Article Text

Abstract
Objectives To investigate the use of oral anticoagulants (AC) and antiplatelet agents (AP) in the management of atrial fibrillation (AF) among patients in primary care in England.
Design Epidemiological study.
Setting 1857 general practices in England representing a practice population of 13.1 million registered patients.
Patients 231 833 patients with a history of AF.
Main outcome measures The primary outcome was AC and AP use by CHADS2 score and age groups <30 years, 30–49 years, 50–64 years, 65–79 years and >79 years.
Results 231 833 patients with a history of AF were identified, giving a prevalence among uploading practices of 1.76%. Prevalence of AF varied markedly between practices, related to differing practice age profiles. The total number of patients with AF in a practice was strongly predicted by the number of patients aged 65 years and over in the practice. 57.0% of the AF population had a CHADS2 score ≥2 and 83.7%≥1. 114 212 (49.3%) patients received AC therapy. AC uptake increased with increasing CHADS2 score up to a score of 3, but thereafter reached a plateau. Among 132 099 patients with a CHADS2 score ≥2, 72 211 (54.7%) received an AC, 14 987(11.3%) were recorded as having a contraindication or having declined AC therapy, leaving 44 901 (34.0%) not on AC therapy and without a recorded contraindication or recorded refusal. Among patients not prescribed an AC, 79.9% were prescribed an AP. The use of AC declined in the elderly (for CHADS2≥2, 47.4% of patients ≥80 years, compared with 64.5% for patients aged <80 years, p<0.001). By contrast, AP uptake was more prevalent among elderly patients.
Conclusions Over one-third of patients with AF and known risk factors who are eligible for AC do not receive them. There is a high use of AP among patients not receiving AC. Uptake of AC is particularly poor among patients aged 80 years and over.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Atrial fibrillation (AF) is a major preventable cause of stroke.1 Despite the fact that anticoagulation is very effective in preventing strokes due to AF,2 there is extensive evidence that anticoagulants (AC) remain underused.3–11 This underuse of AC is reflected in the low utilisation among patients with known AF presenting with stroke.12 Appropriate AC is particularly important among the elderly, as this group is at greatest risk of strokes attributable to AF.13
Risk factors for stroke among patients with AF are well recognised.14 Many of these risk factors are based on simple clinical information from the patient's history that is readily available in primary care databases. Database interrogation, therefore, has the potential to identify patients at increased risk of stroke and to determine whether these patients are treated with AC therapy.
The Guidance on Risk Assessment and Stroke Prevention in Atrial Fibrillation (GRASP-AF) tool is a software suite which searches general practice clinical information systems to enable practices to identify patients with a history of AF and review the risk profile of individual patients. The tool is based on the widely used CHADS2 risk evaluation system.15 The aggregated uploaded information from GRASP-AF is the basis of the present study which provides insights into the prevalence and contemporary management of AF in England.
Methods
The GRASP-AF registry
The GRASP-AF tool is based on the use of MIQUEST (Morbidity Information QUery and Export SynTax), a common query process supported by all the primary care databases in England. The tool, which was developed jointly by the West Yorkshire Cardiovascular Network and PRIMIS (Primary Care Information Services) from The University of Nottingham, is managed by NHS Improvement in conjunction with PRIMIS. It is based on the CHADS2 risk evaluation system. Practice participation and uploading of data to the central server is voluntary.
Study population
A set of Read codes was identified (see online supplementary appendix 1) to search for patients with a history of AF, or atrial flutter, occurring at any time in a patient's history. In a subgroup of patients, interrogation additionally included a search for an AF resolved code, where this had been recorded. Patients listed as AF resolved were still included in the overall analysis.
Further searches were undertaken to identify Read codes of clinical characteristics related to stroke risk (see online supplementary appendix 1). In the initial iteration of the tool reported here, estimation of stroke risk was based on the individual components of CHADS2 score, namely a history of heart failure, a history of hypertension, the patient's age, a history of diabetes and a history of stroke or transient ischaemic attack. All diagnoses were considered positive for CHADS2 scoring if the patient had a history of these conditions at any time in the past.
The database was additionally interrogated to determine whether the patient had been issued with a prescription for AC within the last 6 months (initially warfarin, acenocoumarol and phenindione, but later expanded to include the new oral AC, dabigatran, rivaroxaban and apixaban), or whether an AC had been prescribed by a third party. Interrogation was also undertaken to detect whether the patient had an existing coding for a contraindication to AC, or if a patient had declined AC therapy. Interrogation similarly assessed prescription issue for antiplatelet agents (AP) therapy (aspirin, clopidogrel or dipyridamole), and whether an AP agent had been coded as contraindicated or declined.
Data uploading
The GRASP-AF tool is designed to provide patient-level data on the CHADS2 score and AC and AP prescribing within a practice. Additionally, the data are summarised at practice level as a dashboard (see online supplementary appendix 2). Practices also have the opportunity to upload anonymised aggregated data to a central server. Uploaded data were aggregated by age bands (less than 30 years, 30–49 years, 50–64 years, 65–79 years and 80 years and over), use of AC or AP drugs and by CHADS2 score. Population data for the practice, aggregated along the same age bands, was also uploaded for AF prevalence analysis.
Practices were encouraged to send data on first using the GRASP-AF tool in order to obtain a baseline set of results, which they could then use to compare with later uploads to assess any changes. Only the initial upload was considered for the current analysis. This report relates to data uploaded between 25 July 2009 and 31 March 2012.
Cohort analysis
Using the total number of patients with AF as the numerator and the total number of patients registered in practices as the denominator, we calculated the prevalence of AF by age group. The use of AC and AP for each CHADS2 score was calculated from the number of AF patients issued a prescription for an AC or AP divided by the number of AF patients with that CHADS2 score.
For each age group and for combinations of age groups, the relationship between the total number of patients with AF in an individual practice, and the total number of registered patients in that practice was depicted using scatter plots, quantified using generalised linear models with heteroskedasticity-consistent estimation, and the linear dependence measured using Pearson's correlation coefficient, to identify the age group which had the strongest association with total AF burden in the practice.
The relationship between the proportion of patients with AF on AC and AP was investigated using generalised linear models with a logit link and binomial distribution. For AC and AP, sequential models were fitted which regressed the proportion of patients with AF on an anticoagulant on age group, CHADS2 score, age group*CHADS2 score interaction, and compared with the null model. All analyses were performed using R V.2.10.1 (http://www.r-project.org/). Ethical approval was not required under NHS research governance arrangements for the project.
Results
Prevalence of AF
In total, 1857 general practices uploaded their data during the period of the study. Among an overall practice population of 13.1 million patients, 231 833 patients with a history of AF were detected by the tool. The overall prevalence of patients with a history of AF was 1.76%. Interrogation for an AF resolved code was undertaken in a subgroup of 389 general practices. In these practices, an AF-resolved code, with no later AF diagnosis code, was recorded in 6.1% of all patients with a history of AF.
Figure 1 shows that the prevalence of AF varied between practices and increased substantially with age. Considering all age groups combined, the median prevalence among uploading practices was 1.70% (IQR 1.28%–2.08%).

Prevalence of atrial fibrillation by age group. For each age group, the box plot represents the IQR, and the whiskers extend by a further 1.5 times the IQR. Individual outlying practices beyond this are shown as individual points.
The overall number of patients in a practice was a relatively poor predictor of the total number of patients with AF in that practice. By contrast, the total number of patients aged 50 years and over, 65 years and over and 80 years and over in individual practices, each strongly correlated with the total number of patients with AF for that practice. The strongest association between age group and total number of patients with AF was observed for patients aged 65 years and over—an increase in 1000 patients aged 65 years and over in a practice was associated with, on average, an increase of 101.5 patients with AF (95% CI 100.7 to 102.2) (figure 2).
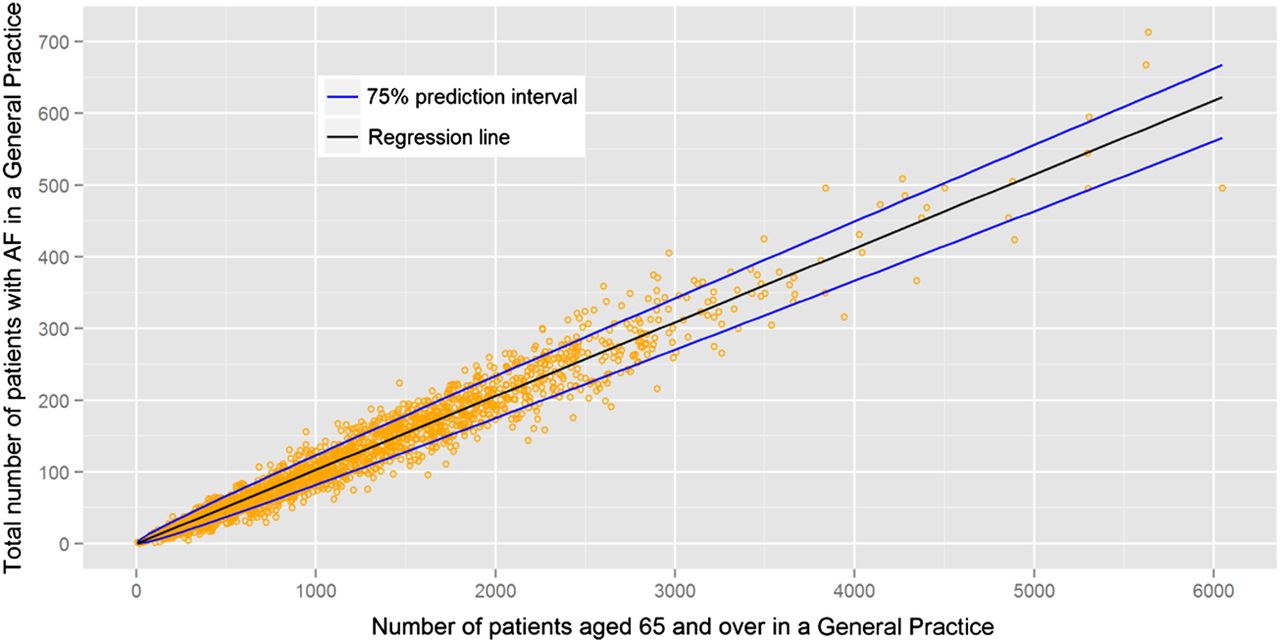
Scatter plot of the total number of patients with atrial fibrillation in a practice related to the number of patients in a practice, aged 65 years and over. Each dot represents an individual practice. Black line: regression line, β=0.1015 (95% CI 0.1007 to 0.1022). Blue lines: 75% prediction interval. Modelling was performed using a square root transform of both variables to account for heteroskedasticity. Pearson's correlation coefficient, R=0.98, p<0.001.
Prescription of AC and AP
Overall, the proportion of patients with AF who were prescribed AC and AP was 49.3% and 42.5%, respectively, with 6.9% of patients being prescribed both AC and AP. The proportion of patients with AF who were prescribed AC and AP varied by practice (IQR: AC 44.4–55.1%; AP 37.7–47.8%). For both AC and AP, a greater proportion of patients was recorded as therapy contraindicated than therapy declined (AC: contraindicated 8.7%, declined 1.9%; AP: contraindicated 14.0%, declined 0.5%). The proportion of patients in whom there was a recorded contraindication to the therapies varied considerably by practice (IQR: AC 2.6–12.0%; AP 6.1–20.0%). Among the AF-resolved subgroup, 9.4% were prescribed AC, 30.2% an AP and 1.9% both.
CHADS2 scores and anticoagulation
In total, 57.0% of the AF population had a CHADS2 score of ≥2 and 83.7%≥1. The proportion of patients with a CHADS2 score of ≥2 varied by practice (IQR 52.4–61.9%). Table 1 shows that the prescription of both AC and AP increased with increasing CHADS2 score for scores 0–3, and plateaued thereafter to reach 58.1% for AC and 46.5% for AP at a score of 6.
Frequency of prescriptions, contra-indications and declines for anticoagulant therapy and antiplatelet therapy by CHADS2 score
Among patients with a CHADS2 score ≥2, 54.7% were prescribed an AC, 9.2% were listed as AC contraindicated and 2.2% were recorded as having declined AC therapy. In total, 34.0% of patients with AF who had a CHADS2 score ≥2 were, therefore, not recorded as having been prescribed an AC with no recording of a contraindication or having declined AC therapy.
The uptake of AP also increased with CHADS2 score. Among patients with a CHADS2 score ≥2, 36.2% were prescribed solely an AP, with 90.9% being prescribed either an AC or AP or both. Among patients who did not receive an AC, 79.9% were prescribed an AP.
Age and prescription of AC and antiplatelet therapy
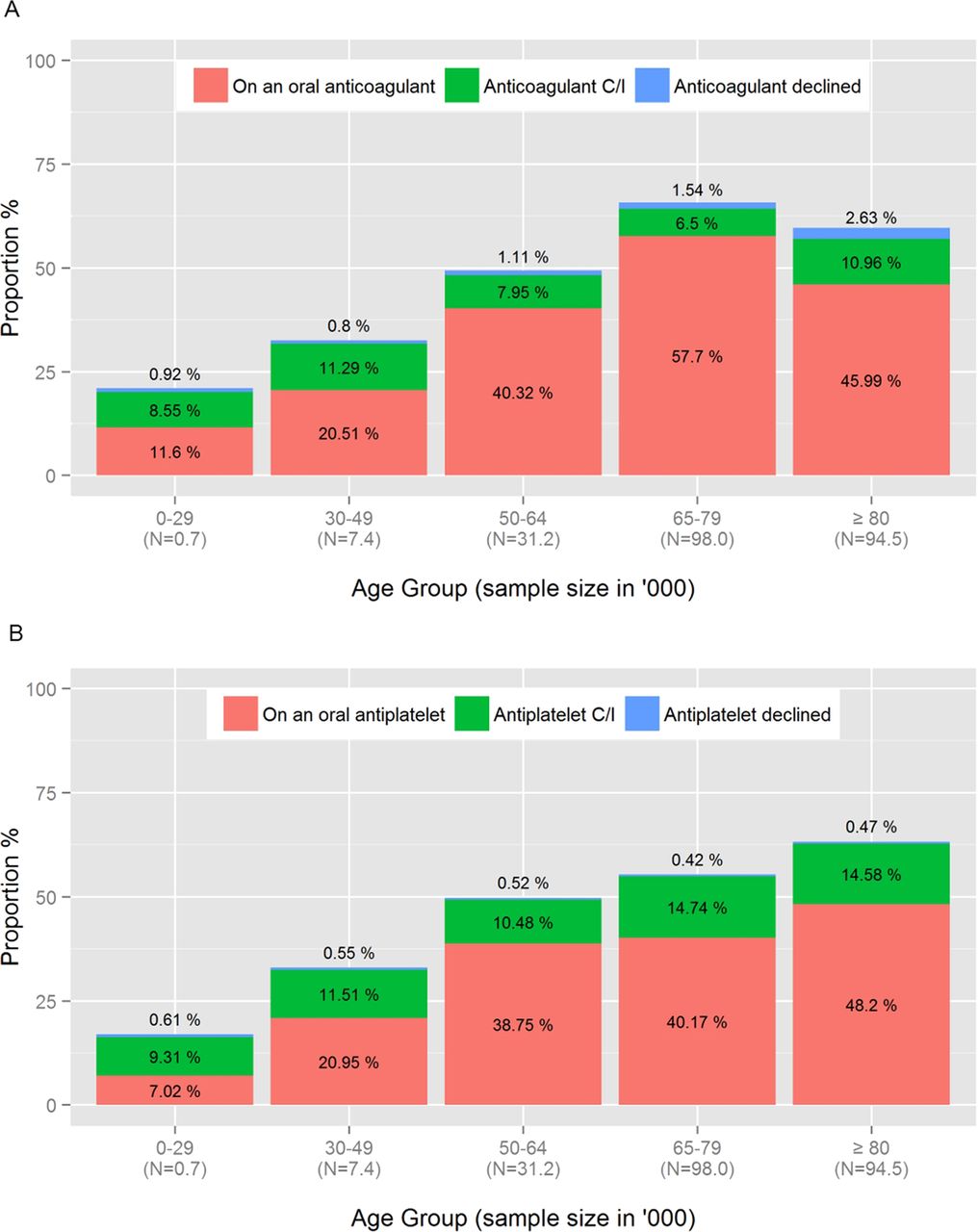
Figure 3A shows that the uptake of AC therapy increased with age for patients aged less than 80 years, but decreased in patients aged 80 years and over. By contrast, AP use continued to increase with age in patients aged 80 years and over (figure 3B).

The proportion of atrial fibrillation patients prescribed anticoagulant therapy (A) and antiplatelet therapy (B) by age group.
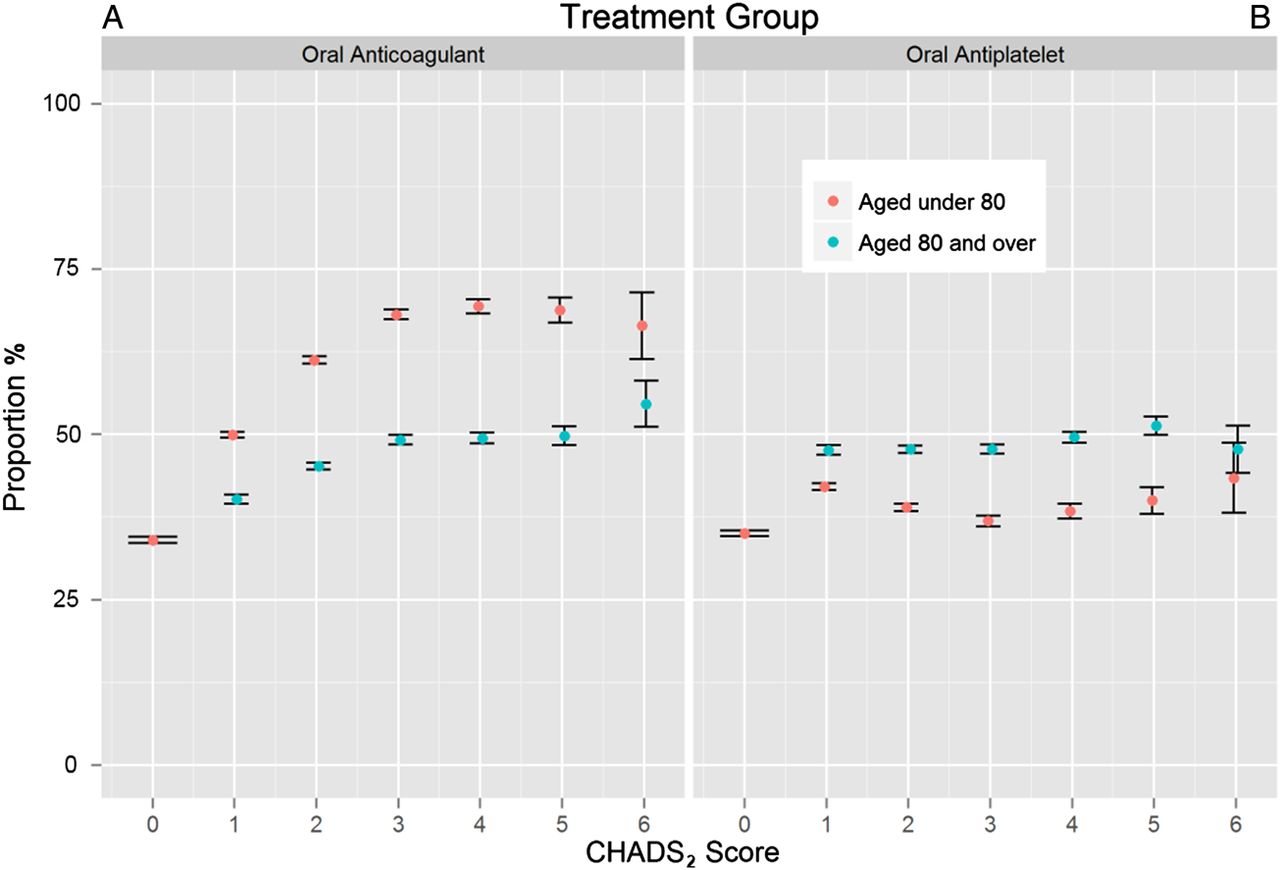
This age-dependent difference in the prescription of anticoagulant therapy for AF was explored further by assessing AC and AP use across the range of CHADS2 scores in relation to age (figure 4). For CHADS2 scores 1–6, the proportion prescribed an AC was lower in those aged 80 years and over, than in those aged less than 80 years. Conversely, for patients with a CHADS2 score from 1 to 6, the proportion with AF prescribed an AP was higher in those aged 80 years and over and remained relatively constant across scores (figure 4B). In the generalised linear models, the evidence for an effect of age group on the prescription of AC and AP by CHADS2 score was strong (AC p<0.001, AP p<0.001). Overall, among high-risk patients with CHADS2≥2, the prescription of AC was 47.4% for patients aged 80 years and over compared with 64.5% for patients aged under 80 years. This difference was only partly accounted for by differences in recorded contraindications to AC (≥80 years, 11.2% vs <80 years, 6.5%) or patients declining AC (≥80 years, 2.7% vs <80 years, 1.5%).

Proportion (95% CI) of atrial fibrillation patients prescribed anticoagulant therapy (A) and antiplatelet therapy (B) by CHADS2 score for patients aged 80 years and over, and for patients aged under 80 years.
Figure 5 shows how the proportion of patients with a CHADS2≥2 prescribed AC varied between practices. The uptake of AC was higher among patients aged under 80 years than in those aged 80 years and over. Approximately one-quarter of practices (23.5%) prescribed AC to 56.5% or more of eligible patients aged 80 years and over, whereas for patients aged less than 80 years, three-quarters of practices (76.5%) achieved this same level of AC uptake.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proportion of patients with CHADS2≥2 prescribed anticoagulant therapy by age under 80 years and age 80 years and over, with kernel density estimates for each age group distribution.
Discussion
AF prevalence
This study of AF in general practices in England reveals that the overall prevalence of AF among practices uploading data from 2009 through 2012 was 1.76%. This estimate is higher than previous reports. In 2006, NICE (National Institute for Health and Clinical Excellence) estimated the prevalence of AF was 1.28%.16 This was based on a 1998 survey of 211 general practices representing a total population of 1.4 million patients in England and Wales.7
It is not surprising that the prevalence estimate in the current study exceeds previous UK-based estimates. This may partly reflect a recognised trend for AF prevalence to increase over time.6 ,17 It also may reflect the methodology of the current study which included patients with a diagnosis of AF at any time in their patient record. In designing the interrogation tool it was decided from the outset to include all episodes of AF and not to make any attempt based on database interrogation to assess whether susceptibility to AF might have resolved. This was left to clinician judgement and individual case review. While it is certainly true that there are situations in which AF may be regarded as resolved, many patients with a single episode of AF are susceptible to recurrence, and a case can, therefore, be put forward for both regular review and for continuing AC despite apparent resolution.
The marked effect of age on AF prevalence observed in the present study is well recognised. This effect largely accounted for apparent differences in prevalence between individual practices. The total number of patients with AF in a practice could be predicted as 10.15% of the number of patients aged 65 years and over. This relation provides a potential tool for practices to benchmark their individual AF prevalence value in relation to their practice age profile. It also provides a means of projecting the increase in AF prevalence which will be associated with ageing of the population.
Anticoagulant uptake among patients with AF
The GRASP-AF tool provides an estimate of the number of patients with AF who are currently receiving an AC. Overall, just less than half (49.3%) the number of patients with a history of AF received an AC.
The study also provides an estimate of the number of patients eligible for treatment in relation to risk stratification strategies. If treatment were to be targeted on patients with a CHADS2≥2, this would cover 57% of the AF population. This is almost identical to a recent estimate of 56.9% which was based on 583 UK general practices.6 If the treatment threshold for AC therapy is reduced to CHADS2≥1, this would target 84% of the AF population. It is not possible to retrospectively analyse our data to assess the consequences of using the more sensitive CHA2DS2VASc risk stratification system.14 The tool has now been modified to additionally make a CHA2DS2VASc risk score available to users.
It is clear from the current data that there is a relationship between patients’ degree of risk as determined by CHADS2 score and AC uptake. Our study clearly shows that AC uptake increased through CHADS2 scores 0–3, and thereafter reached a plateau. A very similar relation is apparent in the recently reported study of UK practices.6 These findings differ from the observations of Gallagher et al,18 which were based on observations on 41 910 patients with chronic AF in a UK general practice database. Data collection in their study commenced in 2000. They found that patients with a lower CHADS2 score were more likely to be prescribed warfarin than patients with a higher CHADS2 score. Our findings also differ from those of Sandhu et al19 who assessed the uptake of AC in relation to risk among 42 834 Canadian patients with non-valvular AF assessed during the period 2000–2005. They found that AC uptake did not vary across CHADS2 risk categories. Our study, together with that of Holt et al, suggest that risk stratification plays a greater role in contemporary therapy than was the case a decade ago, and may indicate that the 2006 NICE guideline has had some impact on therapy among general practices in England.
Gallagher et al18 reported that approximately 60% of patients with a CHADS2 score ≥2 in the UK did not receive warfarin. Holt et al6 found that this had reduced to 47.0%, and our own study suggests further improvement to 45.3%. After allowing for patients in whom AC was contraindicated or declined, 34.0% of patients with CHADS2≥2 in the current study did not receive an anticoagulant.
The fact that 36.2% of patients with CHADS2≥2 were prescribed AP without AC suggests an over-reliance on AP for stroke prevention in AF. The superiority of warfarin over aspirin for stroke prevention in high-risk patients was clearly recognised in the NICE guidance which applied throughout the duration of the study.16 The high use of AP may partly reflect the recommendations of the Quality and Outcomes Framework (QOF) of the NHS (National Health Service) which provided equal emphasis on AC and AP in stroke prevention throughout the study period. This may have contributed to the fact that 90.9% of patients with CHADS2≥2 were treated with either an AC or AP or both, thereby fulfilling the stated objectives of QOF at that time.
Our data shows an age-dependent inequality in the prescription of AC and AP. Reduced prescribing of AC among elderly patients with AF has been observed in previous studies.4 ,11 ,18–22 A recent survey of UK general practices database records from 2000 to 2009 showed that this underuse of AC therapy in the elderly is not adequately explained by either an increase in comorbidities or in bleeding risk.23 The current study has shown that there is an increase in prescribing of AP agents for elderly patients. This is in stark contrast with the results of the Birmingham Atrial Fibrillation Treatment of the Aged (BAFTA) study24 demonstrating superiority of warfarin over aspirin in stroke prevention in the elderly and, perhaps, represents a misconception that aspirin is safer than warfarin in a more elderly population. It illustrates the risk-treatment paradox previously reported in AF management,19 that patients at higher risk of stroke, and more likely to benefit from AC therapy, are not receiving appropriate treatment—perhaps because of a perceived increased risk of side effects associated with warfarin therapy in the elderly.
The GRASP-AF data also demonstrate the considerable variation between practices both in the uptake of AC among high-risk patients and in the coded contraindications to AC therapy. That such variation exists, suggests that there is substantial scope to improve AC uptake in AF. Based on the observations from the current study of the proportion of patients who are high-risk (CHADS2≥2), and the proportion of these patients who are not on AC with no documentation of contraindication or therapy decline, combined with Office of National Statistics (ONS) population estimates for England,25 we estimate that there were approximately 169 000 such patients in England between 2009 and 2012. Most of these patients were taking aspirin. Based on a number needed to treat from the BAFTA study of 50 to prevent one thromboembolic event or intracranial haemorrhage,24 in excess of 3000 strokes could potentially be prevented annually if these individuals were commenced on AC in preference to AP.
Limitations of the current study
The data in this report represent uploaded information from 21.2% of general practices in England. In that practices that elected to upload their data, GRASP-AF is not a random sample, and it is possible that the sample, although large, is not representative of the primary care population in England. The proportion of patients aged 65 years and over in the population of practices uploading GRASP-AF data, is higher than that reported by the ONS 2010 estimate for England (17.3% vs 16.5%).25 There may, therefore, be a slight over-representation of elderly patients among practices uploading data.
The GRASP-AF tool interrogates general practice records, and is limited by the accuracy of coding in these records. The results reported in this study may under-represent comorbidities and, hence, overall stroke risk.6 For recorded contraindications, coding may once again be an under-representation, but as it represents perceived contraindications, there is the additional possibility for over-representation. The modelling of aggregated data to quantify the relationship between AF burden and age, and to study the interaction between AC use by CHADS2 score in the elderly may be biased by mathematical coupling of the data. Nonetheless, we explored a number of model strategies to find good model fits and robust estimates.
Conclusions
Over 20% of general practices in England have uploaded data on their AF patients using the GRASP-AF tool. Analysis of these data show that uptake of AC has improved in comparison with previous studies, but even so, over one-third of high-risk patients remain untreated. AP agents are very frequently used as an alternative, particularly among the elderly. Education on the benefits of AC in comparison with AP offers great potential for stroke prevention.
Acknowledgments
We would like to acknowledge and thank the general practitioners and practice staff throughout England who contributed to this analysis through uploading their practice data together with the clinical advisors and the development team at PRIMIS. Additionally, we would particularly like to thank Adele Graham, Kathryn Griffith, Shona Holding and David Fitzmaurice who contributed to the development of the GRASP tool.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix 1
- Data supplement 2 - Online appendix 2
Footnotes
-
Contributors CC, original concept, pilot, initial national roll-out and writing. RH, overall national supervision of GRASP-AF. IR, national data collection. WRL, data analysis and statistical assistance. JB, coordination at PRIMIS and data analysis. MF, primary care advice. KT, initial development and pilot study. CPG overview of data analysis and writing. Guarantors CC, CPG.
-
Funding The initial development of the GRASP-AF tool was funded by the West Yorkshire Cardiovascular Network and subsequent development funded by NHS Improvement.
-
Competing interests MF has received honoraria and travel grants from Boehringer-Ingleheim, Bayer, Bristol Myers Squibb, INRStar, Pfizer and Roche. Apart from this, and the involvement of NHS Improvement, the authors have no competing interests.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Practices uploading to GRASP-AF did so under a guarantee of anonymity, and the data is subject to a data collection agreement which states that only contributing practices, PCT information facilitators, PRIMIS staff and other workers validated by NHS Improvement will have access to the data. Therefore, practice-level data is only available to individuals meeting these criteria. However, the data collection agreement also states that the data will be used for the purposes of comparative analysis and that anonymised data may be used by NHS Improvement to understand and monitor the management of stroke risk in AF. To this end, NHS Improvement will consider release of the highest-level aggregated data on request. Any such requests should be submitted to RH for consideration.