Article Text

Abstract
Objective: To estimate the need for coronary revascularisation, by using an incidence of indications approach, among 45–84 year olds with stable angina, unstable angina, and acute myocardial infarction.
Design: Modelling exercise. Six key steps along the pathway of care from initial diagnosis in primary or secondary care to revascularisation were defined and the frequency of indications estimated using routine data from hospital admissions and data from studies in the general population, and primary and secondary care.
Setting and patients: Mid-1998 population of England.
Intervention: Coronary revascularisation.
Main outcome measure: Ability to benefit (need), defined by randomised trials, expert panel ratings from the ACRE (appropriateness of coronary revascularisation) study, or by informal consensus.
Results: The need for coronary revascularisation was estimated to be 92 000 procedures, equivalent to a rate of 1861 per million population. Overall, the model of need exceeded current provision by 3.3:1, although among people aged 75 years and over the ratio was 7.7:1. A plausible upper estimate of need—obtained by assuming that 90% of patients with stable angina were referred from primary care and that angiography would be performed in 65% of patients with acute myocardial infarction and 75% of patients with unstable angina—was 2626 per million population.
Conclusions: The national target of 1500 revascularisation procedures per million population is credibly related to population need, although upper estimates of need are considerably higher. Better understanding is required of the benefits of referring patients with specific indications from primary care. The greatest relative increase in provision is required for those aged 75 and older, among whom trial evidence of benefit is scant.
- needs assessment
- models, theoretical
- coronary revascularisation
- coronary disease
- ACRE, appropriateness of coronary revascularisation
- ENACT, European Network for Acute Coronary Treatment
- HES, hospital episodes statistics
- ICD-10, International classification of diseases, 10th revision
- MSGP4, 4th national morbidity survey in general practice
- OXMIS, Oxford myocardial infarction incidence study
- TACTICS-TIMI 18, treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy-thrombolysis in myocardial infarction 18
Statistics from Altmetric.com
- ACRE, appropriateness of coronary revascularisation
- ENACT, European Network for Acute Coronary Treatment
- HES, hospital episodes statistics
- ICD-10, International classification of diseases, 10th revision
- MSGP4, 4th national morbidity survey in general practice
- OXMIS, Oxford myocardial infarction incidence study
- TACTICS-TIMI 18, treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy-thrombolysis in myocardial infarction 18
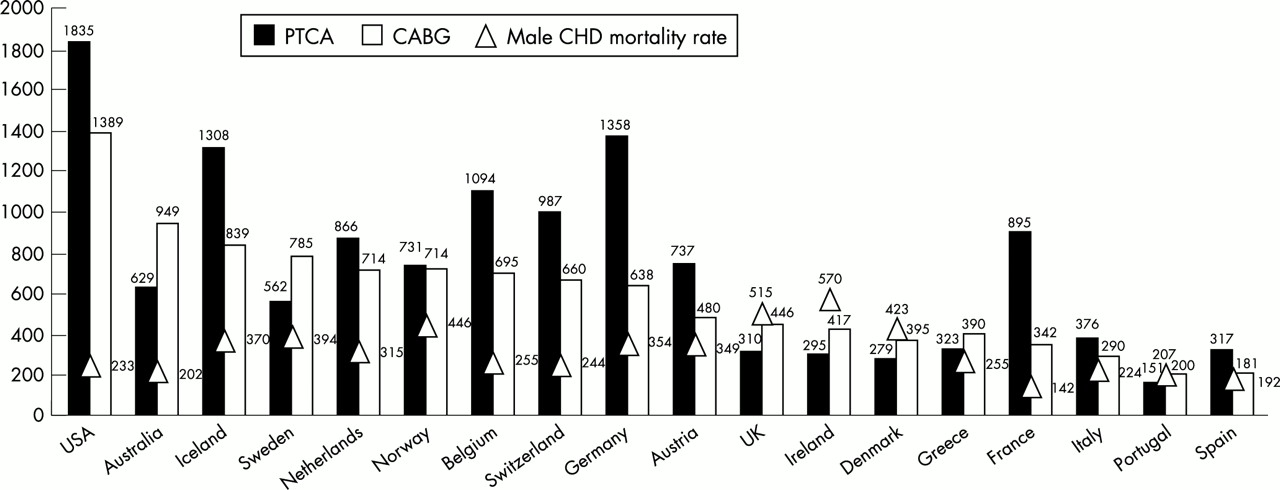
There are large international differences in coronary revascularisation rates (fig 1⇓),1–,3 with those in the USA (3224 per million population) nearly four times those in England (839 per million population) (fig 1⇓ and table 1⇓).4,5 Although these variations may in part be explained by the supply of facilities and doctors, the prevailing clinical culture towards invasive management, and differing public expectations, it is widely perceived that revascularisation is underprovided in England relative to need. As a consequence the government has set a national target of 1500 revascularisations per million population.6
Rates (per million population) of coronary revascularisation in England compared with the USA
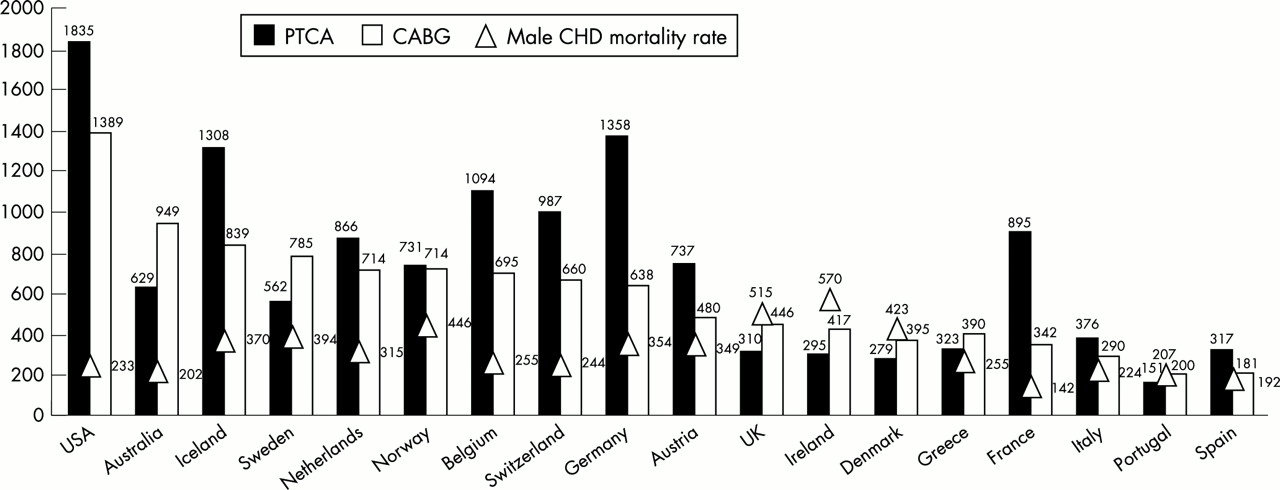
Coronary revascularisation rates per million inhabitants in the USA,2 Australia,3 and Europe1 and age adjusted mortality from coronary heart disease (CHD) in men. European coronary heart disease mortality data are for men aged 45–74 years per 100 000, 1990–2; US and Australian data are for men aged 35–74 years per 100 000 in 1995.4,5 CABG, coronary artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty.
It is unclear to what extent existing revascularisation rates, or their planned increase, reflect measured population need (ability to benefit),7,8 as the evidence and assumptions underpinning the current target have not been made explicit. Attempts have been made to model regional revascularisation requirements using standardised mortality ratios for coronary heart disease9 or coronary heart disease incidence,10 which are crude markers of need. A more sophisticated approach attempts to measure the population frequency of the indications for which revascularisation confers benefit.11 An indication is defined by the type of morbidity, its severity, and the degree of test abnormality. Such an “incidence of indications” approach has been applied in other conditions (for example, the need for total hip replacement12) and offers the advantage of explicitly linking epidemiological estimates of the population prevalence and incidence of specific clinical presentations with the evidence of effectiveness from randomised trials. However, there has been no previous attempt to model the need for revascularisation based on an incidence of indications approach.
The aim was to model coronary revascularisation need compared with current provision among patients with stable angina, unstable angina, and acute myocardial infarction. We further sought to test whether underprovision was greater at older ages.
METHODS
We developed two models of the incidence of indications for coronary revascularisation. Firstly, we used data on current patterns of referral, investigation, and treatment of 45–84 year olds in England to estimate current provision. Secondly, we modelled population need for revascularisation based on consensus guidelines, trial evidence of benefit, and ratings of appropriateness.
In a recent prospective study,13 chronic stable angina, unstable angina, and myocardial infarction accounted for 71% of the original clinical presentations, before angiography, of patients who subsequently underwent coronary revascularisation. The original clinical presentations before angiography of the remaining 29% undergoing revascularisation were recurrent angina after revascularisation, atypical chest pain, near sudden death, ventricular arrhythmia, asymptomatic, and miscellaneous or other presentations. For each of the presentations chronic stable angina, unstable angina, and myocardial infarction we defined six parameters likely to have a major impact on revascularisation rates:
Parameter 1: proportion of the population developing a new clinical presentation each year
Parameter 2: percentage of these referred to secondary care
Parameter 3: percentage of these surviving to be considered for angiography
Parameter 4: percentage of these undergoing (current practice) or deemed appropriate for (model of need) angiography
Parameter 5: percentage of these with obstructive coronary disease
Parameter 6: percentage of these undergoing (current practice) or deemed appropriate for (model of need) revascularisation.
We estimated these parameters from published and unpublished sources, stratifying by age group (45–64, 65–74, and 75–84 years) and sex, where possible. Since trial data are lacking for many patients—for example, older people—we incorporated expert panel judgements of revascularisation appropriateness, which have been validated against clinical outcomes.14
We conducted sensitivity analyses to identify the parameter with the largest influence on predicted need, within each clinical presentation, by modelling plausible increases in individual parameters one at a time while holding constant the other parameters in the model of need.
Chronic stable angina
Parameter 1—Estimates of stable angina incidence vary widely15–,17 (table 2⇓). We used the MSGP4 (4th national morbidity survey), 1991–92 (age and sex standardised rate across age groups: 13.5 per thousand).15 A proportion of incident indications for revascularisation also result from worsening symptoms among prevalent cases of angina,18 for which no reliable data exist. Among medically treated patients with angina in angioplasty trials, approximately 10% experience sufficient worsening of symptoms to require revascularisation over a year.19 Extrapolating from these data and allowing for our interest in referrals rather than revascularisations, we added 15% of the prevalent cases to the number of incident cases.
Range of estimates of incidence of chronic stable angina for parts of the UK
Parameter 2—In the model of current practice, general practice referral rates were obtained from the General Practice Research Database,20 1998 (age and sex standardised rate across age groups: 2.2 per thousand). A proportion of new outpatient referrals arise from sources other than general practice. On the basis of the observed case mix in one general medical outpatient clinic10 we applied a multiplying factor of 2.4 to the general practitioner referral rate to account for this. The model of need assumed, in keeping with the National Service Framework,6 higher rates of referral from primary care: 80% of 45–64 year olds,21 70% of 65–74 year olds, and 60% of 75+ year olds. The age gradient was chosen to account for limited trial evidence of benefit in older populations, the increased risks associated with coronary revascularisation in older age groups,22 and increased comorbidity with age.23,24 As a sensitivity analysis, the referral rate was increased to 90% in all age groups.21
Parameter 3—The mortality while waiting for referral was assumed to be 2% for the current practice model25 and 0% for the model of need.
Parameter 4—The model of current practice assumed that the proportion of referrals undergoing angiography was 30%.16,26 On the basis of data from a rapid access chest pain clinic in Bromley for 1999, our model of need assumed that 51% of referrals subsequently undergo angiography (Wood D, personal communication).
Parameter 5—In both models, the age and sex specific prevalence of angiographically defined obstructive coronary disease (single vessel, double vessel, and triple vessel or left main stem disease) was obtained from a prospective study in London for 1996/7 (the ACRE (appropriateness of coronary revascularisation) study).14
Parameter 6—In the model of current practice, age and sex specific proportions of subjects with specific coronary artery disease patterns undergoing revascularisation were estimated from the ACRE study.14 The model of need was based on age and sex specific proportions of subjects with specific coronary artery disease patterns in whom revascularisation was deemed appropriate.14 The ACRE study rated the appropriateness for revascularisation, scored by an expert panel, based on clinical and angiographic findings, and applied these ratings to a population of 2552 patients with coronary artery disease referred for angiography. Nearly all patients were assigned a rating. Patients in whom revascularisation was rated appropriate, and subsequently received it, had better clinical outcomes than those who were similarly rated but who received only medical treatment, providing evidence of the clinical validity of the expert panel ratings.14
Myocardial infarction
Parameter 1—The predicted incidence of fatal and non-fatal myocardial infarction was based on the OXMIS (Oxford myocardial infarction incidence study).27 These data highlight the burden of myocardial infarction in the community, although the computation of the model predictions began with parameter 2.
Parameters 2 and 3—We used national hospital episodes statistics (HES) data (1998–99) to compute incident age and sex specific emergency hospital admission rates for acute myocardial infarction (International classification of diseases, 10th revision (ICD-10) code I121) (age and sex standardised rate across age groups: 3.12 per thousand population) and inpatient death rates following admission for acute myocardial infarction (15.5%). (The low referral rate compared with the incidence rate reflects prehospital mortality.)
Parameter 4—In the model of current practice, angiography rates within six months of acute myocardial infarction (8%) were taken from data on routine clinical practice in the UK for 1993–94.28 This rate was very similar to a more recent estimate of 9% in UK settings in 1997–98 but that was based on the follow up of a randomised controlled trial of different fibrinolytics.29 In the model of need, we estimated appropriate rates of angiography from a systematic review, which found that angiography rates > 30% were not associated with reduced rates of death or reinfarction compared with conservative management.30 In the sensitivity analysis we assumed that 65% of patients with acute myocardial infarction undergo angiography, reflecting US practice.31
Parameters 5 and 6—These parameters were based on the ACRE study in both models.14
Unstable angina
Parameter 1—We found no population based data for the UK on the incidence of unstable angina. This parameter was therefore extrapolated from parameter 2 and we assumed a 100% referral rate to hospital.
Parameter 2—We computed age and sex specific emergency hospital admission rates for angina and unstable angina (ICD-10 code I120 in the main diagnosis field) from the HES database (1998–99); 99% of diagnoses were unstable angina (52%) or angina unspecified (47%).
Parameter 3—In hospital death rates were derived from a study of coronary care units in London.32
Parameter 4—In the model of current practice, the angiography rate was 27%, based on national referral patterns in the UK for 1998–99.33 In the model of need, we based predicted angiography rates on the TACTICS-TIMI 18 (treat angina with Aggrastat and determine cost of therapy with an invasive or conservative strategy-thrombolysis in myocardial infarction 18) trial,34 in which the 50% of patients at higher risk benefitted from invasive management.
Parameters 5 and 6—The ACRE study was used to derive age and sex specific estimates of angiographically defined obstructive coronary disease and proportions appropriate for revascularisation.14 In a sensitivity analysis, angiography rates were increased to 75%, reflecting the additional proportion of people in the TACTICS-TIMI 18 trial with an intermediate risk score in whom there was inconclusive evidence of benefit.
Coronary revascularisation in England: current provision
Current rates were computed for the resident population of England aged 45–84 years from the 1998–99 HES database using Office of Population Census and Surveys-4 procedure codes K40–K46 for coronary artery bypass grafts and K49–K50 for coronary angioplasty. Emergency and elective procedures were combined. Since we were estimating need for stable angina, unstable angina, and myocardial infarction, which account for approximately 71% of indications for coronary revascularisation, we estimated the current actual provision for these indications by multiplying the total number of procedures carried out for all indications (n = 39 420 in HES database) by 0.71 (39 420 × 0.71 = 27 988).
RESULTS
A total of 461 400 people were estimated to develop incident or significantly worsening chronic stable angina, fatal and non-fatal myocardial infarction, and unstable angina each year (table 3⇓).
Coronary revascularisation need applied to 1998 England mid-year population compared with a model based on current patterns of investigation and treatment in England (men and women aged 45–84 years)
Model of current practice
On the basis of current general practitioner referral rates and hospital admission rates, we estimate that approximately 240 400 people are seen in secondary care with stable angina, acute myocardial infarction, or unstable angina every year (table 3⇑). The model of current practice predicted that 5% of patients with incident and worsening stable angina, 3% with fatal and non-fatal acute myocardial infarctions, and 14% with unstable angina undergo revascularisation. These proportions are in line with previous estimates.22,28,33
The model of current practice predicted 27 465 revascularisation procedures, within 2% of our estimate of actual provision of 27 988. This provides evidence in support of the validity of the six steps in the model and the estimates used. In the model of current practice, 49% of procedures were for stable angina, 8% for myocardial infarction, and 44% for unstable angina. This compares with relative proportions in the ACRE study of 61%, 12%, and 28%, respectively. This disparity may reflect the inclusion of emergency admissions for angina in our definition of unstable angina and the difficulties of distinguishing unstable angina from acute myocardial infarction.
Model of predicted need for coronary revascularisation
The model of need predicted that 356 400 people should be referred to secondary care. The proportions of new indications predicted to need revascularisation were 20% of stable angina cases, 10% of fatal and non-fatal acute myocardial infarctions, and 29% of unstable angina cases. The incidence of need for coronary revascularisation was predicted to be 92 000 among 45–84 year olds in England, equivalent to a rate of 1861 per million total population.
Overall, the model of need exceeded current provision by 3.3:1, although among people aged 75 and over the ratio was 7.7:1 (table 4⇓). In other words, the model of need predicts that provision in those aged 75–84 would have to increase by 670% above current National Health Service provision compared with an increase of around 140% in those aged 45–64 and 250% in those aged 65–74 (table 4⇓).
Age specific need for coronary revascularisation compared with current NHS provision
Sensitivity analysis
Figure 2⇓ shows the effects of varying model assumptions on predicted need for revascularisation. We sought to illustrate a plausible upper estimate of need and assumed that 90% of patients with stable angina were referred from primary care and that angiography would be performed in 65% of patients with acute myocardial infarction and 75% of patients with unstable angina. The increase in referrals from primary care had the greatest single impact, being associated with a predicated increase in revascularisation rates of 314 per million population. The combined impact of these three assumptions was to predict a population need for revascularisation of 2626 per million population.

{kind=link}
{kind=link}
Sensitivity analyses: effects of varying model assumptions on predicted need for revascularisation procedures in men and women aged 45–84 years. Assumption changed: (1) angina—90% of all patients with incident angina are referred to secondary care; (2) myocardial infarction—65% undergo angiography; (3) unstable angina—75% undergo angiography; (4) total—effect of changes in all three assumptions.
DISCUSSION
Objective addressed
We found that the recent government targets for revascularisation fall within a credible range of population need, although sensitivity analyses suggest that the need for revascularisation may be much higher. These targets may be reached in very different ways—for example, by increasing the referral rate of stable angina from primary care or by increasing the proportion of patients who undergo revascularisation after angiography. Underprovision is greatest among older age groups. These findings need to be considered together with the more global issue of other priorities for investment, including other disease areas and preventive treatment.
Advantages of the incidence of indications approach: articulating appropriateness
We have attempted to model the national need for coronary revascularisation by using an incidence of indications method.11 This approach offers a central advantage over other methods by transparently matching an estimate of ability to benefit to clinically meaningful patient groups or indications. The clinical judgement to perform coronary revascularisation is based on combinations of patient characteristics including the type and severity of presenting morbidity, number of diseased vessels, left ventricular function, and operative risk. For each indication the degree of benefit (in mortality or functional status) can be estimated. In some cases randomised trial evidence can be used, yet despite the accumulating number of trials there is considerable debate about appropriate rates of revascularisation.7,30,35–,38 This is partly because of the selected nature of trial participants, developments in current practice that have outpaced trials, and the lack of trials in primary care investigating referral strategies for angiography. This suggests that other, explicit methods are used to estimate benefit. Ours is the first attempt to incorporate the ratings of an expert panel of revascularisation appropriateness, in which the likelihood of benefit is rated on a nine point scale for specific indications. These ratings, which can be applied to virtually every patient, have been shown to be associated with clinical outcome14 and therefore offer an important tool in defining need.
Systematically identifying what we don’t know
The incidence of indications approach makes explicit where the major gaps in the evidence lie, giving a clear framework for improving the model with the results of further research. Two forms of new knowledge are required. Firstly, better estimates are required of the ability to benefit from certain management steps, for example, referral from primary care for a specialist opinion. There is a lack of clinical outcome studies investigating whether patients with suspected stable angina in primary care benefit from referral to secondary care. One trial suggests that aggressive medical management of such patients may avert the need for revascularisation.39 In the absence of large trials in primary care, this question can be addressed with expert panel methods. Secondly, better estimates are required of the incidence of specific indications. Thus, for stable angina the incidence (first ever presentation), as well as the incidence of worsening angina among prevalent cases, is uncertain. The incidence in the community of unstable angina, fulfilling the definitions used in clinical trials, is not known.
Primary care
Our model indicates that attainment of recent national targets requires changes in the management of chronic stable angina. Currently, most patients are managed within primary care. Increased facilities and staffing for the investigation of patients with angina would shift the emphasis for the initial management of these patients from primary care to secondary care.
However, by comparison with stable angina, the evidence base for measuring population need for revascularisation for the acute coronary syndromes is more robust. National HES data are available to estimate the incidence of patients with acute myocardial infarction surviving to reach secondary care and several randomised trials have compared different invasive management strategies among hospitalised patients.30 Despite the stronger evidence base there are still striking international variations in the proportion of people undergoing revascularisation following both acute myocardial infarction, ranging from 8–61%,28 and unstable angina, ranging from 2–60%.7 Since countries with very high revascularisation rates after myocardial infarction or unstable angina do not necessarily have better outcomes,7,31,36 the right revascularisation rate to benefit population health is unclear.
Age
The model of need and comparisons with the USA (table 1⇑) indicate that underprovision is greatest among patients aged 75 and older. We tested whether this disparity was an artefact of the lack of age specific angiography rates by modelling a range of extreme values. We found that the underprovision at older ages was robust to these changes in assumptions. The evidence base for the relative benefit of intervention in people of this age is less secure than that for younger people and there is no basis for judging whether older people would seek invasive treatment where there is no evidence of improved survival. In the original trials of coronary bypass surgery only 7% of subjects were over 60 years.40
Limitations: underestimating the need for revascularisation
The model may underestimate revascularisation need because we did not model (a) the backlog of patients with stable angina for whom referral to secondary care would be appropriate; (b) the backlog of patients waiting for revascularisation (for example, 16 000 patients were awaiting cardiothoracic surgery in 1999 (KH07 quarterly returns, Department of Health)); (c) the full range of patients with angiographically determined coronary artery disease who may benefit from revascularisation (the ACRE study showed that the benefits of revascularisation extended to patients in whom revascularisation was deemed of uncertain appropriateness); (d) repeat revascularisation after angioplasty (which even with the use of stenting and modern adjunctive treatment ranges from 5–17%);41,42 and (e) other indications such as valve disorders, heart defects, or near sudden death (we assumed that need for these uncommon indications was being met).
Limitations: overestimating the need for revascularisation
Conversely, the model may overestimate revascularisation need for four reasons. Firstly, the case mix of patients referred to secondary care may alter as referral rates increase, with greater proportions of milder angina, for which revascularisation is less effective, and more non-coronary chest pain. Thus, the assumption that the appropriate coronary angiography rate for stable angina cases is 51% (table 3⇑) may be too high. Secondly, aggressive medical management, particularly of lipids, may reduce the need for revascularisation; the benefits of maximising medical treatment versus revascularisation in relation to symptomatic control and quality of life remain unclear.39,43 Thirdly, a single patient may have an incident case of stable angina, unstable angina, and acute myocardial infarction in one year, thus leading to double or triple counting. Furthermore, 47% of angina admissions were coded as angina unspecified so we may have overestimated the incidence of unstable angina by up to 93%. A recent study (ENACT, European network for acute coronary treatment) suggested that the hospital admission rate for unstable angina may be approximately 0.2%,44 providing some support for the possibility that our estimate (5 per 1000 among 45–84 year olds) is an overestimate. Some of the difference, however, may have arisen because ENACT was a hospital based, pan-European study with no lower age limit. Fourthly, if falling rates of coronary heart disease mortality over time5 reflect a decline in the incidence of angina, unstable angina, and myocardial infarction, there may be a reduction in need for revascularisation.
Conclusion
Recent government targets for revascularisation fall within a credible range of population need. Studies in unselected patients that examine the impact on clinical outcome of key referral decisions, particularly from primary care, would substantially improve the ability to model need.
Acknowledgments
SF first thought of the idea. RMM reviewed the literature, abstracted the data, performed the analysis, and wrote the first draft. SF, DG, and HH commented on the drafts and made significant suggestions for improvements to the model, the writing of the paper, and the interpretation of the data. AB and KRK read drafts, commented on the clinical aspects of the study, suggested data sources and improvements to the model, and were involved in interpreting the results. RMM will act as guarantor for the study. We are indebted to a number of other people. HES data were made available by the Department of Health to the authors courtesy of the HES National Service Framework project (Professor Shah Ebrahim and colleagues), funded by a South and West Regional project research and development grant. Advice on using HES was obtained from Dr Steven Oliver, and Davidson Ho processed the HES database located at the Department of Social Medicine, University of Bristol. Angela Crook provided data from the ACRE database. We thank Drs Paul Roderick, Cam Bowie, Ali Round, and Ian Baker for useful discussions about the model and for sharing ideas, and Ronan Ryan for help with the study on general practitioner referral rates from the General Practice Research Database. Professor David Wood and Dr Kevin Fox provided data from their rapid access chest pain clinic. Dr Chris Cannon provided additional data from the TACTICS-TIMI 18 trial. HH is supported by a Department of Health National Public Health Career Scientist Award.