant.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A fibre showing severe myofibrillary disarray and oedema with moderate glycogen is present.Left gluteus maximus, ultrastructure ×712.
CASE 3
A 21 year old unconscious man was admitted with severe bilateral extrapyramidal rigidity and extensor plantar responses. His temperature was 37°C. He had taken one tablet of lysergic acid diethylamide (LSD) a few hours previously, together with some alcohol. Abnormal laboratory results are given in table 1. The serum concentration of LSD was 69.9 ng/ml 24 hours after admission. A drug screen revealed no other drugs.
Needle biopsy of the vastus lateralis was carried out. Tissue was frozen, sectioned, and stained or processed for electron microscopy, as above. On light microscopy, there was mild generalised oedema, with occasional type 1 and 2 fibres showing tiny oedematous vacuoles. Short, irregular contraction bands could be seen in some fibres on longitudinal section. The usual distribution and mild size variation in fibre type were present. Histochemical stains revealed moderate glycogen and a little lipid. Ultrastructural examination showed severe architectural disturbance similar to case 2. There were areas where the cytosol was completely devoid of myofibrils and contained only oedema fluid. In other fibres, the fibrils were seen in bundles separated by oedema. The mitochondria and sarcoplasmic reticulum were vacuolated.
One year later a repeat muscle biopsy was carried out and was normal. This case has been briefly reported previously.17
Discussion
Early recognition and prompt treatment of NMS are essential as the features progress rapidly after onset, as illustrated by case 1, in which the outcome was fatal in spite of the diagnosis being made as soon as severe symptoms were present. The condition may be missed if the possibility of recreational drug use has not been considered. It has been reported that approximately half a million people a week in the United Kingdom take these drugs and they are widely available at “raves” and discos, where energetic repetitive non-stop dancing takes place in a hot humid atmosphere.12,17 These conditions result in a hypermetabolic muscle state, associated with excessive heat production and impaired cooling, and leading to hyperpyrexia—the sequence of events being similar to that of heat stroke.12 NMS is made worse by dehydration or physical exhaustion.15 The number of these cases is increasing.13
Muscle involvement plays a key role in NMS with a typical “lead pipe” hypertonicity and rigidity present from the onset.1–3,14 Muscle damage is responsible for the respiratory or renal failure in fatal cases: the former is precipitated by muscle rigidity and decreasing chest wall compliance leading to hypoventilation and aspiration pneumonia, while the latter is caused by massive rhabdomyolysis, myoglobinuria, acute tubular necrosis, and renal failure.15
The intense muscle contractions in NMS are caused by extrapyramidal stimulation following an acute fall in dopaminergic activity due to depletion or blockade.1–4 Dopaminergic neurones are a heterogeneous group found in the hypothalamus, where thermal regulation is sited, the striatum, where muscle tone is controlled, the frontal-limbic system, where consciousness resides, and the spinal cord, where dysfunction leads to dysautonomia.15 The original neuroleptics led to a reduction in central dopaminergic stimulation but the newer ones, including Prozac and Roxiam, although they have more specific antidopamine D2 receptor activity may still, albeit less frequently, produce NMS.17,18 These drugs have antiserotoninergic effects in addition and, as serotonin normally inhibits dopamine activity or blocks its release, a combination of effects may lead to the fall in dopamine activity.18 Neuroleptics have also been shown to inhibit the mitochondrial complex 1 enzyme, so that there may be a direct effect on muscle as well.19 Ecstasy is a ring substituted methylamphetamine which affects serotoninergic pathways,20 while LSD has a high affinity for serotonin receptors.21 Both may be associated with extrapyramidal muscle rigidity and rhabdomyolysis.20–22
The site of central nervous system involvement has been confirmed by imaging and necropsy studies. Single photon emission computed tomography (SPECT) scan analysis can be used to image dopamine receptor occupancy with the tracer (123I) iodobenzamide. In a case of NMS, blockade of D2 receptor occupancy was shown to correlate with the presence of extrapyramidal signs.23 In another case, focal neuronal necrosis in the hypothalamus of a young male with NMS was demonstrated.24
There have been three previous case reports detailing muscle damage in NMS, and four brief mentions of muscle biopsy results.8,12,25–27 Vastus lateralis in a 29 year old man with NMS from fluphenazine was examined at necropsy.28 It revealed endomysial oedema and scattered focal acute fibre necrosis. Lipid and glycogen were absent but mitochondria were normal. We reported similar findings previously in case 3.29 Muscle biopsy of another case showed sarcoplasmic vacuolation and denervation atrophy,26 while mainly normal fibres, with some variation in size, increase in internal nuclei, and atrophy of type 2 fibres, were reported in another.27 In two fatal ecstasy associated cases, normal muscle was present in one12 and non-specific atrophy of type 2 fibres in the other.8 In a large recent review of NMS, the muscle features have been summarised as non-specific.16
In distinct contrast to the above, however, is the case report of a 48 year old man given haloperidol for anxiety after a coronary angioplasty, who developed bilateral anterior and dorsal forearm compartment syndromes which necessitated fasciotomies.29 Widespread muscle necrosis and ischaemia were identified. He later made an uneventful recovery. This report supports our finding that there may be severe local involvement; in our case 2, the gluteal mass was thought to be a tumour.
We report here a dramatic picture in the acute phase of NMS, including a spectrum of fibre oedema from focal swelling through diffuse vacuolation to necrosis, and associated with severe endomysial oedema. Obvious contraction bands could be found in some fibres. The changes could also be seen at the ultrastructural level where all the intracellular organelles contained oedema and myofibrils were separated by lakes of fluid.
It might be suggested that these changes were artefactual but this is not the case for the following reasons. There was clinical evidence of severe muscle damage (increased serum CK concentrations and renal tubular myoglobin) and obvious muscle swelling, so localised that in case 2 it raised the possibility of a tumour. In case 1, the muscles were conspicuously pale, swollen, and oedematous at necropsy. On microscopy, there was no inflammatory exudate to account for this. The necropsy and biopsy specimens from all three cases showed the same changes, while other tissue processed at the same time, and a second biopsy taken after recovery in case 3, were completely normal.
Both fibre types were damaged in our cases. In unaffected areas, no abnormalities in fibre distribution or size were seen, apart from mild non-specific atrophy in case 1, and this patient had had a long inpatient hospital course before developing the syndrome.
The changes described here point to the possible pathogenesis. It is postulated that aerobic metabolism is exhausted by the intense rigidity and repetitive contractions. Glycogenolysis is then initiated, followed by mobilisation of free fatty acids. When these become depleted, membrane integrity cannot be maintained. There is an inadequate supply of the high energy substrates needed for the reuptake of calcium ions from the sarcoplasmic reticulum and it becomes leaky. Fibre oedema occurs. At the same time, calcium ions accumulating in the mitochondria activate proteases and fibre necrosis follows. All the effects described are made worse by the inexorable rise in core temperature caused by the muscle activity and its accompanying hypermetabolic state.18
The findings reported here can be compared with those in two other hyperpyrexic syndromes: malignant hyperthermia and heat stroke. In malignant hyperthermia, mostly non-specific changes have been reported,30 but in one recent fatal case, similar segmental necrosis and hypercontraction bands were detected.31 Although the mechanism of damage is different, as the primary lesion is an abnormality in the ryanodine channel of the muscle fibre resulting in excessive release of calcium through the sarcoplasmic reticulum, it is likely that there is a common final pathway of necrosis, owing to the accumulation of calcium ions.18 In heat stroke, there is undoubted rhabdomyolysis32 but no recent studies of muscle histology have been reported.
Acknowledgments
We are most grateful to Dr I A R More of the Department of Pathology, Glasgow University, for the ultrastructural investigations.