Article Text

Abstract
Objective: To investigate the outcome of patients with acute chest pain and normal troponin concentrations.
Design: Prospective cohort design.
Setting: Single centre study in a teaching hospital in Spain.
Patients: 609 consecutive patients with chest pain evaluated in the emergency department by clinical history (risk factors and a chest pain score according to pain characteristics), ECG, and early (< 24 hours) exercise testing for low risk patients with physical capacity (n = 283, 46%). All had normal troponin concentrations after serial determination.
Main outcome measures: Myocardial infarction or cardiac death during six months of follow up.
Results: 29 events were detected (4.8%). No patient with a negative early exercise test (n = 161) had events versus the 6.9% event rate in the remaining patients (p = 0.0001). Four independent predictors were found: chest pain score ⩾ 11 points (odds ratio (OR) 2.4, 95% confidence interval (CI) 1.1 to 5.5, p = 0.04), diabetes mellitus (OR 2.3, 95% CI 1.1 to 4.7, p = 0.03), previous coronary surgery (OR 3.1, 95% CI 1.3 to 7.6, p = 0.01), and ST segment depression (OR 2.8, 95% CI 1.3 to 6.3, p = 0.003). A risk score proved useful for patient stratification according to the presence of 0–1 (2.7% event rate), 2 (10.2%, p = 0.008), and 3–4 predictors (29.2%, p = 0.0001).
Conclusions: A negative troponin result does not assure a good prognosis for patients coming to the emergency room with chest pain. Early exercise testing and clinical data should be carefully evaluated for risk stratification.
- prognosis
- troponin
- unstable angina
Statistics from Altmetric.com
Since the introduction of troponin as a marker of necrosis, the diagnostic and prognostic accuracy of acute chest pain has improved significantly. Troponin has had such an impact that a consensus was needed for a new definition of acute myocardial infarction.1 Furthermore, in patients with troponin increases, not only must an acute myocardial infarction be diagnosed but also invasive management is advised.2,3 However, in acute chest pain without an increase in troponin the decision remains a challenge in terms of both diagnosis and prognosis.
Some data indicate that a negative troponin result confers a good prognosis given the low incidence of cardiac death or non-fatal myocardial infarction at 30 days in such cases (0.3% for negative troponin I and 1.1% for negative troponin T).4 Therefore, a policy of rapid discharge from the emergency room may be advocated. However, other studies found a non-negligible 3% rate of major events at 30 days.5,6 Furthermore, in the series of Kontos and colleagues7 the sensitivity of troponin for predicting significant coronary artery disease or significant complications in patients with acute chest pain was low. In this sense, though the absence of troponin increase would identify a lower risk, this does not necessarily imply a low risk group.
The present study examined a series of patients coming to the emergency department with acute chest pain in the absence of ST segment elevation and with normal troponin concentrations. They were managed by a chest pain unit protocol, including early exercise testing, and were followed up for six months. The aim was to investigate the outcome of patients with chest pain and negative troponin results.
METHODS
Patient population
A total of 609 consecutive patients coming to the emergency room of our hospital (from 15 January 2001 to 1 June 2003) with acute chest pain of possible coronary origin and with normal troponin I concentrations were prospectively studied. All patients were evaluated by a chest pain unit protocol implemented in our institution and comprising the clinical history, ECG, serial troponin I determination, and early exercise testing in the low risk subgroup.8,9,10 The inclusion criterion was the clinical diagnosis of chest pain of possible coronary origin, established by the cardiologist on duty. ST segment elevation in the initial ECG, left bundle branch block, and heart failure (Killip class > I) were exclusion criteria. Patients admitted more than once during the study period were included only on first admission.
Chest pain unit protocol
Clinical history
The clinical characteristics of chest pain presentation were assessed. On the basis of these characteristics, the semiquantitative score previously reported by Geleijnse and colleagues11 was calculated (appendix 1). In addition, risk factors such as sex, age, smoking, arterial hypertension, diabetes mellitus, cholesterol, family history, previous ischaemic heart disease, and previous coronary surgery were recorded.
ECG
An ECG was recorded in the emergency room and evaluated for ST segment depression (> 1 mm) and T wave inversion (peak inversion > 1 mm).
Troponin I
Troponin I was determined in the emergency department on arrival and six (in patients arriving within the first two hours after pain onset), eight, and 12 hours after pain onset. Troponin I was determined immunologically with an Immulite assay (Diagnostic Products Corporation, Los Angeles, California, USA). According to the manufacturer’s instructions, the Immulite troponin I kit was used to test 255 serum samples from healthy laboratory volunteers and from hospitalised patients who had been shown to be negative for troponin I by another immunometric method. The median value for these samples was non-detectable; 98% of the values were below 1.0 μg/l. Troponin I increase was defined as ⩾ 1 μg/l (upper limit of normality). The troponin I assay was tested in our laboratory, the coefficient of variation being < 10%. Coefficients of variation were obtained at two levels: one within the normal range and the other above the normal range.
All patients had normal troponin concentrations at all determinations.
Early exercise testing
After the clinical history and ECG were evaluated, 326 patients (54%) were directly hospitalised and 283 (46%) were considered to be eligible for early exercise testing (within the first 24 hours after their arrival). The decision to order an early exercise test was left to the discretion of the attending physician once the normality of troponin values 12 hours after chest pain onset was known. Eligible patients were considered to be at low risk according to the clinical history, with no ECG evidence of ischaemia or confounding repolarisation changes, and the existence of physical capacity for exercise. A symptom limited Bruce protocol was used. The result was considered positive in the case of angina or ischaemia induction (indicated by a 1 mm horizontal or downsloping depression of the ST segment at 80 ms from the J point or by a 1 mm ST elevation). The test was considered inconclusive if the patient was unable to reach a submaximal heart rate (85% of the theoretical age predicted heart rate) or developed non-specific ST-T segment changes during or after exercise. A negative test was reported in the case of at least one submaximal test without angina or ischaemia. All 161 patients with a negative result were discharged after the exercise test and all 60 patients with a positive test were hospitalised. In the case of an inconclusive test, the final decision was left to the supervising physician.
In-hospital management
All admitted patients were treated with aspirin, low molecular weight heparin, and β blockers (unless contraindicated). A total of 236 patients (39%) underwent cardiac catheterisation. During hospitalisation 101 patients (17%) underwent a revascularisation procedure: 67 had percutaneous coronary intervention and 34 had coronary surgery. Creatine kinase MB mass (5 μg/l upper limit of normal) was routinely determined 12 and 24 hours after a revascularisation procedure.
Fifty seven patients had normal coronary arteries (24% of the invasive studies). Thirty two of them had been directly hospitalised, whereas 25 had performed an early exercise test before hospitalisation (16 with a positive result and nine with an inconclusive result). Thirty seven men (21% of the catheterised men) and 20 women (33% of the catheterised women) had a normal angiogram.
End points
Patients were followed up for six months. The following events were regarded as end points: acute myocardial infarction, in the case of a new episode of chest pain with increased troponin I; and a major event defined as acute myocardial infarction or cardiac death. Information on the end point was collected in the outpatient department or by telephone. Sudden death was regarded as cardiac death. Two patients died of non-cardiac causes (respiratory failure and cancer) and their follow up period was defined as the time elapsed up to that point. Acute myocardial infarction was also considered if creatine kinase MB increased to ⩾ 3 times the upper limit of normal after coronary angioplasty or to ⩾ 5 times the upper limit of normal after coronary bypass surgery.12
Statistical analysis
To analyse the predictors for the end points, clinical factors such as chest pain score and risk factors (age, sex, smoking, arterial hypertension, diabetes mellitus, cholesterol, family history, previous ischaemic heart disease, and previous coronary surgery), and ECG data (ST segment depression, T wave inversion) were taken as independent variables. Categorical variables were expressed as percentages and were compared by the χ2 test. Multivariate analysis by Cox regression tested variables that were significant at p < 0.1 in the univariate analysis. The odds ratios (ORs) and their 95% confidence intervals (CIs) were calculated. Finally, survival curves according to the Kaplan-Meier method were determined with the use of the log rank test for the analysis of trend. A p ⩽ 0.05 was considered to be significant.
RESULTS
Patient population characteristics
Table 1 shows the clinical and ECG characteristics of the global patient population. Patients allocated to early exercise testing presented with less typical chest pain (mean (SD) chest pain score 9.2 (2.2) v 11.7 (2.7) points, p = 0.0001), were younger (61 (11) v 67 (11) years, p = 0.0001), had lower rates of hypertension (52% v 67%, p = 0.0001) and previous ischaemic heart disease (27% v 59%, p = 0.0001), and had a higher rate of current smoker status (24% v 17%, p = 0.03). There were no differences in the proportion of men (67% v 66%, p = 0.8) or of hypercholesterolaemia (51% v 56%, p = 0.2), diabetes (24% v 26%, p = 0.5), family history (15% v 11%, p = 0.1), or previous coronary surgery (5% v 7%, p = 0.3).
During follow up, 25 patients (4.1%) had an acute myocardial infarction, nine (1.5%) died of cardiac causes, and 29 (4.8%) had a major event. Six myocardial infarctions and two deaths (one caused by retroperitoneal haematoma after percutaneous intervention and the other after bypass surgery) were related to the revascularisation procedures.
Prognostic stratification according to early exercise testing
One hundred and eighty five patients were discharged immediately after early exercise testing (161 with a negative test and 24 with an inconclusive test). No patient with an early negative test had major events and one patient discharged after an inconclusive test had a non-ST elevation acute myocardial infarction during follow up. Among hospitalised patients one died and two had infarctions (all events in test positive patients) after exercise testing.
Given the good prognosis of a negative result in the early exercise test, the global patient population was divided into two groups according to their capacity to perform a negative early exercise test. Patients without a negative early exercise test, owing either to a contraindication to exercise or to a non-negative result, had a 6.0% rate of myocardial infarction (p = 0.001) and a 6.9% rate of major events (p = 0.0001) compared with the 0% event rate in the subgroup of patients with a negative early exercise test.
Predictors of acute myocardial infarction
Table 2 lists the predictors of acute myocardial infarction during the follow up by univariate and multivariate analyses. The independent factors that increased the risk of an acute myocardial infarction were a higher chest pain score (per point, OR 1.2, 95% CI 1.1 to 1.4, p = 0.009), older age (per year, OR 1.04, 95% CI 1.01 to 1.09, p = 0.04), male sex (OR 3.7, 95% CI 1.2 to 11.1, p = 0.02), diabetes mellitus (OR 2.5, 95% CI 1.1 to 5.7, p = 0.02), and ST segment depression (OR 2.9, 95% CI 1.2 to 6.8, p = 0.02).
Predictors of major events
Table 3 presents the predictors of major events. By multivariate analysis, a higher chest pain score (OR 1.2, 95% CI 1.1 to 1.4, p = 0.01), diabetes mellitus (OR 2.3, 95% CI 1.1 to 4.7, p = 0.03), previous coronary surgery (OR 3.1, 95% CI 1.3 to 7.6, p = 0.01), and ST segment depression (OR 2.8, 95% CI 1.3 to 6.3, p = 0.003) were related to major events. As there were revascularisation related adverse events, the multivariate analysis was repeated after censoring of patients at the time of revascularisation; in this second analysis, chest pain score (p = 0.01), ST segment depression (p = 0.003), and diabetes mellitus (p = 0.05) persisted as independent predictors of major events.
Risk stratification
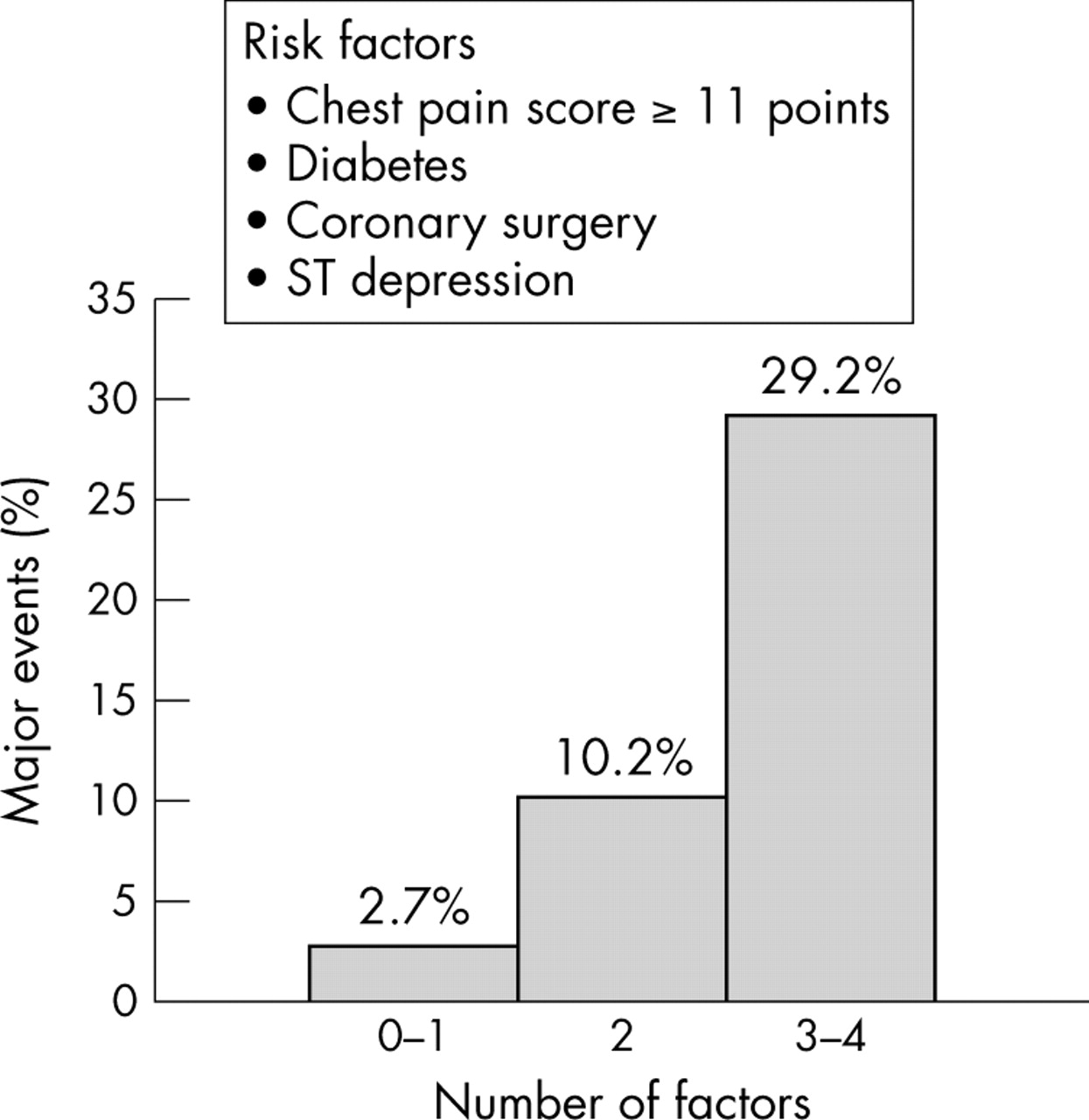
The patient population was stratified according to the four independent factors associated with major events in the multivariate analysis: chest pain score, diabetes mellitus, previous coronary surgery, and ST segment depression. The continuous variable chest pain score was transformed into a categorical variable by the receiver operating characteristic test to define the best cut off value (score ⩾ 11 points); this categorical variable persisted as an independent predictor in the multivariate model (OR 2.4, 95% CI 1.1 to 5.5, p = 0.04). Four subgroups were considered according to the presence of no (n = 201), one (n = 240), two (n = 98), or three or four factors (n = 24). The event rate increased progressively with the number of the risk factors: no factors, 2.5% event rate; one factor, 2.9%; two factors, 10.2%; and three or four factors, 29.2%. Three risk categories were defined (fig 1): low risk (no or one factors, 2.7% event rate), intermediate risk (two factors, 10.2%), and high risk (three or four factors, 29.2%). The differences were significant between the high risk subgroup and the intermediate (p = 0.001) and low risk (p = 0.0001) subgroups and between the intermediate and the low risk subgroups (p = 0.008). The survival curves shifted downwards progressively from the low risk to the high risk subgroups (log rank 40.5, p = 0.0001 for the trend) (fig 2).
DISCUSSION
Main findings
In the present study patients with acute chest pain and negative troponin concentrations had a non-negligible rate of major events of 4.8% after six months of follow up. Risk can be stratified based on simple data available at presentation. On the one hand, patients without contraindication to early exercise testing and who perform a negative test constitute a very low risk population. On the other hand, clinical data such as pain characteristics, diabetes, previous coronary surgery, and ST segment depression allowed risk stratification; the greater the number of these factors the higher the risk of major events.
Clinical history
Symptom evaluation in the emergency room is of utmost importance in patients with chest pain. One of the major problems with chest pain symptoms is that they are variable and perceived very differently by patients.13 In most patients presenting to the emergency room with chest pain, this symptom is related to non-cardiac disorders without fatal potential, such as musculoskeletal, gastro-oesophageal, or anxiety syndromes.14 Lee and colleagues15 defined some characteristics indicating very low risk: sharp or stabbing pain, no history of angina pectoris or myocardial infarction, pain with pleuritic or positional components, and pain that was reproduced by palpation of the chest wall. To assess the characteristics of chest pain, we have used a score previously published by Geleijnse and colleagues.11 This clinical score was found to be an independent predictor of worse outcome, indicating a greater probability of a cardiac origin of the pain.
Other data from the clinical history, such as diabetes and previous coronary surgery, proved to be important. In populations with different characteristics, such as patients admitted with the diagnosis of unstable angina or non-ST segment elevation acute myocardial infarction, the risk scores also incorporate the variable diabetes.16,17
ECG
About 50% of patients with unstable angina or non-Q wave myocardial infarction do not have significant changes on the ECG.18 The most important adverse ECG prognostic indicator is the presence of ST segment depression.18–25 Previous studies of non-ST segment elevation acute coronary syndromes have shown that quantitative assessment of the ECG is helpful in assessing the likelihood of events in patients with a negative troponin test presenting with ischaemic chest pain.26 We studied only patients with normal troponin concentrations, resulting in a 12% rate of ST segment depression, this being lower than the 24% or 27% rates observed in the global spectrum of patients with chest pain.9,19 ST segment depression was an independent predictor of poor outcome, although the low prevalence of ST depression in patients with normal troponin may limit its clinical value.
Role of early exercise testing
Previous studies have provided evidence of the safety and usefulness of early exercise testing in patients with chest pain considered to have low risk.27–33 The main contribution of the early exercise test in these patients is its high negative predictive value (⩾ 98%), which allows them to be safely discharged from the emergency department.34 In the present series, no patient with a negative exercise test had events during follow up, despite early discharge without hospitalisation.
Outcome of chest pain with normal troponin concentrations
Risk scores based on clinical data at presentation have been developed in non-ST segment elevation acute coronary syndromes in mixed populations of patients with chest pain with and without increased cardiac markers.9,16,17 However, the prognostic evaluation of the subset of patients with normal troponin remains a challenge. Hamm and colleagues4 suggested rapid and safe discharge based on the low rate of events at 30 days in such cases. However, more recent studies reported a 3% event rate, this being much lower than in patients with troponin increase but high enough to prevent this population from being defined as a low risk group.5,6 The present study detected a 4.8% event rate over six months of follow up in a population managed by a chest pain unit protocol that included early exercise testing. Simple clinical data available at presentation can be used to categorise patients from low to high risk depending on the number of risk variables, which are a typical presentation of pain (chest pain score), diabetes, previous coronary surgery, and ST segment depression. Therefore, the clinical data of these patients should be carefully evaluated.
Limitations
Firstly, the lack of systematic exercise testing, left to the decision of the attending physician, may limit the findings of the present study. Secondly, it would have been of interest to know whether the early exercise test provided incremental prognostic information additional to that provided by clinical risk scoring; however, the lack of statistical power because of the small sample size does not allow us to analyse the subgroup of patients allocated to early exercise testing, incorporating in the multivariable analysis exercise testing variables along with the clinical risk predictors. Thirdly, since the indication for revascularisation was not controlled and there were revascularisation related adverse events, decisions regarding revascularisation may bias the results.
Conclusions
A negative troponin result does not assure a good prognosis for patients coming to the emergency room with chest pain. The frequency of major events at six months is a non-negligible 4.8%. Early exercise testing and clinical data available in the emergency room are useful for risk stratification.
This work was supported by a grant from RECAVA-FIS.
Characteristics of the patient population (n = 609)
Predictors of acute myocardial infarction by univariate and multivariate analyses
Predictors of major events (acute myocardial infarction or cardiac death) by univariate and multivariate analyses
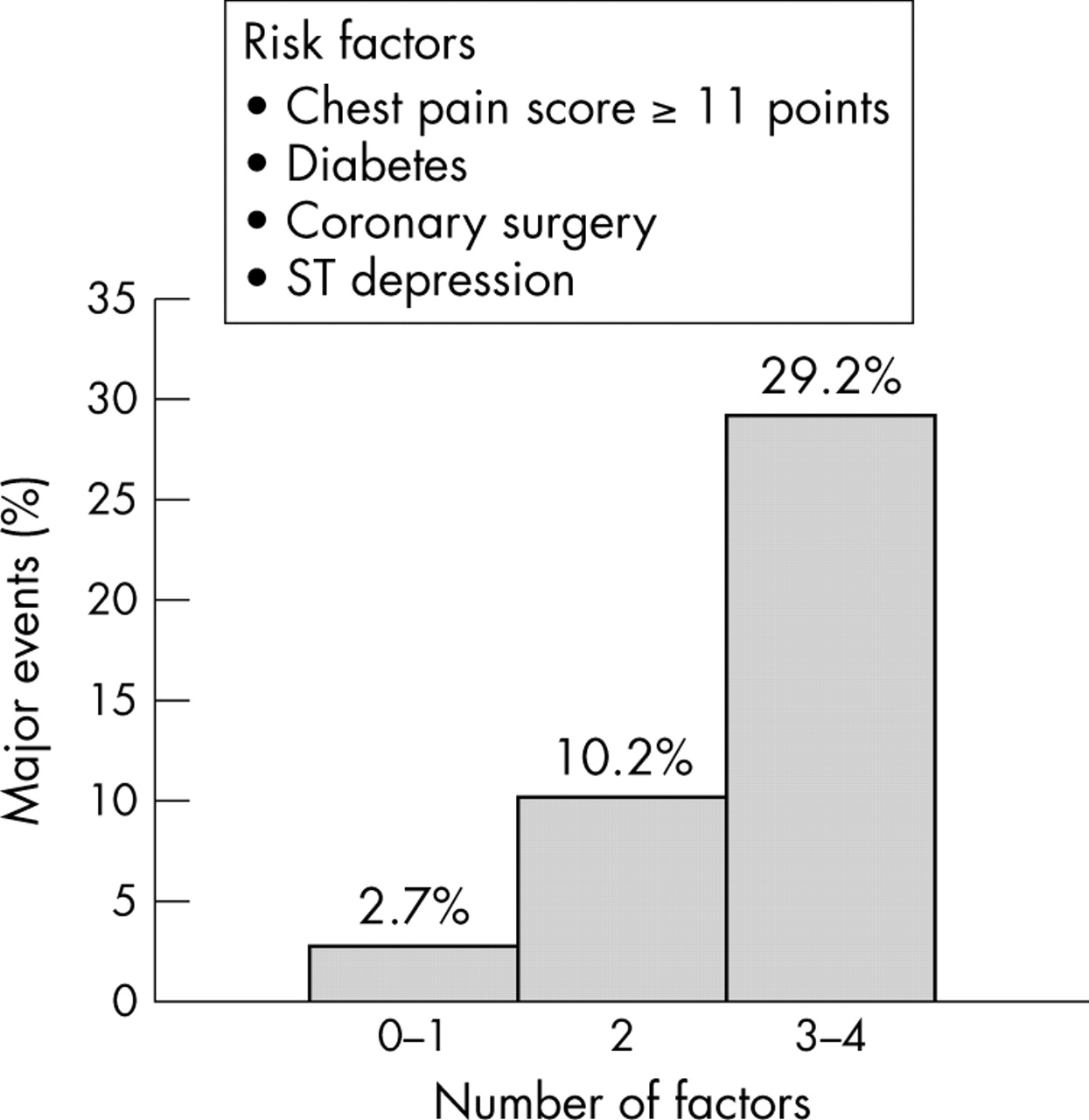
Even rate stratification by risk factors related to major events. The differences were significant between the high risk (3–4 risk factors) and the intermediate (2 factors, p = 0.001) and low risk (0–1 factors, p = 0.0001) subgroups and between the intermediate and low risk subgroups (p = 0.008).

{kind=link}
{kind=link}
Kaplan-Meyer curves showing the event rate during the six months of follow up in the three risk subgroups of patients. The survival curves shift downwards progressively from the low risk to the high risk subgroups (log rank 40.5, p = 0.0001 for the trend).