Article Text

Abstract
Background: The ability of β blockers to improve left ventricular function has been demonstrated, but data on the effects on cardiac remodelling are limited.
Objective: To investigate, using cardiovascular magnetic resonance (CMR), the effects of carvedilol on left ventricular remodelling in patients with chronic stable heart failure and left ventricular systolic dysfunction caused by coronary artery disease.
Design: Randomised, double blind, placebo controlled study.
Setting: Chronic stable heart failure.
Patients and intervention: 34 patients with chronic stable heart failure and left ventricular systolic function taking part in the CHRISTMAS trial (double blind carvedilol v placebo) underwent CMR before randomisation and after six months of treatment.
Main outcome measure: Left ventricular remodelling at six months.
Results: The carvedilol and placebo groups were well balanced at baseline, with no significant intergroup differences. Over the study period, there was a significant reduction in end systolic volume index (ESVI) and end diastolic volume index (EDVI) between the carvedilol and the placebo group (carvedilol −9 v placebo +3 ml/m2, p = 0.0004; carvedilol −8 v placebo 0 ml/m2, p = 0.05). The ejection fraction increased significantly between the groups (carvedilol +3% v placebo −2%, p = 0.003).
Conclusions: Treatment of chronic stable heart failure with carvedilol results in significant improvement in left ventricular volumes and function. These effects might contribute to the benefits of carvedilol on mortality and morbidity in patients with chronic heart failure.
- CHRISTMAS, carvedilol hibernation reversible ischaemia trial, marker of success
- CMR, cardiovascular magnetic resonance
- COI, cardiac output index
- COMET, carvedilol or metoprolol European trial
- EDVI, end diastolic volume index
- EF, ejection fraction
- ESVI, end systolic volume index
- LVEDV, left ventricular end diastolic volume
- LVESV, left ventricular end systolic volume
- LVMI, left ventricular mass index
- LVSVI, left ventricular stroke volume index
- β blockers
- remodelling
- heart failure
- magnetic resonance imaging
Statistics from Altmetric.com
- CHRISTMAS, carvedilol hibernation reversible ischaemia trial, marker of success
- CMR, cardiovascular magnetic resonance
- COI, cardiac output index
- COMET, carvedilol or metoprolol European trial
- EDVI, end diastolic volume index
- EF, ejection fraction
- ESVI, end systolic volume index
- LVEDV, left ventricular end diastolic volume
- LVESV, left ventricular end systolic volume
- LVMI, left ventricular mass index
- LVSVI, left ventricular stroke volume index
Recent years have seen a notable improvement in both morbidity and mortality in patients with chronic heart failure. Much of this benefit is derived from the use of therapeutic agents, including angiotensin converting enzyme (ACE) inhibitors and β blockers, which interfere with neurohormonal pathways that are activated by cardiac dysfunction. In placebo controlled trials, β blockers have consistently improved survival, reduced hospital admissions, and improved symptoms and quality of life.1–,5
Much of the benefit of β blockade in patients with heart failure secondary to left ventricular systolic dysfunction may result from their ability to improve left ventricular systolic function, which has been demonstrated in various studies using echocardiography or nuclear techniques.6–,8 Data on cardiac remodelling, however, are limited. Cardiovascular magnetic resonance (CMR) provides an accurate and reproducible measurement of left ventricular remodelling in small sample sizes, by assessment of volumes, ejection fraction, and mass.9,,10 We investigated the effects of carvedilol versus placebo on left ventricular volume, mass, and function using CMR as a measure of cardiac remodelling in patients with chronic stable chronic heart failure and left ventricular systolic dysfunction caused by coronary artery disease. This was a substudy of the CHRISTMAS trial (carvedilol hibernation reversible ischaemia trial; marker of success).11,,12
METHODS
Patients
Thirty four consecutive patients recruited for the CHRISTMAS trial from two participating centres were included in the CMR substudy. Patients were recruited between 1995 and 1999, and the study began before publication of the major β blocker outcome trials in chronic heart failure. The inclusion and exclusion criteria for the CHRISTMAS trial were as follows:
-
chronic stable heart failure (New York Heart Association functional class I–III) from systolic dysfunction caused by coronary artery disease
-
already receiving optimised chronic heart failure treatment (including diuretics and an ACE inhibitor if tolerated)
-
echocardiographic imaging of sufficient quality for wall motion analysis.
Patients with atrial fibrillation or severe valvar disease were excluded, and additional exclusion criteria for the CMR substudy were the presence of an implanted pacemaker and claustrophobia.
Study design
Patients underwent the first CMR scan after inclusion in the CHRISTMAS trial, but before randomisation to carvedilol or placebo. The follow up scan was done six months after randomisation, while patients were still on double blind treatment. Height, weight, and blood pressure were recorded before scanning, the latter done after 20 minutes of rest in a sitting position. During each study, heart rate was recorded continuously and the average heart rate during the scanning sequence noted.
The CMR substudy was approved by the ethics committees of both participating centres, and written consent was obtained.
CMR measurement of remodelling
CMR was done with a Picker Edge 1.5 T scanner (Marconi, Cleveland, Ohio, USA), using the body coil and ECG triggering, as previously described.13 In brief, the cardiac short axis was determined from three scout images of the left ventricle—the transverse axis, the vertical long axis, and the breath hold diastolic horizontal long axis. The basal short axis slice was positioned just forward of the atrioventricular ring, and all subsequent breath hold cines were acquired in 1 cm steps towards the apex. A breath hold, segmented gradient echo, fast low angle shot (FLASH) sequence was used for each of the contiguous short axis slices. Parameters were as follows: echo time (TE), 3.8 ms; repeat time (TR) = RR interval; slice thickness, 10 mm; field of view, 35 × 35 cm; read matrix, 256; phase matrix, 128; frames, 16; flip angle, 35°; phase encode group, 6–10. An average of 10 short axis segments was needed to encompass the entire left ventricle.
Image analysis was carried out on a personal computer using software developed in-house (CMRtools, Cardiovascular Imaging Solutions, London, UK). End diastolic and end systolic images were chosen as the maximum and minimum cross sectional areas in each cine. Short axis end diastolic epicardial and endocardial borders were traced manually for each slice. From the area within the contours and the slice thickness, the epicardial volume and endocardial volume (left ventricular end diastolic volume, LVEDV) were calculated, the difference representing myocardial volume. Left ventricular mass (LVM) was derived from this volume by multiplying by the specific density of the myocardium (1.05 g/cm3).14 End systolic endocardial borders were also traced, to give left ventricular end systolic volume (LVESV). The difference between LVEDV and LVESV represents the left ventricular stroke volume (SV). Ejection fraction (EF (%)) was calculated as (LVEDV – LVESV)/LVEDV × 100. Papillary muscles were included in the mass and excluded from the volume. All analyses were done off-line in random order, with investigators blinded to the patient details and previous results.
Statistical analysis
To control for changes in body mass index over the study period, EDV, ESV, SV, cardiac output (CO), and LVM were expressed as an index of total body surface area—EDVI, ESVI, LVSVI, COI, and LVMI—by dividing each variable by the patient’s body surface area.15 Unpaired t tests between the carvedilol and placebo groups were employed at baseline to detect any initial differences. Differences within the carvedilol and placebo groups over the study period were assessed using a paired t test. Differences between the carvedilol and placebo groups over time were examined using an unpaired t test on the intragroup differences. Results are expressed as mean (SD), with a probability value of p < 0.05 being considered significant. Statistical analyses were done with commercial software (StatView version 4.53; Abacus Concepts Inc, Berkeley, California, USA). The reproducibility of CMR in our centre has been published previously and the interstudy percentage variability is 2.5% for EDV, 3.1% for ESV, 4.8% for EF, and 3% for LVM.9 The minimum detectable differences in EDV, ESV, EF, and LVM by CMR for the 16 subjects in the carvedilol group were therefore 2.8 ml, 3.6 ml, 6% (absolute change), and 3.5 g, respectively; for the 13 subjects in the placebo group, the values were 3.2 ml, 4 ml, 6% (absolute change), and 3.8 g.
RESULTS
Thirty four patients were recruited into the CMR study and underwent a baseline scan. Of these, five did not complete the study. One patient was withdrawn from the substudy following a possible drug interaction, one because of worsening heart failure, one because of sleep apnoea, and two because of claustrophobia. These patients were therefore excluded from the analysis. All but one of the patients recruited were male. Their mean (SD) age was 71 (8.5) years. Mean EDVI was 135 (44) ml/m2 (normal 66 (12) ml/m2); mean ESVI, 95 (42) ml/m2 (normal 21 (8) g/m2); mean EF, 31 (11)%; and mean LVMI, 83 (24) g/m2 (normal 87 (24) g/m2) (normal values are from Lorenz and colleagues 16). Mean body surface area was 1.84 m2. The groups were well balanced at baseline, with no significant differences between them (table 1⇓). The mean dose of carvedilol achieved in the CMR study patients was 32 (15) mg.
Comparison of ventricular remodelling and haemodynamic variables at baseline and at the end of the study between the carvedilol and placebo groups
Change over time within each group
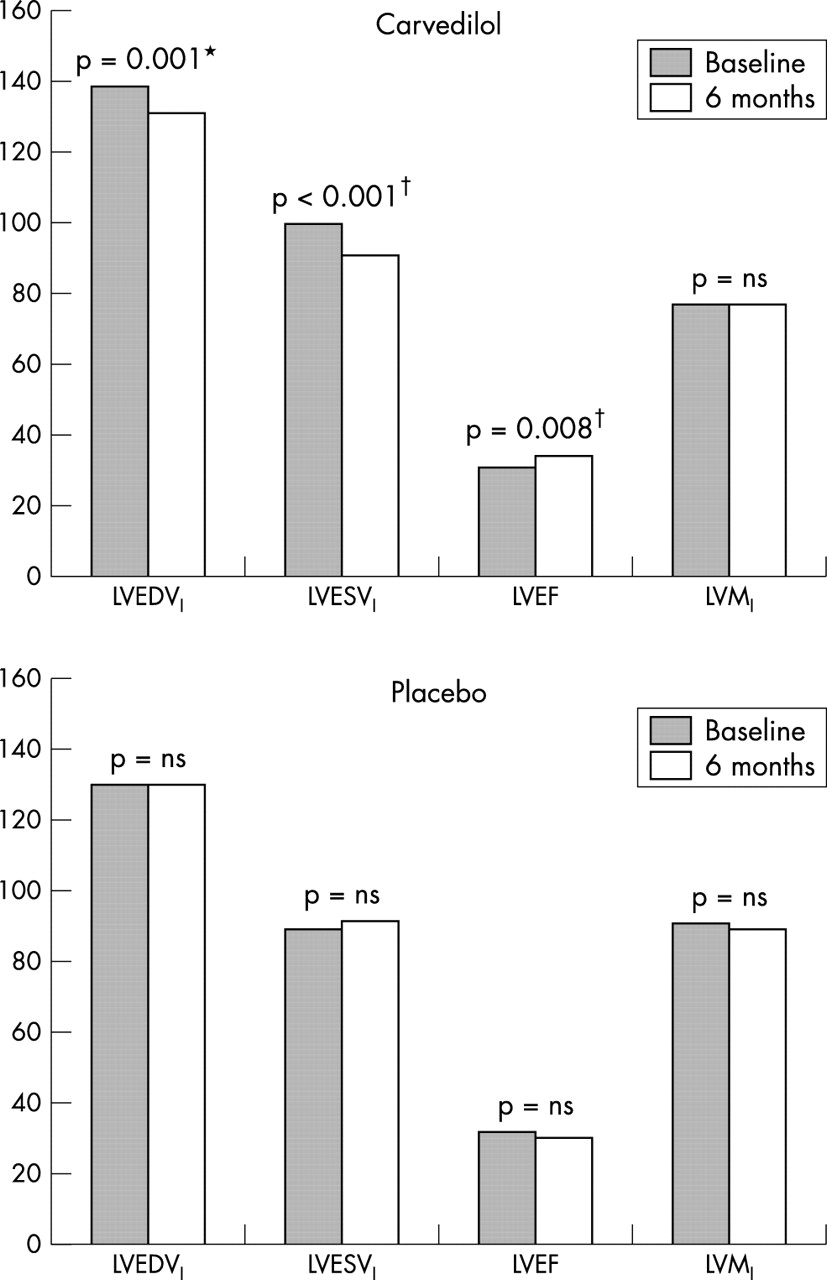
In the carvedilol group, the mean EDVI decreased from 139 to 131 ml/m2 (p = 0.001), representing a 5% decrease over the study period. The ESVI decreased by 9% (from 100 to 91 ml/m2, p = 0.0004), while ejection fraction increased by 9% (from 31% to 34%, 3% absolute, p = 0.008). There was no change in LVSVI, COI, LVMI, or blood pressure. Within the placebo group there were no significant changes in any of the remodelling indices over time. The changes are summarised in fig 1⇓.

{kind=link}
Change in variables over six months. LVEDVI, left ventricular end diastolic volume index; LVESVI, left ventricular end systolic volume index; LVEF, left ventricular ejection fraction; LVMI, left ventricular mass index. *p < 0.05, †p < 0.01 for the comparison of the change in variable over time between carvedilol and placebo groups.
Differences between groups over time
Over the study period, the carvedilol group showed a reduction in ESVI (carvedilol −9 ml/m2v placebo +3, p = 0.0004). There was also a significant difference in EDVI (carvedilol −8 ml/m2v placebo 0, p = 0.05) and ejection fraction (carvedilol +3% v placebo −2%, p = 0.003). None of the other variables differed significantly.
DISCUSSION
The main finding of this study is that over six months’ treatment of chronic stable heart failure, carvedilol resulted in a significant decrease in left ventricular volumes at both end systole and end diastole and thereby a reversal of adverse left ventricular remodelling. In addition, the left ventricular ejection fraction improved significantly with carvedilol. Left ventricular volumes and LVEF are strong predictors of all cause mortality and sudden death,17–,19 and a causal relation is suspected. Despite a reduction in volumes and arterial pressure, which should have reduced left ventricular wall stress, no reduction in left ventricular mass was observed.
An improved mass/volume ratio, leading to a reduction in left ventricular wall stress, could be of benefit either by reducing the metabolic demands on the left ventricle or by reducing the potential for arrhythmias. The sample size used here precludes stratification by dose, but a larger sample and a longer period of follow up could give additional insights into the effect of increasing doses of carvedilol and the duration of treatment on left ventricular remodelling.
Many studies have shown improvement in left ventricular function with β blockers (table 2⇓), but the mechanism remains poorly understood. The degree of functional improvement exerted by different agents, as illustrated by a meta-analysis of trials of carvedilol and metoprolol, has led to the suggestion that pharmacological effects other than pure β1 blockade are responsible.20 Indeed, carvedilol significantly reduced mortality compared with metoprolol in the recent COMET study.21 Investigators have, however, cautioned that this may simply reflect a lack of equivalence in the β1 blockers used rather than any additional pharmacological benefits. The exact mechanism of functional improvement has yet to be determined.21
Randomised trials of the effect of β blocker treatment on ejection fraction
Despite the wealth of studies on the effect of β blockers on left ventricular function, there have been few previous studies of the effect on left ventricular remodelling. Sharpe and colleagues found a significant reduction in EDV and ESV with carvedilol treatment over 12 months using cross sectional echocardiography in a 123 patient substudy of the Australia/New Zealand heart failure research collaborative group study.7,,36 These patients had heart failure of ischaemic origin and were already on an ACE inhibitor. Khattar and colleagues showed a reduction in ESV, but no change in EDV by cross sectional echocardiography with carvedilol monotherapy, and did not find any benefit in ESV when an ACE inhibitor was added to the carvedilol group.37 There was, however, a significant reduction in ESV when carvedilol was added in patients who had received six months of ACE inhibitor treatment alone. Groenning and colleagues published a randomised CMR study showing that metoprolol had reverse remodelling effects in 41 patients with chronic heart failure, with a significant reduction in EDVI and ESVI over six months of treatment.38 More recently, Dubach and associates used CMR to investigate a placebo controlled trial of bisoprolol in heart failure, but found only a non-significant trend for EDV and ESV reduction over 12 months.39 Carvedilol differs from conventional β1 selective compounds such as metoprolol and bisoprolol in that at therapeutic doses it blocks all three adrenergic receptors (β1, β2, and α1), resulting in a more comprehensive adrenergic protection of the failing heart.40 Furthermore, it reduces cardiac adrenergic activity41 and prevents the β1 receptor upregulation which is typically seen with β1 selective agents such as metoprolol.42 Because of its α1 blocking properties, carvedilol causes moderate peripheral vasodilatation which results in less myocardial depression, no reduction in cardiac output, and no initial haemodynamic compromise (which is normally observed with pure β blockers).43,,44 Thus it may be tolerated better than other agents.
Conclusions
Treatment of chronic stable heart failure with carvedilol results in significant improvement in left ventricular volumes and thereby in reversal of adverse left ventricular remodelling. This may partially explain the benefits of carvedilol on mortality and morbidity in patients with chronic heart failure.