Article Text

Abstract
Background: The thrombolysis in myocardial infarction (TIMI) risk score has been shown to risk stratify patients with suspected acute coronary syndromes (ACS) effectively in the emergency department (ED) but cannot be used to guide patient disposition. We aimed to evaluate whether modifying the TIMI risk score to give greater weighting to ischaemic ECG changes and troponin elevations would enhance its risk stratification and thus potentially facilitate safe patient discharge after 12-h troponin testing.
Methods: A prospective diagnostic cohort study was performed within the ED at Manchester Royal Infirmary, a university-affiliated teaching hospital with an annual ED census of approximately 145 000 patients. 804 patients who had presented to the ED with suspected cardiac chest pain were recruited. All patients underwent 12-h troponin T testing and were followed up by telephone and chart review after 30 days for the composite primary outcome of death, acute myocardial infarction (AMI) or urgent coronary revascularisation.
Results: The modified TIMI risk score outperformed the original (area under the receiver operator characteristic curve 0.87 versus 0.77, p<0.001). Using a cut-off of more than 2 points the score had a sensitivity of 96.4% for the prediction of 30-day events. The specificity of the score was only 51.0%, suggesting that in practice over 40% of patients would be ineligible for discharge even after troponin testing.
Conclusions: Modifications to the TIMI risk score can improve its performance in the risk stratification of patients presenting to the ED with chest pain. However, a lack of specificity may still limit its use for guiding patient disposition after troponin testing.
Statistics from Altmetric.com
Suspected cardiac chest pain accounts for approximately 20% of all acute medical admissions at a cost of over £900 million in the UK alone.1 2 Only approximately 25% of admitted patients will prove to have an acute coronary syndrome (ACS).3 4 There is therefore tremendous potential to reduce unnecessary hospital admissions in this patient group.
Troponins are the gold standard biochemical markers for the diagnosis of acute myocardial infarction (AMI);5 they are also commonly used as the sole discriminator when deciding whether patients need further inpatient investigation and management. Patients with unstable angina are, however, by definition, troponin negative.6 7 It is not always easy to distinguish unstable angina from stable angina and non-cardiac chest pain on clinical grounds alone.8 Almost 6% of patients with suspected ACS but normal troponin levels will die or have an AMI within 12 weeks.9 Even patients with both normal troponin and non-diagnostic ECG have a 5.4% incidence of death, AMI or urgent revascularisation (UR) by 14 days,10 a 1.5% mortality by 6 months11 and a 6.7–8% mortality by one year.12 Clearly, a risk stratification tool that helps to identify high-risk individuals while facilitating safe discharge for others is desirable.
The thrombolysis in myocardial infarction (TIMI) risk score for non-ST elevation ACS has been shown to risk stratify patients with confirmed ACS13 14 and has been validated in the undifferentiated emergency department (ED) population.15–18 However, in the ED setting the relative underweighting of ischaemic ECG changes and troponin elevations (both score only 1 point in the TIMI score) is contrary to past research, as both are known to be powerful independent predictors of prognosis.11 12 19 20 In practice, the presence of either criterion would usually prevent a patient from being labelled as “low risk” and would indicate the need for hospital admission.21
Our aim was to evaluate whether pragmatic modifications to the TIMI risk score are likely to enhance its performance for the identification of populations who are at high and low risk of adverse cardiac events within 30 days.
METHODS
Study design and setting
This is a substudy of the Early Vascular Markers of Acute Coronary Syndromes (EVaMACS) study, a single-centre prospective diagnostic cohort study. The study was approved by the local research ethics committee (reference 05/Q1410/27). All patients provided written informed consent. We recruited patients at Manchester Royal Infirmary, a university-affiliated teaching hospital with an annual ED census of approximately 145 000.
Selection of participants
Consecutive patients aged over 25 years who presented to the ED with a primary complaint of chest pain that the initial treating physician suspected may be cardiac in nature were eligible for inclusion. Patients were excluded if they had another medical condition requiring hospital admission, renal failure needing dialysis, significant chest trauma with suspicion of myocardial contusion, if they were pregnant, did not speak English, were prisoners or if their most significant episode of chest pain was more than 24 h before ED presentation.
Data collection and processing
Clinical data were recorded in the ED by the treating physician on a custom-designed patient report form. The TIMI risk score was extracted later and entered into a database using Microsoft Access 2003. The patient report form did not calculate or advise the clinician of the TIMI risk score. Similarly, clinical data were not entered into the database and TIMI risk scores were not calculated until after outcomes had been assessed. The TIMI risk score was not used to influence patient care during the study period.
Under the ED protocol low-risk patients could be investigated in the ED observation ward with serial creatine kinase myocardial-type mass estimation and 6 h of ST-segment monitoring.21 However, the study protocol mandated that all patients also had blood taken for troponin T testing 12 h or more after the onset of their most significant symptoms (Roche Diagnostics, 99th percentile 0.01 ng/ml; coefficient of variation <10% at 0.035 ng/ml) in accordance with current guidelines.7 22 If patients were discharged before 12-h troponin testing they were recalled or visited at home. Following assessment and initial management in the ED, patients were referred to the medical admissions unit, coronary care unit, cardiology ward, ED observation ward or discharged home according to the discretion of the physicians responsible for their care.
The TIMI risk score was assessed using previously reported criteria.16 Because ischaemic ECG changes and troponin elevations are known independently to identify high-risk populations who would not ordinarily be considered for discharge from the ED, we modified the score so that the presence of either or both of these criteria would score 5 points, thus automatically identifying these patients as high risk. All other TIMI criteria scored 1 point. The modified TIMI risk score was therefore scored from 0 to 10 points (table 1). Every ECG was reported by the treating physician using the patient report form. The patient report form directly asked whether there were acute ischaemic features.
All patients were followed up 30 days post-presentation. At that time the patient’s outcome was checked by examining the National Health Strategic Tracing Service database for mortality data and hospital records for clinic letters, investigation reports and details of hospital admissions and/or ED attendances. Patients were then interviewed by telephone. If no contact could be established with the patient, their general practitioner was contacted.
Outcome measures
The principal outcomes were death, AMI (excluding the index event) and urgent coronary revascularisation. Coronary revascularisation included the detection of a new angiographic coronary stenosis of 50% or greater in which revascularisation could not be achieved, as reported by the patient’s interventional cardiologist. AMI was defined according to American Heart Association and European Society of Cardiology guidelines.5 The diagnostic troponin cut-off was set at the smallest value above the 99th percentile at which the coefficient of variation was 10% or less (0.035 ng/ml).23
Statistical methods
Sensitivity, specificity, predictive values and confidence intervals were calculated using Stats Direct version 2.6.1. Other data were analysed using SPSS version 12.0 or MedCalc 9.3.9.0.
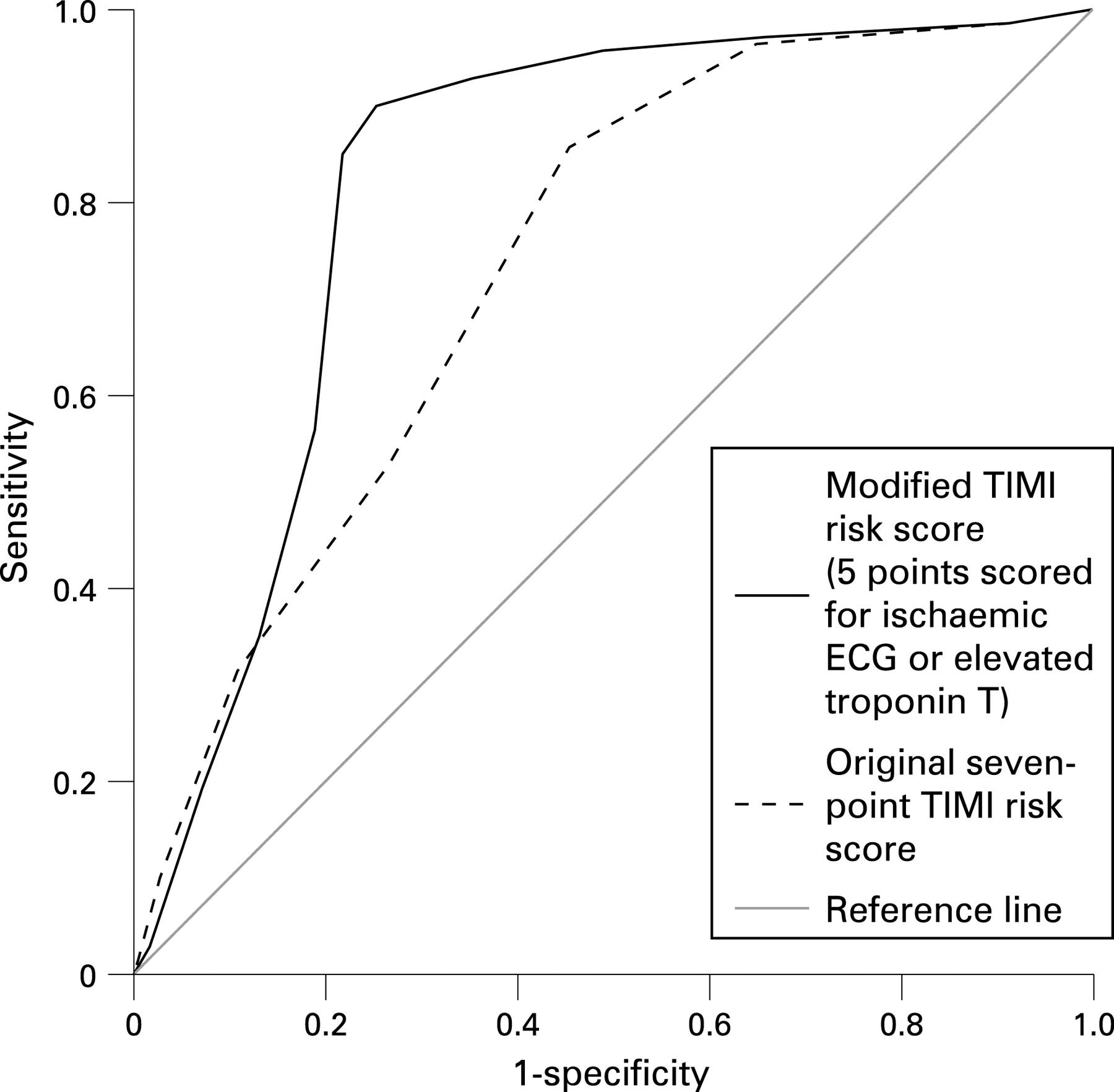
We compared the modified TIMI risk score with the original score using receiver operating characteristic (ROC) curve analysis. Comparative performance was assessed by comparing the areas under the curves (AUC). The optimal cut-offs for the TIMI risk scores were selected by choosing the scores at which sensitivity exceeded 95% with the highest specificity.
RESULTS
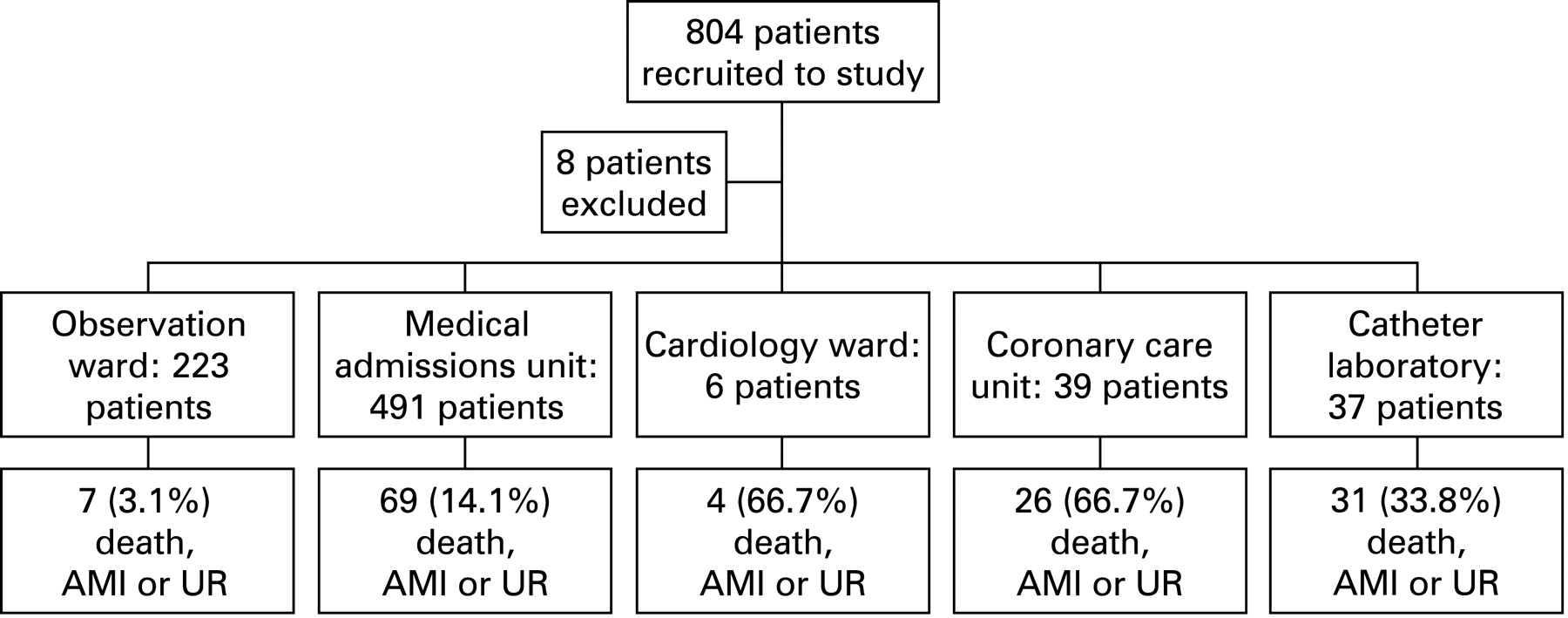
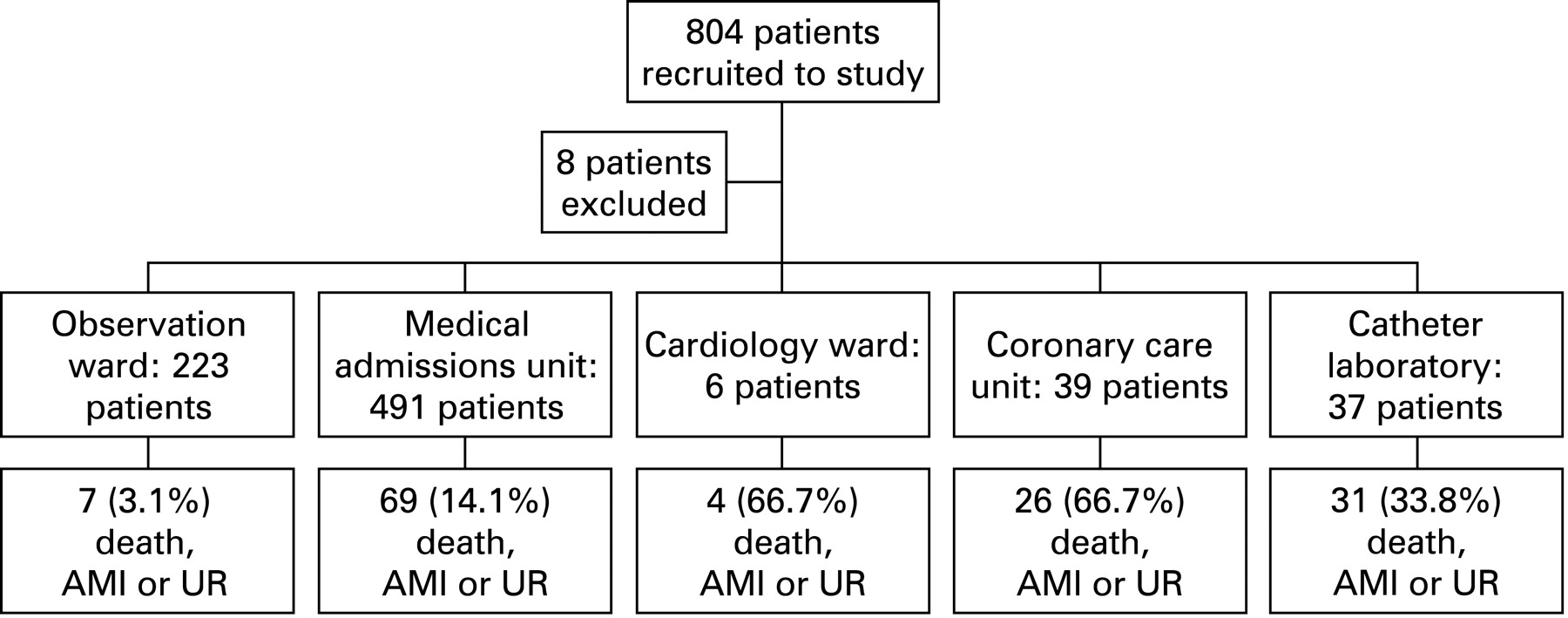
A total of 804 patients was recruited to the study between January 2006 and February 2007. Eight patients were excluded because they were found to meet predefined exclusion criteria. No patients were lost to follow-up; 796 patients were suitable for final analysis. A total of 148 (18.6%) patients had a 12-h troponin level above the diagnostic cut-off for AMI; 226 (28.4%) patients had ischaemic ECG changes; 527 (66.2%) patients had neither AMI nor ischaemic ECG changes. At the 30-day follow-up, death, AMI (excluding the index event) or the need for UR had occurred in 137 (17.2%) patients. Baseline characteristics are shown in table 2.
Table 3 shows the performance of the original and modified TIMI risk scores for prediction of the composite outcome. Figure 1 shows the ROC curves for the original and modified TIMI risk scores. The AUC for the original score was 0.77 (95% CI 0.73 to 0.80) and for the modified score 0.87 (0.85 to 0.90). The difference was statistically significant (p<0.001).
The sensitivities and specificities of the modified TIMI risk score at different cut-offs are shown in table 4. From this table it can be seen that using a cut-off of greater than 0 or greater than 1 carried high sensitivity for the prediction of adverse events but had a poor specificity (<50%), meaning that the majority of “healthy patients” (who would not have developed an event) would need to be admitted to hospital in order to avoid missing those who would have an event. By placing the cut-off at more than 2 points the modified TIMI risk score predicted the composite outcome with a sensitivity of 96.4% (95% CI 91.7% to 98.4%) and a specificity of 51.0% (47.2% to 54.8%). The positive predictive value was 29.0% (25.0% to 33.3%) and the negative predictive value 98.5% (96.6% to 99.4%). Accordingly, for every 1000 patients treated we would project that six patients would be discharged although they would go on to develop an adverse event within 30 days. A total of 422 patients would be admitted to hospital although they would not develop the composite outcome. At higher cut-offs the sensitivity fell below 95%, which would lead to an unacceptably high event rate.
Patient disposition from the ED is shown in fig 2. If we accept that patients who were sent to the observation ward were all felt to be at low risk of adverse events (as per the ED protocol), clinicians had a sensitivity of 94.9% (95% CI 90.0% to 97.5%) and specificity of 33.8% (30.3% to 37.5%) for predicting adverse events. As such, we would project that per 1000 patients treated nine would be discharged although they would go on to develop an adverse event within 30 days. A total of 547 patients would be admitted to hospital although they would not develop an event.
{kind=link}
{kind=link}
DISCUSSION
Our results have validated previous findings that the original TIMI risk score is able to stratify the risk of adverse events within 30 days in ED patients with suspected cardiac chest pain. We have also demonstrated that a modified TIMI risk score with greater weighting given to ischaemic ECG changes and troponin elevations enables superior risk stratification to the original score. The modified score has a high sensitivity and negative predictive value. Patients with a modified TIMI score of less than 3 could be discharged from hospital with a small (1.2%) risk of adverse events.
Some may consider that this is an acceptably low risk and it does compare favourably with the proportion of patients sent to the ED observation ward who developed an event within 30 days (3.1%). The score is still somewhat limited by a lack of specificity, meaning that over 40% of patients would be ineligible for discharge even after 12-h troponin testing. However, if the ED observation ward is utilised to investigate low-risk patients who will be discharged if they prove not to have biomarker elevations, the modified TIMI risk score may help in the selection of these patients provided that appropriate follow-up is provided.
This is the first study to present an evaluation of a modified TIMI risk score in a form that could potentially influence patient disposition. Ischaemic ECG changes and troponin elevations are known independently to identify patients who are at high risk of adverse events in the near future. Using the original TIMI risk score a patient with both of these risk factors could still be identified as “low risk” in the absence of other risk factors. By giving greater weighting to both of these risk factors our modifications prevent this from happening. By evaluating this modified score in the undifferentiated population with suspected cardiac chest pain, all of whom underwent 12-h troponin testing, our cohort is drawn from the precise population for whom the score could be utilised in clinical practice.
Our composite outcome included coronary revascularisation, which is subject to potential bias. Patients who had several cardiac risk factors, ischaemic ECG changes or troponin elevations (and therefore higher TIMI risk scores) are more likely to undergo coronary angiography than patients without those risk factors. These patients may then be more likely to undergo coronary revascularisation procedures as a result. Nonetheless, previous similar research has utilised the same composite outcome.13 15 16 18 24–26 Despite the potential sources of bias the composite outcome is currently the most practical, reliable and objective measure of short-term outcome that we have for this population. Whereas we acknowledge this limitation, it ought not to preclude the drawing of meaningful conclusions from the study.
We reported the sensitivity and specificity of the modified TIMI risk score at all relevant cut-offs but selected an optimal cut-off of greater than 2 points on the basis that this score achieved a sensitivity of over 95% with the highest specificity. Pragmatically, this would appear to be the most appropriate cut-off for making clinical decisions about patients with cardiac chest pain. If the score were to be clinically implemented, further economic and qualitative patient-centred analyses should be undertaken in order that the optimal cut-off is determined in a more robust and scientific manner. Furthermore, because of the possibility that this derivation set overestimates the clinical utility of the modified TIMI risk score, external validation of these findings is warranted before clinical implementation.
The results of this study are consistent with previous reports. Evaluations of the original TIMI risk score in the ED population have demonstrated AUC of 0.74 and 0.79 for predicting short and medium-term adverse events.15 25 A validation study from the USA reported similar event rates in relation to the original TIMI risk score, including a 5.5% incidence of death, AMI and revascularisation by 30 days among patients with a TIMI risk score of 2 or less.24 This compares with a rate of 5.0% from our own cohort.
This previous work suggests that, although the original TIMI risk score enables risk stratification, it cannot be used to influence patient disposition. Our results support that conclusion but add that by pragmatically modifying the TIMI risk score enhanced risk stratification can be achieved. It is possible that patients who score less than 3 using the modified TIMI risk score may be considered for discharge after 12-h troponin testing, but it is still important to appreciate that the risk of adverse events is not zero. Furthermore, as over 40% of patients would be admitted to hospital even after troponin testing, additional risk stratification would still be necessary.
Whereas it would appear that the TIMI risk score does aid in the risk stratification of patients with suspected ACS, it remains unclear how effective it can be in guiding medical decision-making. Our modified TIMI risk score may help to facilitate triage to an ED observation ward or low dependency unit, although it is still compromised by a lack of specificity for guiding further investigation following troponin testing and even low-risk patients had a 1.2% incidence of significant adverse events within 30 days. The holy grail of an early risk stratification tool to rule out ACS therefore remains elusive.
CONCLUSIONS
A modified TIMI risk score that gives greater weight to ischaemic ECG changes and troponin elevations provides superior risk stratification to the original TIMI risk score. The score identifies a low-risk group who may be eligible for discharge after 12-h troponin testing if cautious follow-up arrangements are in place. However, the clinical utility of the score may be limited by a very low specificity. Validation of these findings is warranted.
Acknowledgments
The authors would like to acknowledge the input of Dr Steve Roberts, who was consulted before commencing patient recruitment with regard to statistical analysis. They would also like to acknowledge the assistance given by all of the nursing and medical staff in the ED at Manchester Royal Infirmary.
REFERENCES
Footnotes
Funding: Central Manchester and Manchester Children’s University NHS Trust funded the project. Half of RB’s salary was paid by Manchester Metropolitan University during the study period.
Competing interests: None.
Ethics approval: Ethics approval for the project was obtained from the local research ethics committee, reference 05/Q1410/27.
Patient consent: Obtained.
Contributors: RB had the original idea for this study, designed the study protocol, recruited patients, followed up patients, collated and analysed the data and prepared the manuscript. GMcD, SC and KM-J provided supervision for the project and assisted with the editing of the manuscript. JF assisted with patient recruitment, data collation, study administration and revised the manuscript.
Linked Articles
- Primary survey