Article Text

Abstract
Background Key Information Summaries (KIS) were introduced throughout Scotland in 2013 so that anticipatory care plans written by general practitioners (GPs) could be routinely shared electronically and updated in real time, between GPs and providers of unscheduled and secondary care.
Aims We aimed to describe the current reach of anticipatory and palliative care, and to explore GPs’ views on using KIS.
Methods We studied the primary care records of all patients who died in 2014 in 9 diverse Lothian practices. We identified if anticipatory or palliative care had been started, and if so how many weeks before death and which aspects of care had been documented. We interviewed 10 GPs to understand barriers and facilitating factors.
Results Overall, 60% of patients were identified for a KIS, a median of 18 weeks before death. The numbers identified were highest for patients with cancer, with 75% identified compared with 66% of those dying with dementia/frailty and only 41% dying from organ failure. Patients were more likely to die outside hospital if they had a KIS. GPs identified professional, patient and societal challenges in identifying patients for palliative care, especially those with non-cancer diagnoses.
Conclusions GPs are identifying patients for anticipatory and palliative care more equitably across the different disease trajectories and earlier in the disease process than they were previously identifying patients specifically for palliative care. However, many patients still lack care planning, particularly those dying with organ failure.
- Supportive care
- Chronic conditions
- Home care
- Service evaluation
- Terminal care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Anticipatory and advance care planning is about ‘thinking ahead’. It encourages practitioners to work with patients, carers and relatives to plan for the right person to do the right thing, at the right time, to achieve patient goals, facilitating shared decision-making and person-centred care in the appropriate setting. Planning ahead is recognised as being central to the provision of palliative care.1
With ageing populations and rising multimorbidity, general practitioners (GPs) are caring for increasing numbers of patients with complex conditions approaching the end of life. Even in countries where palliative care is relatively well developed, most people still do not benefit from palliative care before they die. We previously reported that only around 20% of people with non-malignant illnesses were identified for generalist palliative care in 2011 in Scotland, and that this varied greatly from 75% in cancer to 20% in dementia/frailty and 19% in organ failure.2 Such patients were identified just weeks before death. This is illustrated in figure 1. Considerably fewer than this received specialist palliative care. These findings illustrated the need for the WHO resolution published in 2014, that palliative care should be integrated into the care of people with all advanced conditions from an early stage.3

Percentage of patients on the general practice palliative care register at death, according to illness trajectory and if so when they were placed on the register.
Since 2012, the Scottish Government has funded two new initiatives which together aim to extend generalist palliative care to all people who might benefit and to improve care for people with advanced illness earlier rather than later and in all settings. These are the Scottish Palliative Care Directly Enhanced Service (DES) and the Key Information Summaries (KIS) for anticipatory care (see box 1 for a summary). The specific inclusion of anticipatory care planning in the latest Scottish payment contract for GPs provides a framework for identifying high-risk patients. This planning uses tools such as the Scottish Patients At Risk of Readmission and Admission score (SPARRA)4 and the Supportive and Palliative Care Indicators Tool (SPICT), which has been validated.5 ,6
Details of the two initiatives to promote anticipatory and palliative care in Scotland
The Scottish Palliative Care Directly Enhanced Service has encouraged general practitioners (GPs) to identify more patients with non-malignant disease for palliative care by supporting them to use the Supportive and Palliative Care Indicators Tool (SPICT)5 to trigger them adopting a palliative care approach and to report specifically on numbers of non-malignant patients placed on their GP palliative care register.
The Scottish Key Information Summary (KIS) is a new IT development in NHS Scotland pioneering a shared medical record between healthcare professionals. It was introduced into all GP practices across Scotland in 2013 and allows selected parts of the GP electronic patient record to be shared with the wider NHS using a template within the GP clinical system. Patients with the most complex health and social care needs are selected to have a KIS written to capture key points of their anticipatory care plans. These include details of medical diagnoses, medications, carers, social care and next of kin details, baseline function and cognition, understanding of illness, wishes about resuscitation and place of care and any drugs or equipment at home. It has a small extra section for palliative care which details any anticipatory prescribing and is designed to be added to over time as the patient's clinical condition progresses. The KIS is now available when the patient consents to be viewed by secondary care, community teams, NHS24, the GP out-of-hours service, the Scottish Ambulance Service, hospital pharmacies and some hospices.
We aimed to better understand how the KIS was facilitating anticipatory and palliative care among patients approaching end of life, the current reach of anticipatory and palliative care, and to explore views of GPs on using KIS in practice.
Methods
We recruited nine GP practices across NHS Lothian to incorporate a mix of sociodemographic status and practice sizes.
Quantitative data collection and analysis
Participating practices provided the researcher with a list of all patients who had died in 2014. The principal researcher, JT, a GP with research training, accessed GP clinical records to review the notes of all deceased patients to see if a KIS had been completed. She also recorded which components were completed, and when, in relation to death. Case notes were reviewed to identify which of the three main disease trajectories—cancer, dementia/frailty or organ failure—the patient was on at time of death. JT also examined whether the patient had multimorbidity (two or more chronic conditions) and their place of death. Patients with sudden unexpected deaths were excluded from the analysis.
Logistic regression was performed by AL. The binary outcome of the logistic regression model was hospital death or death outside of hospital (elsewhere). The estimated ORs of patients dying in hospital were adjusted for a cluster of practices by means of a logit link in a binomial distribution of a robust generalised estimating equation and an exchangeable correlation structure.7 All analyses were performed using STATA software (V.11.1; StataCorp LP).
Qualitative data collection and analysis
JT, revealing that she was a GP interested in palliative care, also sought via the practice manager to interview a GP from each practice who was experienced in using a KIS (see box 2 for the interview schedule). Interviews were conducted face to face, lasting from 10 to 30 min, digitally recorded and transcribed verbatim together with field notes. Transcripts were analysed by JT for key topics and a priori and emerging themes.8 To increase reflexivity, JR, an experienced qualitative researcher, also analysed one-third of the transcripts and discussed the coding and analysis strategies with JT. Throughout the data analysis process, emerging themes and the coding tree were discussed with the multidisciplinary research steering group through regular meetings.
Semistructured interview schedule
How long have you worked in this practice as a general practitioner (GP)? How long have you been working as a GP?
Can you tell me how your practice uses the Key Information Summary (KIS) for anticipatory care planning?
How do you decide when to start a KIS? Do you use the Scottish Patients At Risk of Readmission and Admission (SPARRA) data/Supportive and Palliative Care Indicators Tool (SPICT)/suggestion from hospital?
Do the GPs complete the KIS themselves or are other team/admin members involved with them?
How do you deal with issues of consent and does this pose any challenges when completing a KIS?
What would trigger you to complete a Palliative Care Summary?
What about patients with non-malignant conditions? Do you find them more difficult to identify than those with cancer?
Have you received any formal training (including communication skills training) in discussing anticipatory care with your patients?
Do you think such training would be helpful, and if so are you aware of any?
What might influence your decision to attend such training?
What are your thoughts on the KIS and how do you find it to use in practice?
How time-consuming is it and does this factor into your decisions to complete/which parts to complete?
How does your practice run your KIS and Palliative Care meetings
Who attends?
How do you decide which patient to discuss?
Are they useful?
How do you find communication between primary and secondary care around KIS?
Does this help your decision to use the KIS?
Is it different for patients with and without cancer ?
Do you get much feedback from secondary care/out-of-hours about your KIS?
What would you do to improve the current service if you were given the chance?
Ethical considerations
The Caldicott guardian approved the process of accessing notes of deceased patients which helped consenting practices to feel able to participate. Permission from the South East Scotland Research Ethics Service to proceed with this study as a service evaluation, and ethical approval from the University of Edinburgh Ethics Review Group were granted.
Results
Quantitative results
Sample characteristics
A total of 605 deceased patients from the nine practices were identified, after excluding sudden unexpected or unexplained deaths. The median age was 81 years (IQR 72–92 years). Of these, 35% were identified as dying with cancer, 31% with dementia and/or frailty and 34% with organ failure. In total, 85% were suffering from multimorbidity (table 1). GP practices ranged in size from 5691 to 11 473 patients (table 2).
Patient sample characteristics
General practice characteristics
Identification for anticipatory care
Practices varied greatly, identifying between 92% and 36% of patients for anticipatory care (ie, having a KIS). Overall, 60% of patients had a KIS completed prior to death (table 3). The proportion of patients with a KIS was highest for those with cancer (74%), and lowest for those with organ failure (41%). KIS were started a median of 18 weeks before death.
Percentage of patients with different components of the KIS completed at death, and if so when discussed, according to illness trajectory
Over half of all patients who died had an anticipatory care plan (58%). Again, patients with cancer were most likely to have an Anticipatory Care Planning (ACP), whereas those with organ failure were least likely. ACPs were started a median of 15 weeks before death, approximately 3 weeks after the KIS was started.
Overall, 40% of deceased patients had the Palliative Care Summary (PCS) part of the KIS completed, and this occurred a median of 11 weeks prior to death. Those with cancer were most likely to have a PCS (62%), whereas those with organ failure were least likely to have this (22%). Figure 2 displays the differences in levels of anticipatory and palliative care by illness trajectory.

Percentage of patients with a Key Information Summary (KIS) and with a Palliative Care Summary (PCS) at death, according to illness trajectory and if so when the KIS and PCS were started.
Around half of all patients who died with cancer or frailty/dementia had a Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) form completed prior to death in contrast to only 25% of those with organ failure. Only 29% of patients had their preferred place of death recorded, and 23% had their preferred place of final care recorded. Patients with cancer were most likely to have had a record of both these preferences, whereas patients with organ failure were least likely (table 3).
Place of death
Overall, 50% of patients died in hospital (table 3). Logistic regression was performed to assess the impact of illness trajectory on the likelihood of dying in hospital versus dying in another location, adjusting for practice cluster. The odds of dying in hospital for patients with organ failure was higher than the odds of dying in hospital for patients with cancer (OR=2.30, 95% CI 1.26 to 4.18), or those with dementia/frailty (OR=2.25, 95% CI 1.13 to 4.51).
Anticipatory care and place of death
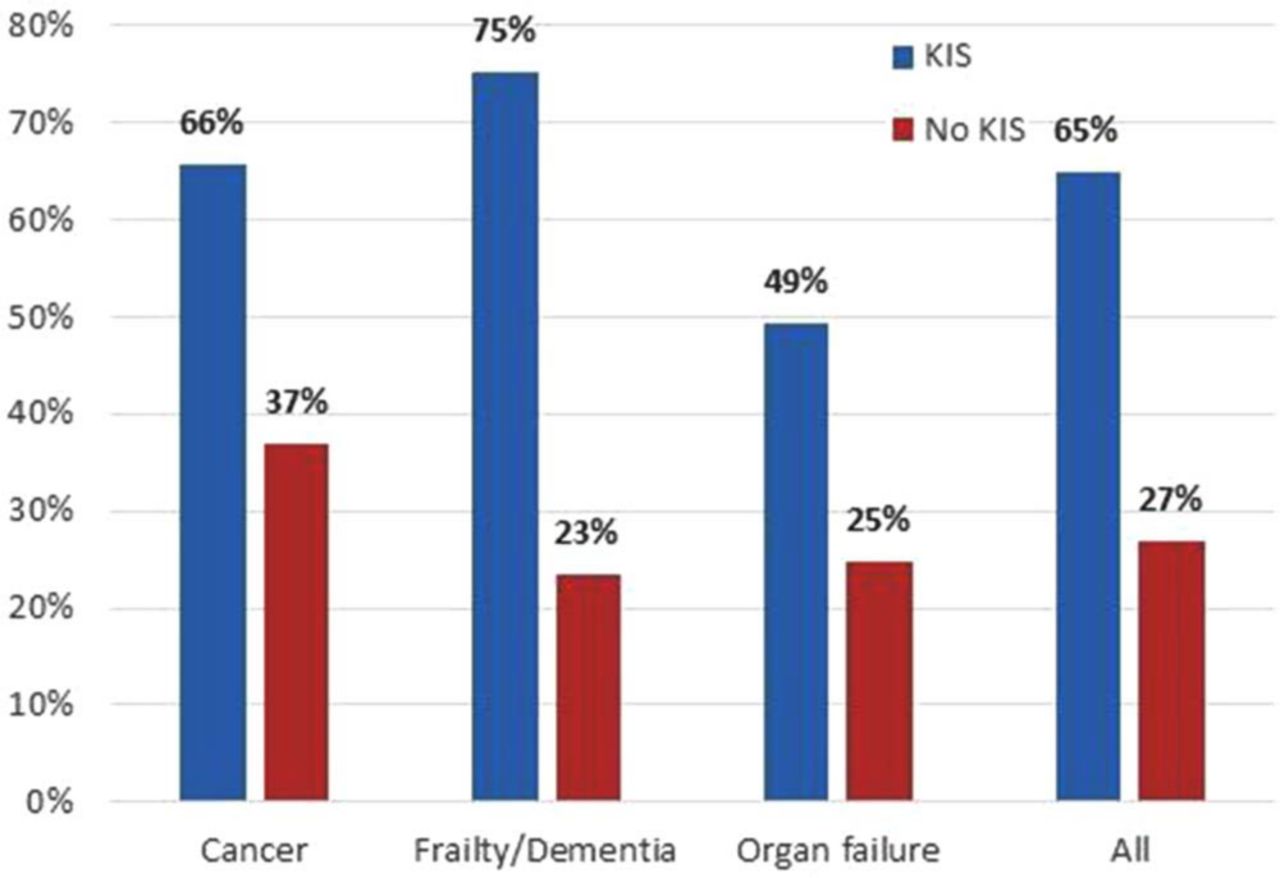
Across all trajectories, a higher proportion of patients with anticipatory care (ie, with a KIS) died outside of hospital compared to those with no KIS. Overall, 65% of patients with a KIS died in a location other than hospital, compared to only 27% of patients who had no KIS (figure 3).

{kind=link}
{kind=link}
{kind=link}
Deaths in the community: percentage of patients with a Key Information Summary (KIS) or no KIS on each trajectory who died in a location other than hospital.
Logistic regression was performed to assess the impact of having a KIS, a preferred place of care recorded or a preferred place of final care recorded on the likelihood of dying in hospital versus dying in another location, adjusting for practice cluster (table 4). The odds of dying in hospital were over 5.5 times higher for patients without a KIS compared to those with a KIS (OR=5.59, 95% CI 3.31 to 9.42). The odds of dying in hospital were nearly seven times higher for those without a preferred place of care record, compared to patients with a recorded place of care preference (OR=6.61, 95% CI 3.41 to 12.83). The odds of dying in hospital was 7.6 times higher for patients without a record of preferred place of final care compared to patients with a recorded preference (OR=7.6, 95% CI 4.27 to 13.55).
Univariate analysis of potential predictors of dying in hospital, adjusted for practice cluster
Qualitative results
JT conducted interviews with four male and six female GPs who had been qualified as GPs for an average 18 years (range 2–30) and had worked in their current practice for 12 years (range 1–23).
Opinions about KIS
In general, GPs thought the KIS was useful, although not always intuitive to complete; “I think it's one of the bits of paperwork that is useful as opposed to being a pain in the neck” (GP6).
Various methods were used to identify patients for KIS with most practices using the SPARRA data4 as part of this process. Other patients were identified opportunistically or through regular multidisciplinary team (MDT) meetings.
In general, they found that patients were happy to consent and positive around the idea of data sharing in this way. “Generally it's very positively received in my experience” (GP4).
Anticipatory and palliative care issues
GPs discussed difficulties with ensuring that the KIS was well completed and kept up to date, acknowledging that a good ACP can be hard to do. One GP commented that what was written in a KIS tended to focus more on what clinicians, as opposed to patients, might see as important. “I think in general if you look through some of them we're good at putting in the medical background. It's the anticipatory kind we're not always particularly great at that—unfortunately probably the most important bits” (GP 3).
There was a feeling that a well-written free text summary within the KIS was the key to facilitating good anticipatory care, and was probably more important than ‘ticking all the boxes’ or identifying patients specifically for palliative care. Several participants stressed the importance of continuity of care. “I think the bottom line is, I would say, it needs to be the clinician that really knows the patient, sees them on a regular basis that needs to be doing the ACP” (GP8).
GPs recognised challenges in identifying patients for palliative care, particularly those with non-malignant diagnoses. “You maybe just manage them [non-cancer patients] and you don't really think about them as perhaps benefitting from palliative care” (GP9), although confidence varied and several mentioned feeling that they were improving with this. A few commented that it was often recognised retrospectively that palliative care should have been started or could have been started earlier. “Fairly frequently when we do SEA [significant event analysis] of palliative care cases, almost always you say in retrospect we could have started the whole palliative process a bit sooner, but it involves difficult conversations and facing up to truths that people find difficult to face up to sometimes” (GP 4).
Access of KIS by out of hours and secondary care services
In general, GPs felt KIS were particularly useful for GPs working out of hours (OOH). “Certainly OOH are good, they very frequently will feedback they've had a good ACP so that's useful” (GP 3). GPs who also worked OOH commented on finding them useful when working in this setting.
GPs were less confident about access to KIS in hospitals “I often feel secondary care don't know it's there or are not using it. We've come across that a couple times where we've had patients who were admitted and it was clear they hadn't known to access that or hadn't used it” (GP 3). They reported receiving little or no feedback from hospital services. “The communication is one way, it's from us to secondary care at the moment” (GP 5).
Areas for improvement: IT, training and communication
While most felt that KIS were an improvement on previous methods for data sharing of anticipatory care, there were still issues with integration into GP clinical systems and improving ease of use. “Issues around the layout (in the computer systems are) difficult, can't blend very well” (GP 2). None of the GPs interviewed had had any formal training around discussing and delivering anticipatory care.
There was a desire to see increased use of KIS by secondary care. GPs would welcome increasing dialogue between themselves and other MDT members being able to contribute more actively to anticipatory care planning and KIS and what makes a good care plan. “It would be good to get feedback on if this is a good ACP or this isn't great or we need a bit more information. And better communication from secondary care, on patients they have discharged who are at risk of going back in, to have an ACP” (GP 10).
Discussion
When comparing the 2014 findings in this present study with 2011 data from a similar group of 10 Scottish practices, we found that patients had a much greater chance of being formally identified for an anticipatory or palliative care approach prior to death than before the KIS was introduced. Moreover, we previously reported that only 20% of patients with frailty/dementia were identified for palliative care, and this was at a very late stage—median of 2 weeks before death. However, this study shows that 35% of patients with frailty/dementia had been identified for palliative care, a median of 10 weeks prior to death.2 A comparison of figures 1 and 2 illustrates these and other differences.
However, despite improvements, many patients, especially with organ failure, were still not documented as identified for an anticipatory approach. Earlier identification helps a series of conversations to take place over time, as we noted in the progressive completion of the KIS in this study, at a pace that suits individual patients, rather than rushed discussions during the last days or weeks of life. As more parts of the KIS were progressively completed, the OR of dying in a location other than hospital for patients with a KIS, compared to those with no KIS, increased.
Surprisingly, slightly fewer patients with a cancer diagnosis were identified as ‘palliative’ than previously.2 GPs commented that it was the identification for anticipatory care, and the creation of a meaningful ACP, that was of prime importance in managing these patients, rather than being identified specifically for palliative care. Given the ageing population and increasing number of people9 with multimorbidity, there is a shift from disease-focused interventions, which have tended to favour patients dying from cancer for palliative care, towards a more generic goals of care approach. This may be the way forward when thinking about how to deliver equitable care for all in their last phase of life.10 It is not always necessary to talk about dying.
Previous literature has shown that care planning for patients at home, in care homes or at hospital discharge can reduce hospital admissions and increase the chance of dying outside of hospital.11 ,12 Advance Care Planning is sometimes deferred by professionals for fear that the patient may lose hope. However, this is not the case.13 Patients with a KIS, in particular those who had had a discussion about where they wanted to die, were less likely to die in hospital. This is important as most people prefer to die outside of hospital,14 and so any interventions which may facilitate this should be incorporated early into routine care.
GPs recognised the challenges in ensuring high-quality anticipatory care, as previously described.15 Our study, however, noted high levels of conversations around DNACPR/Preferred Place of Care (PPC)/Preferred Place of Final Care (PPFC) documented over a number of weeks, evidencing that GPs are taking time to discuss these issues. GPs face significant challenges in dealing with the increasing numbers of patients who would potentially benefit from anticipatory care and having these conversations sensitively and meaningfully takes time.16 Financial incentives only partly address this. National figures show that GPs are writing more KIS than they are resourced for.17 In order to ensure that patients can continue to be appropriately identified for and offered high-quality anticipatory care planning, these resource issues need to be considered. GPs were positive about KIS in the interface between themselves and GPs working OOH, as reported in a previous KIS evaluation.18
Limitations and generalisability
Enthusiastic KIS adopting practices might have been more likely to participate in this evaluation, but individual practices ranged from having 96% to 36% of patients on a KIS at death, displaying a much wider range of implementation than expected from practice demographic populations. GPs interviewed tended to be experienced and sometimes the practice lead in this clinical area. This was an in-depth evaluation from one Scottish Health Board. However, the KIS and the Palliative Care DES were implemented Scotland-wide and we consider that findings would be similar across the country as there was a wide nationwide uptake of both initiatives. Provisions for electronic shared care records, although 100% in Scotland, vary widely across the rest of the UK, but large projects are going ahead in England.19 We highlight the importance of having electronic, real-time, easily shareable records and the potential benefits they can have. The SPARRA tool has been developed over a number of years, and has widespread use in Scotland, but has not been formally validated.
Implications for service development, teaching, training and research
Conversations about anticipatory and palliative care are sensitive and take time to do well, as also previously described.20 ,21 Time and resources required to address this should be invested, especially given the increasing evidence that planning ahead with patients and carers can reduce hospital admissions and deaths in hospital. Hospital admissions are costly to the NHS, can precipitate a decline in older patients22 and many patients would prefer to avoid admission and die at home. Training in when and how to have anticipatory conversations is needed to improve utilisation, especially when there is so much variation in the number of patients started on KIS by different practices. Research focused on training interventions to improve patient identification and anticipatory care planning is recommended.23
Patients with multimorbidities, in this study noted to be 85% at death, particularly need coordinated care, such as anticipatory care. The KIS has a large part to play in the care of this patient group. Anticipatory care planning is ‘everyone's role’ and better mechanisms could exist to allow ‘real-time’ sharing of anticipatory care planning conversations by developments such as the KIS. Routine access of KIS, for patients who have one, should be seen as a compulsory part of care in all settings to help ensure that patient preferences are taken into account and to prevent repeated difficult conversations in multiple settings.
This initiative in Scotland to introduce anticipatory care early in the course of all progressive illnesses has proved to be successful. We evaluated a move away from waiting to identify patients specifically for ‘palliative care’ towards earlier identification of patients for ‘anticipatory care’ across all trajectories of physical decline. GPs found that planning with patients to anticipate likely events, which patients wanted to avoid, and seeking consent to share this information with other services involved with patient care were easier to do than having conversations about dying and possible needs for palliative care. Many people with non-malignant illnesses are sometimes more worried about getting dementia or a hospital or care home admission than actually dying, so dealing with their most pressing concerns enables a more person-centred approach than talking about dying.10 More work into how to integrate this type of approach early for a complex multimorbid population internationally is indicated. Further studies comparing ‘anticipatory care’ or ‘future care planning’ with ‘palliative care’ using the KIS and similar initiatives would be useful to guide how people and their carers can best be helped to get early appropriate care to optimise their last phase of life.
Conclusions
GPs have made considerable progress in identifying patients for an anticipatory care approach, earlier in the disease process, and more equitably across the different disease trajectories, than they were previously in identifying patients for palliative care. However, many still miss out from any care planning, particularly those dying with organ failure. Being identified for an anticipatory approach, in particular having a discussion around the preferred place of death, and communicating this with other medical providers is associated with allowing patients to die outside of hospital should they wish to do so, especially in the residential care setting.
Shared electronic records in the form of KIS are appreciated by GPs and are working well, greatly improving communication between GP and OOH care. Providing good anticipatory care should be seen as everyone's business. Secondary care must increase access and awareness of this development for patient benefit. More work is needed to support clinicians in secondary care and the wider MDT to become more actively involved with anticipatory care to ensure that this approach is maintained at all stages, in all settings, when caring for patients over the course of their illness.
References
Footnotes
Twitter Follow Charlie Hall at @chazhallNI
Contributors SAM and JT designed the study and recruited the practices. JT collected the data and did the initial analysis supported by JR (qualitative) and AL and AF (quantitative). All authors met as a steering group to bring multidisciplinary perspectives. All authors contributed to the initial draft of the paper and also in checking the final manuscript.
Funding A grant of £4,000 from NHS Lothian funded this study. The posts of CH, JS and AF were funded by Marie Curie. The researcher was in receipt of an academic fellowship from the Scottish School of Primary Care through the University of Edinburgh.
Competing interests None declared.
Ethics approval South East Scotland Ethics Service.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Further data may be available by contacting the corresponding author.