Article Text

Abstract
Objective To study the effects of a management programme on hospitalisation and health care costs one year after admission for heart failure.
Design Prospective, randomised trial.
Setting University hospital with a primary catchment area of 250 000 inhabitants.
Patients 190 patients (aged 65–84 years, 52.3% men) hospitalised because of heart failure.
Intervention Two types of patient management were compared. The intervention group received education on heart failure and self management, with follow up at an easy access, nurse directed outpatient clinic for one year after discharge. The control group was managed according to routine clinical practice.
Main outcome measures Time to readmission, days in hospital, and health care costs during one year.
Results The one year survival rate was 71.8% (n = 79) in the control group and 70.0% (n = 56) in the intervention group (NS). The mean time to readmission was longer in the intervention group than in the control group (141 (87) v106 (101); p < 0.05) and number of days in hospital tended to be fewer (4.2 (7.8) v 8.2 (14.3); p = 0.07). There was a trend towards a mean annual reduction in health care costs per patient of US$1300 (US$1 = SEK 7.76) in the intervention group compared with costs in the controls (US$3594 v 2294; p = 0.07).
Conclusions A management programme for patients with heart failure discharged after hospitalisation reduces health care costs and the need for readmission.
- heart failure
- hospitalisation
- management
- health care costs
- nurse led clinics
Statistics from Altmetric.com
The prevalence of heart failure is increasing and the rates of hospitalisation, especially among the elderly, constitute a problem for health care providers.1 ,2 Heart failure is the most common cause of hospitalisation due to cardiovascular disease in patients more than 65 years of age and is associated with frequent readmission, often within 30 days.3 ,4 Up to 40% of readmissions, often resulting from inadequate patient information and non-compliance, may be avoidable.5-7 Heart failure accounts for as much as 1% of all health care costs.8Therefore, there is a need for alternative strategies that aim to optimise the management of heart failure to curtail costs. It is inherent, however, that such strategies do not impair further the patients’ quality of life.
We hypothesised that a management programme for patients, with heart failure could reduce hospitalisation and health care costs without impairing quality of life. We conducted a prospective, randomised study to evaluate the efficacy of a management programme, by examining the time to readmission, overall hospitalisation days, and health care costs, one year after hospitalisation for heart failure.
Patients and methods
Patients aged 65–84 years who were hospitalised primarily because of heart failure between December 1991 and October 1993 at Malmö University Hospital were eligible for the study. Heart failure was diagnosed on the basis of characteristic signs and symptoms and was supported by at least one objective sign present on admission, such as pulmonary rales, peripheral oedema, congestion in a chest radiograph, or a third heart sound. Exclusion criteria were: (1) the presence of other serious disease that either prevented participation or was expected to significantly influence quality of life, morbidity, or mortality in the following year; (2) foreseeable follow up problems such as residence outside the hospital catchment area, serious alcohol or drug abuse, or psychiatric disease; (3) inability to understand or answer the study questionnaires; (4) participation in another clinical trial; or (5) discretion of the treating physician.
RANDOMISATION
The study was approved by the local ethics committee. The committee suggested that randomised consent should be obtained.9 ,10 Thus, eligible patients were randomised by computer generated allocation. Patients were invited to participate and informed consent was given on the basis of information relevant to the allocated study group. This procedure avoided bias arising from control patients being informed of the intervention strategy. It was presumed that this information was likely to influence outcome as some controls would employ the intervention strategy on their own initiative.
INTERVENTION
First, patients and their families received an education programme on heart failure, describing its pathophysiology and pharmacological and non-pharmacological treatment. Adherence to prescribed medication was emphasised and patients were offered a seven day medication organiser (Dosett) if the study nurse considered one to be appropriate. Second, patients received guidelines for self management of diuretics based on the signs and symptoms of worsening heart failure (increased body weight, ankle oedema, dyspnoea, and fatigue) or fluid depletion (rapid weight loss). These data were registered in a patient diary (body weight, ankle circumference, and heart failure symptoms were regularly recorded). The education programme consisted of two 30 minute information visits by a nurse during primary hospitalisation and a one hour information visit for patients and family two weeks after discharge. In-hospital information on pathophysiology and self management guidelines were contained in the patient diary. The group information, held by a study nurse, employed an oral and video presentation to reinforce the information given in hospital. A special effort was made to inform family members who were present. Time was available for questions to the study nurse. Finally, patients were followed up at an easy access, nurse directed, outpatient clinic. The nurse was available by telephone during office hours and was able to see patients at short notice. There was only one prescheduled visit by the nurse at eight months after discharge. Patients were encouraged to contact the study nurse if: their diuretic adjustments did not ameliorate symptoms within two to three days; they felt unsure about which course of action to take; there were profound changes in self management variables; or at their discretion.
The study nurses were registered nurses with experience of heart failure from coronary care units and clinical heart failure trials. They attended an overview lecture on heart failure before starting the study and were able to consult a cardiologist about specific patients at all times. They were also able to schedule doctors’ visits as they considered appropriate. Intervention patients were offered outpatient visits with doctors at the department of cardiology at one and four months after discharge. No guidelines for evaluation or treatment specific to the study were used and changes to treatment prescribed at discharge were made only if clinically indicated.
The control group was followed up at the outpatient clinic at the department of cardiology, by either cardiologists in private practice or primary care physicians as considered appropriate by the discharging consultant. The treating physician was free to evaluate or treat as appropriate.
DATA COLLECTION AND FOLLOW UP
Clinical assessment and registration of sociodemographic data were prespecified and followed a set protocol. Data on hospitalisation and outpatient visits after randomisation were collected prospectively using questionnaires and hospital records. Data on hospitalisation before randomisation were collected retrospectively from hospital records. Patients were followed up for one year. All patients were accounted for and deaths were verified by hospital records or death certificates.
EVALUATION OF QUALITY OF LIFE
Quality of life was evaluated using a disease specific questionnaire, the quality of life in heart failure questionnaire,11 a generic questionnaire, the Nottingham health profile, and the patients’ global self assessment.12-17 The questionnaires were self administered.
COST ANALYSIS
Data on doctors’ visits and readmissions were collected prospectively from patients and hospital records. Each contact with the study nurse was noted. Telephone calls were estimated as 10 minutes per call and outpatient visits as 30 minutes. All costs were based on the amounts charged by our hospital, a university teaching hospital, to patients not covered by Swedish health insurance. The rates charged by the hospital cover only hospital costs: they do not include profits or other costs. The rates are based on the mean daily cost for all patients hospitalised at a specific level of care, as rates pertaining to individual patients, and their specific costs, are not used in the Swedish health care system. The mean cost for hospitalisation was US$381 per day (US$1 = SEK 7.76), doctors’ visits US$129, and nurses’ visits US$39.
There were no standard rates for nurses’ telephone calls or in-hospital visits. The cost of the initial visits by the study nurse to patients in hospital was estimated to 50% of the cost of an outpatient visit—that is, US$20. Outpatient visits included administrative costs, nurses’ salaries, and overhead costs for the outpatient department. The estimated cost for inpatient visits included salaries and some administrative costs. Three telephone calls to the nurse were estimated to cost the same as an outpatient visit. The cost for intervention included inpatient visits by the nurses, the group information visit, and all outpatient visits and telephone calls made by the nurses.
STATISTICAL ANALYSIS
The two study groups were compared by the (two tailed)t test for normally distributed continuous variables and the χ2 test for nominal variables. The Mann-Whitney U test was used to test for differences in continuous variables that are not normally distributed. The Wilcoxon matched pairs test was used for within group comparison. Kaplan-Meier survival curves were constructed to assess differences between groups in the percentage of patients free from death or readmission during one year follow up. The difference between groups was evaluated using the log rank test. A p value of less than 0.05 was considered significant.
Results
BASELINE CHARACTERISTICS
A total of 206 eligible patients were randomised. Randomised consent was withheld by 16 patients (8%) randomised to the intervention group and by none randomised to the control group. Table 1shows the baseline characteristics for the control and intervention groups. The study patients were elderly (mean (SD) age 75.6 (5.3) years) and sex distribution was relatively even (47% were women). Heart failure was moderately severe: New York Heart Association functional class III being most predominant (62%). The most common cause of heart failure was ischaemic heart disease (53%). Seventy five per cent of patients had a left ventricular ejection fraction of less than 40%. The randomisation groups differed significantly only with regard to baseline left ventricular ejection fraction, which was lower in the intervention group.
Baseline characteristics of consenting, randomised patients
MORTALITY
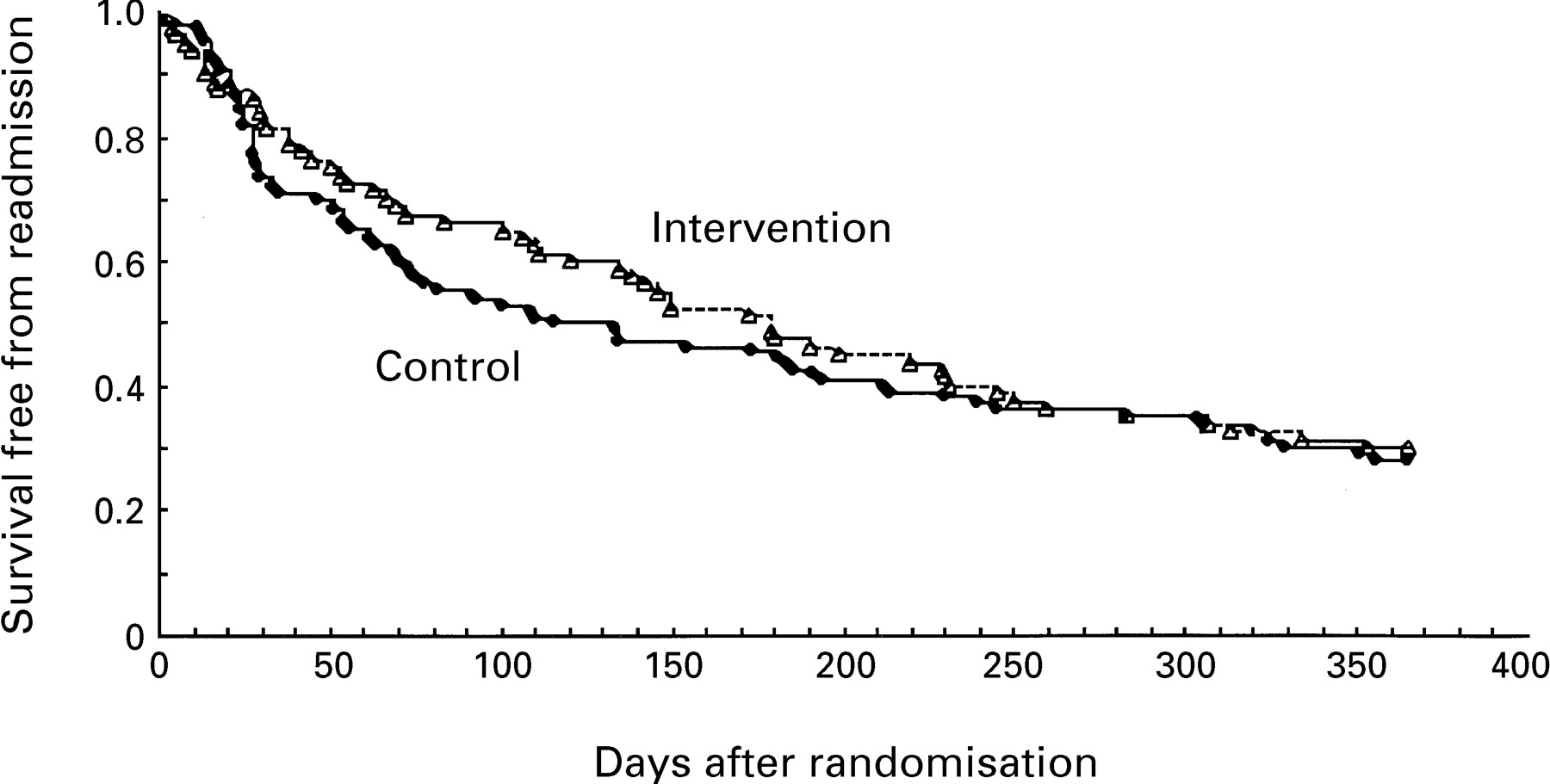
One year mortality did not differ between the intervention and control groups (24 (30%) v 31 (28%)). One patient (6%) who withheld consent died, while 53 (28%) of the remaining study patients died within one year (p = 0.06). There was no significant difference in the number of days hospitalised between the intervention and control groups among patients who died during one year follow up (15.4 (20.3) v 11.2 (16.3). As shown in fig 1, 56 patients (70%) in the intervention group died or were readmitted at least once compared with 79 patients (72%) in the control group (NS). The Kaplan-Meier curves diverge at an early stage in the trial because of a lower risk of death or readmission in the intervention group. At the end of the year, however, there was no significant difference between the groups.

{kind=link}
Kaplan-Meier survival curves showing the percentage of patients in each study group free from death and readmission.
HOSPITALISATION AND HEALTH CARE COSTS
Table 2 compares hospitalisation data at one year follow up for the intervention and control groups. Time to first readmission was longer (33%) in the intervention group than in the controls (p < 0.05). There was a trend towards fewer patients being hospitalised in the intervention group than in the control group (risk ratio 0.72; p = 0.08). The mean number of hospitalisations was 36% lower in the intervention group than in the controls (p = 0.08) and the mean number of days in hospital during follow up tended to be fewer in the intervention group than in the control group (4.2 (7.8)v 8.2 (14.3); p = 0.07). Outpatient visits were similar in the intervention and control groups (3.6 (3.2) v 4.0 (3.4)). Treatment for heart failure was similar in both groups at baseline (table 1), but there was a higher percentage of patients treated with angiotensin converting enzyme (ACE) inhibitors in the intervention group at one year follow up (table3).
Hospitalisation data in survivors at one year
Treatment at one year follow up
Hospitalisation one year before the study was compared with hospitalisation during the study period. The mean number of days hospitalised before the study was similar in the intervention and control groups (4.2 (7.9) v 5.2 (10.6)). During one year follow up there was an increase (59%) in the number of days hospitalised in the control group (5.1 (10.6) v 8.1 (14.3); p < 0.05), while there was no increase in the intervention group (4.2 (7.9) v 4.3 (7.8)).
The mean cost of intervention per patient was US$208. The cost of hospitalisation, because of readmission, tended to be lower in the intervention group than in the controls (table 4). Doctors’ outpatient visits were US$55 less in the intervention group. Hospitalisation was the major source of costs and the lower readmission rate in the intervention group contributed to a mean annual reduction in overall costs of US$1300 per patient (p = 0.07).
Mean annual health care costs (US$/patient)
HEALTH RELATED QUALITY OF LIFE
Health related quality of life did not differ between the intervention group and the control group at baseline (quality of life in heart failure questionnaire 4.5 (1.0) v 4.2 (1.1); Nottingham health profile 30.1 (21.6) v 26.9 (21.2); patients’ global self assessment 4.3 (1.5) v 3.7 (1.6)) or at one year follow up (quality of life in heart failure questionnaire 3.5 (1.3) v 3.5 (1.1); Nottingham health profile 25.3 (22.2) v 23.4 (22.2); patients, global self assessment 3.3 (1.4) v 3.2 (1.6)). Higher scores signify greater impairment of quality of life.
Discussion
In view of the increasing number of patients with heart failure and limited health care resources there is a need to optimise management. Management strategies, however, risk being deleterious to the patient if motivated only by cost containment. It is therefore inherent that such strategies are evaluated in a fashion similar to that of other treatments. The present study examined the effects of patient education and self management combined with an easy access, nurse directed follow up after hospitalisation for heart failure. Patients were older than in other trials but are representative of most patients hospitalised for heart failure.4
Teaching patients with chronic obstructive pulmonary disease about their illness had economic benefits similar to those of the present study.18 Rich et al studied the effects of a multidisciplinary approach aimed at reducing readmission in elderly patients with heart failure.19 Patients at high risk for early readmission were specifically included (in contrast to our study, which included all patients), resulting in readmission rates in the control group that were higher than in the present study. The approach adopted by Rich et al resulted in an absolute reduction in readmissions of 13%, and a reduction in days hospitalised of 36%. We found similar results, and despite the differences in intervention and duration of follow up between these studies supporting the conclusion that changes in the management of heart failure can reduce hospitalisation. However, Rich et al, who used a multifaceted intervention (including both medical and social service aspects), do not identify which elements of intervention led to the reduction in readmission. The present study, which focuses on the effects of a relatively limited intervention, shows that patient education, self management, and nurse directed follow up are of particular importance. Furthermore, follow up in the study by Richet al was only 90 days, therefore conclusions of long term efficacy are not possible. We believe that one year follow up is a suitable indicator of long term effects in elderly patients with heart failure given the prognosis. We have shown that a management programme not only postpones hospitalisation but results in a long term reduction.
The use of self management and nurse mediated follow up has been described in a smaller, uncontrolled trial by West et al.20 Hospitalisation during six months’ follow up was reduced by 87% compared with that before inclusion. Patients were contacted by nurse managers to implement treatment guidelines during follow up. The magnitude of the reduction in hospitalisation does not allow definite conclusions on the efficacy of the programme as the trial was not controlled. This is also true for an earlier trial, utilising a nurse practitioner for follow up, in which a similar reduction (86%) in hospitalisation was reported.21
Pharmacological treatment has been shown to reduce hospitalisation in clinical trials.22 ,23 In the trial reported by Westet al there was a significant increase in treatment with ACE inhibitors and hydralazine,20 which would be expected to favourably influence outcome. The use of ACE inhibitors in our study patients was low at index admission. This finding reflects the pattern of ACE inhibitor utilisation in Sweden. It also results from the lack of assessment of left ventricular function in some patients. In our study ACE inhibitors were prescribed to 75% of patients in the intervention group at one year follow up compared with 52% in the controls. This difference probably arises from the significantly lower left ventricular ejection fraction at baseline in the intervention group. These patients were therefore more likely to receive an ACE inhibitor. It is highly improbable that ACE inhibition alone can explain the differences in hospitalisation and health care costs between the two groups.22
STUDY LIMITATIONS
The present study has several limitations. First, the study population was specifically selected and relatively free from other serious disease. Concomitant disease is, however, common in patients with heart failure and the possibility that increased health care access might lead to an increase in hospitalisation cannot be excluded.24 Second, some patients who were randomised to intervention withheld consent. These patients did not significantly differ from the participating patients, although the trend towards lower mortality suggests that more healthier patients tended not to participate. If this is true, then participation of these patients would have improved further the effects of intervention. Third, as a single centre study many doctors at our hospital were familiar with the intervention and may have applied some of the principles in the control patients. This limitation in combination with the fact that the use of patient self management, patient education, and nurse directed follow up became a part of clinical routine in a heart failure unit opened towards the end of the study may have led to a reduction in hospitalisation of control patients. Finally, the study population was recruited from hospitalised patients and thus definite conclusions regarding the effect of the intervention on an outpatient population cannot be drawn. Further study is necessary.
CONCLUSIONS
A management programme for patients with heart failure, including patient education, self management, and follow up at an easy access, nurse directed outpatient clinic for one year after hospitalisation, can reduce subsequent readmission and health care costs without impairing quality of life.
Acknowledgments
We thank nurses Anneli Iwarson, Marie Holmberg, and Katarina Reuterskiöld for help in designing the intervention and dedication in performing the study, and Fredrik Andersson for reviewing the manuscript and providing valuable advice about the health economic evaluation. The study was supported by grants from the Swedish Heart and Lung Foundation, the research foundation administered by Malmö University Hospital, and the Council for Health Care Research, Lund University.