Article Text

Abstract
Objective To examine the relative impact of three management options in patients aged <60 years with cryptogenic stroke and a patent foramen ovale (PFO): PFO closure plus antiplatelet therapy, antiplatelet therapy alone and anticoagulation alone.
Design Systematic review and network meta-analysis (NMA) supported by complementary external evidence.
Data sources Medline, EMBASE and Cochrane CENTRAL.
Study selection Randomised controlled trials (RCTs) addressing PFO closure and/or medical therapies in patients with PFO and cryptogenic stroke.
Review methods We conducted an NMA complemented with external evidence and rated certainty of evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) system.
Results Ten RCTs in eight studies proved eligible (n=4416). Seven RCTs (n=3913) addressed PFO closure versus medical therapy. Of these, three (n=1257) addressed PFO closure versus antiplatelet therapy, three (n=2303) addressed PFO closure versus mixed antiplatelet and anticoagulation therapies and one (n=353) addressed PFO closure versus anticoagulation. The remaining three RCTs (n=503) addressed anticoagulant versus antiplatelet therapy. PFO closure versus antiplatelet therapy probably results in substantial reduction in ischaemic stroke recurrence (risk difference per 1000 patients over 5 years (RD): −87, 95% credible interval (CrI) −100 to −33; moderate certainty). Compared with anticoagulation, PFO closure may confer little or no difference in ischaemic stroke recurrence (low certainty) but probably has a lower risk of major bleeding (RD −20, 95% CrI −27 to −2, moderate certainty). Relative to either medical therapy, PFO closure probably increases the risk of persistent atrial fibrillation (RD 18, 95% CI +5 to +56, moderate certainty) and device-related adverse events (RD +36, 95% CI +23 to +50, high certainty). Anticoagulation, compared with antiplatelet therapy, may reduce the risk of ischaemic stroke recurrence (RD −71, 95% CrI −100 to +17, low certainty), but probably increases the risk of major bleeding (RD +12, 95% CrI −5 to +65, moderate certainty).
Conclusions In patients aged <60 years, PFO closure probably confers an important reduction in ischaemic stroke recurrence compared with antiplatelet therapy alone but may make no difference compared with anticoagulation. PFO closure incurs a risk of persistent atrial fibrillation and device-related adverse events. Compared with alternatives, anticoagulation probably increases major bleeding.
PROSPERO registration number CRD42017081567.
- cryptogenic stroke
- patent foramen ovale
- anticoagulation
- antiplatelet
- pfo closure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
Summarised the highest quality available evidence by addressing three management alternatives of patent foramen ovale closure plus antiplatelet therapy, anticoagulation alone and antiplatelet therapy alone.
Used network meta-analysis, meta-regression, external evidence and individual patient analyses from survival curves to assist in decision-making.
Applied GRADE approach to thoroughly assess certainty of evidence.
Results were limited primarily by available evidence.
Within the medical therapy arm, the decision to use antiplatelet or anticoagulation was left to the discretion of the physician and patient.
Due to this, three studies could not be used in the primary analysis.
Introduction
Stroke is one of the leading causes of death worldwide and, for those who survive, often results in substantial disability. Central to the management of patients with stroke is preventing additional ischaemic events; the optimal management depends on the underlying aetiology.
In up to 40% of patients with an acute ischaemic stroke, investigations fail to identify a clear cause—the Trial of Org 10 172 in Acute Stroke Treatment criteria classify these strokes as ‘of undetermined aetiology’ or ‘cryptogenic’.1 Patients who have had a cryptogenic stroke are less likely to have classical risk factors for stroke (eg, hypertension, hyperlipidaemia, diabetes mellitus) and are more likely to have a patent foramen ovale (PFO) compared with patients with a stroke from a known aetiology.2 3
A PFO can allow a systemic venous thrombus to travel directly into the systemic arterial circulation instead of the pulmonary venous circulation—a phenomenon known as a paradoxical embolism.4 5 The importance of this phenomenon as a cause of stroke is, however, controversial. Other potential mechanisms of PFO-associated stroke include intracardiac thrombus formed in the tunnel of the PFO, on the surface of the atrial septal aneurysm or left atrial appendage.5
Until recently, randomised controlled trials (RCTs) had failed to definitively establish that closing a PFO reduces the risk of subsequent stroke.6–8 Meta-analyses including earlier trials offered conflicting conclusions.9–12 Current clinical practice guidelines recommend against PFO closure for most patients who have had a cryptogenic stroke.13
In September 2017, two new trials14 15 and the long-term follow-up of a previously reported trial16 addressed the utility of PFO closure for patients aged <60 years with cryptogenic stroke. Evidence from recent meta-analyses that incorporate data from these RCTs suggests that PFO closure may prevent stroke. However, despite evidence that anticoagulation is more effective than antiplatelet therapy at preventing stasis-related venous or intracardiac thrombi, these meta-analyses make the assumption that antiplatelet and anticoagulation therapies are similarly effective.17
This systematic review is part of the BMJ Rapid Recommendations project, a collaborative effort from the MAGIC research and innovation programme (www.magicproject.org) and the BMJ.18 The aim of the project is to respond to new potentially practice changing evidence and provide trustworthy practice guidelines in a timely manner. In light of the new evidence for PFO closure and because other reviews do not report clinically relevant comparisons (eg, PFO closure vs antiplatelet therapy), we performed a systematic review to inform the parallel guideline published in a multilayered electronic format on bmj.com and MAGICapp (https://www.magicapp.org/goto/guideline/JjXYAL/section/j79pvn).19 As requested by the Rapid Recommendations panel, in the absence of sufficient direct evidence to fully inform recommendations, we conducted complementary analyses using indirect evidence.
Methods
Protocol
The study protocol was registered with PROSPERO: CRD42017081567.20
Patient and public involvement
According to the BMJ Rapid Recommendations process,18 a multiprofessional guideline panel provided critical oversight to the systematic review and identified populations, subgroups and outcomes of interest. The BMJ Rapid Recommendation panel, and in particular three people who had experienced a cryptogenic stroke (two of whom had undergone PFO closure), assessed the relative importance of the outcomes.19 The guideline panel submitted a list of possible outcomes and then rated the importance of each outcome on a scale from 1 (least important) to 9 (most important). For items with scores of 4, the panel considered further and made a final decision by consensus, with special consideration of the views of the patient panellists. The patients stressed the importance of several outcomes that other panel members had identified and uniquely highlighted the importance of detailed information about the device or procedure-related adverse events.
Search strategy
A search from a previous systematic review that we judged as comprehensive included research articles indexed before 1 May 2013.12 We updated that review with a search of Medline, Medline in-process, EMBASE and Cochrane CENTRAL from 1 January 2012 to 15 October 2017 using a combination of keywords and MeSH terms for ‘patent foramen ovale’ AND ‘stroke’, using the sensitive search filters for therapeutic interventions developed by the Health Information Research Unit at McMaster University (see online supplementary appendix 1).21 22 We also searched all references from included studies and all of the studies citing the included studies on Google Scholar.
Supplemental material
Study selection
We included RCTs addressing the relative impact of PFO closure versus antiplatelet therapy versus anticoagulation in patients, and anticoagulation versus antiplatelet therapy with PFO and cryptogenic stroke. We also included prior rigorous systematic reviews addressing antiplatelet versus anticoagulant therapy in patients with deep venous thrombosis, atrial fibrillation and heart failure. Reviewers screened titles and abstracts in duplicate and subsequently assessed eligibility from the full text for all possible eligible articles. In comparing PFO closure with antiplatelet therapy for the outcome of stroke, we used only RCTs in which at least 80% of medical therapy patients received antiplatelet rather than anticoagulation.
Data collection
Two reviewers independently abstracted data from the included RCTs and resolved conflicts by discussion. We searched the clinical trial registration page on clinicaltrials.gov for additional outcome data and emailed the corresponding authors of the included RCTs requesting outcome data when it was missing or could not, as presented in the public domain, be included in meta-analytic estimates.
The patient-important outcomes we considered included ischaemic stroke, death, major bleeding, persistent atrial fibrillation or flutter, transient or paroxysmal atrial fibrillation, device or procedure related adverse events, pulmonary embolism, transient ischaemic attacks (TIAs) and systemic embolism. For serious device or procedure-related complications, two independent clinician reviewers categorised the specific serious adverse events in the primary studies as probably related or unrelated to the device or implantation procedure; reviewers resolved disagreement with, if necessary, input from a third reviewer. We used the definitions in the original studies for all outcomes except for persistent atrial fibrillation; our classification included the definition used in the original study and included patients who underwent a cardioversion. We also abstracted key outcomes from the external evidence systematic reviews.
Risk of bias and certainty of evidence
We assessed risk of bias in duplicate using a modified Cochrane tool in which we used response options of ‘definitely or probably yes’ (assigned a low risk of bias) and ‘definitely or probably no’ (assigned a high risk of bias), an approach that has proved valid.23 24 Specifically, we assessed random sequence generation; concealment of treatment allocation and blinding of participants, caregivers and outcome assessors. Reviewers resolved conflicts through discussion.
We followed the GRADE approach to rate the quality of evidence derived from pairwise and network meta-analyses (NMA) as well as from external evidence.25 26 Direct evidence from RCTs starts at high quality and may be rated down based on risk of bias, indirectness, imprecision, inconsistency and publication bias. For network estimates, we rated the quality of evidence in each of the direct, indirect and network estimates.26 The rating of indirect estimates starts at the lowest rating of the two pairwise estimates that contribute to the indirect estimate and can be rated down further for intransitivity. If direct and indirect estimates contributed similar power to the network estimate, then we used the higher rating. The network estimates were further rated down for incoherence between direct and indirect evidence. For analyses that incorporated external evidence, we rated down the quality of evidence for indirectness (down one level for major bleeding and two levels for ischaemic stroke).27 Review authors and the linked Rapid Recommendation panel members came to consensus regarding certainty of evidence ratings.
Statistical analysis
We analysed patients in groups to which they were randomised. For both pairwise and NMA, we report pooled ORs; for estimates from NMA we report 95% credible intervals (CrI) from the Bayesian analysis and for direct estimates 95% CI. We present pooled risk differences (RD) and their certainty/CIs for all comparisons, applying relative risks to baseline risk estimates when there were adequate numbers of events, and direct calculation of risk differences when events were very infrequent. In reporting absolute events, we standardised absolute estimates to a rate per 1000 patients followed for 5 years assuming proportional event occurrence (in other words, for a reported follow-up of 3 years we would multiply by 5/3). Atrial fibrillation and device or procedure-related adverse events were, however, very likely to have occurred soon after the procedure and we therefore report events per 1000 patients as reported in the studies.
The PFO closure arm was used for the baseline risk to allow consistency across comparisons involving PFO closure versus antiplatelet agents and anticoagulants. Baseline risk estimates represent the median risk of the outcome in the six RCTs of PFO closure. For comparisons of antiplatelet agents and anticoagulants, the antiplatelet arm provided the baseline risk to estimate the absolute effect estimate in the anticoagulation arm. The baseline risk for the antiplatelet arm (10%) was calculated using the baseline risk in the PFO closure arm. This proved similar to the median of three studies that included an antiplatelet arm (9%) and maintained consistency with the PFO closure comparisons.
Network meta-analysis
To compare effects of alternative medical therapies, for ischaemic stroke, recurrent TIA, death, major bleeding and systemic embolism, we conducted an NMA of RCTs within a Bayesian hierarchical fixed effect framework with non-informative priors and adjusted for correlation between effects in the multiarm trial. We generated posterior samples using Markov Chain Monte-Carlo simulation technique running the analysis in three parallel chains. We used 100 000 burn-in simulations to allow convergence and then a further 500 000 simulations to produce the outputs. We assessed model convergence using the Gelman and Rubin test, accepting a threshold of <1.05 and used the node-splitting approach for the assessment of loop inconsistency.28 29 We calculated direct estimates of absolute effects using the modified Dias model, incorporating lines into the Dias model.30 We performed the NMAs with R V.3.4.1 (R Core Team, 2016, Vienna, Austria: R Foundation for Statistical Computing) using the gemtc library.31
Pairwise meta-analysis
As there is no reason, for the outcomes of atrial fibrillation and device or procedure-related adverse events, to expect any difference whether PFO closure is compared with anticoagulation or antiplatelet therapy, for these outcomes we conducted a pairwise meta-analysis of PFO closure versus either medical therapy. We used the random-effects Mantel-Haenszel (M-H) method to estimate relative risk (RRs) and 95% CIs, using the M-H risk difference approach for studies that did not have any events in either arm. For outcomes with event rates <1%, we used the Peto fixed effects method to estimate OR and 95% CI. For all outcomes, we examined statistical heterogeneity among studies using the I2 statistic and visual inspection of the forest plots.27
Meta-regression analysis
We hypothesised that anticoagulation may be more effective than antiplatelet therapy for preventing stroke. Thus, we expected that the effect of PFO closure versus medical therapy would be largest in the RCTs that had proportionally more patients in the medical therapy group that were treated with antiplatelet therapy rather than anticoagulation. To explore this, we performed a random-effects meta-regression of PFO closure versus medical therapy, with the proportion of patients in the medical therapy arm who received anticoagulation as the independent variable. We used random-effects meta-regression with the studies were weighed by the inverse of their variance.
Modelling with external data from other indications
Because few patients were randomised to PFO closure versus anticoagulation (n=353) or anticoagulation versus antiplatelet agents (n=405) and events were infrequent, the estimates of effect of PFO closure versus anticoagulation were extremely imprecise. For instance, for ischaemic stroke the CrI around the relative effect included a relative reduction in events of 90% to a more than quadrupling of events (NMA OR 0.51, 95% CrI 0.09 to 4.46). We considered this information essentially uninformative, as did the Rapid Recommendations panel. We nevertheless considered the option of anticoagulation crucial to the decision, and therefore sought strategies for more informative estimates of effect.
For ischaemic stroke, the most likely mechanism of cryptogenic stroke associated with PFO is stasis-related thrombi, most notably paradoxical venous thromboembolism (VTE). The panel and systematic review team therefore deduced that the relative effects of anticoagulation versus antiplatelet therapy in the secondary prevention of VTE could provide credible estimates of effect for patients with cryptogenic stroke and PFO. For major bleeding, we deduced that the relative effects of vitamin K antagonist (VKA) anticoagulation and low-dose Acetylsalicylic acid (ASA) are similar to those seen in other common indications including VTE, heart failure and atrial fibrillation and could therefore provide credible estimates of relative bleeding risk of antiplatelet agents (with or without PFO) and anticoagulants.
Thus, the panel and systematic review team ultimately decided to use this evidence to provide indirect evidence of estimates of effect for three key outcomes (ischaemic stroke, major bleeding and pulmonary embolism). We therefore performed a secondary analysis that also included RCT evidence from other conditions (VTE, heart failure and atrial fibrillation).
For ischaemic stroke, we digitised Kaplan-Meier curves and extracted patient-level time-to-event data.32 For illustrative purposes, we present the individual patient data by treatment arm (PFO closure plus antiplatelet therapy, antiplatelet therapy alone, anticoagulation and medical therapy left to the discretion of the treating physician). Each enrolled patient contributed equally to the survival curves.
Subgroup analysis
We planned subgroup analyses based on the echocardiography-determined shunt size and the presence of an atrial septal aneurysm. We hypothesised that patients with a larger shunt size will have a larger benefit with PFO closure than patients with a small shunt size and that patients with an atrial septal aneurysm will have a larger benefit with PFO closure than patients without an atrial septal aneurysm.33
Results
Our systematic literature search yielded 772 potentially relevant publications; 10 trials presented in 8 reports ultimately proved eligible (figure 1, online supplementary appendix 2: eTable1).6 8 14–16 34–36 Seven eligible multicentre RCTs published in 2013 or later comparing PFO closure plus antiplatelet therapy versus medical therapy enrolled 3913 patients (range per RCT: 120–980 patients) (table 1). The Patent Foramen Ovale Closure or Anticoagulants versus Antiplatelet Therapy to Prevent Stroke Recurrence (CLOSE) trial included three separate randomised trials.14 In the first trial, patients eligible for all options were randomised to PFO closure (n=173), antiplatelet therapy (n=171) or anticoagulation with a VKA or direct oral anticoagulant (n=180; 93% of which were a VKA). In the second trial, patient’s ineligible for anticoagulation were randomised to PFO closure (n=65) or antiplatelet therapy (n=64). In the third trial, patients with contraindications to PFO closure were randomised to antiplatelet therapy (n=7) or anticoagulation (n=3). Of the remaining eligible RCTs, one specified that all patients in the group who were not randomised to PFO closure were treated with antiplatelet therapy (n=664).15 Four RCTs allowed the treating physician to choose between antiplatelet and/or anticoagulation therapy for the patients randomised to medical therapy: a minority of these patients (range 20%–34%) were prescribed anticoagulation at the time of discharge from initial hospital admission.6 8 16 36 The last three studies compared antiplatelet therapy with anticoagulation (n=503).14 34 35 One study reported a composite end point for ischaemic stroke and TIA; we therefore could not use the data in our meta-analyses of stroke (n=44).34 However, we were able to use data from this RCT in analyses of death and major bleeding. Another RCT reported only a composite outcome of stroke and death (n=98),35 with non-significant results suggesting a possible reduction with anticoagulation compared with antiplatelet therapy (HR 0.52, 95% CI 0.16 to 1.67, p=0.28).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of studies included in review treatment of patients with patent foramen ovale and cryptogenic stroke.
Characteristics of patients in eligible studies
There is risk of bias in most studies due to a lack of blinding of medical personnel or patients regarding the placement of a PFO closure device (see online supplementary appendix 3: eFigure 1). Also, half of the studies had incomplete data; we contacted the authors of three RCTs for additional outcome data.14 34 35 The lead author of the CLOSE study (J-LM) provided additional unpublished data; however, the authors of the two remaining studies did not respond.
We identified a recent rigorous systematic review of 12 trials and 11 999 participants for secondary prevention of VTE17 and a recent rigorous systematic review of 15 trials and 4982 participants across indications that provided a trustworthy estimate for an increase in major bleeds37; both reviews compared anticoagulant with antiplatelet therapy.
Table 1 presents the characteristics of the eligible studies. In most, the mean age was approximately 45 years, approximately 50%–60% were male, and approximately 50%, or more, had moderate or larger shunt. The median follow-up was 3.9 years with a range of 1.2–5.9 years.
PFO closure plus antiplatelet therapy versus antiplatelet therapy alone
Table 2 provides estimates of effect and certainty of evidence for all patient-important outcomes, including, as presented subsequently, complications of PFO closure. PFO closure plus antiplatelet therapy reduced the risk of ischaemic stroke compared with antiplatelet therapy alone (NMA OR 0.12, 95% CrI 0.04 to 0.27; risk difference per 1000 patient-years followed for 5 years (RD): −87, 95% CrI −100 to −33; moderate certainty) (see online supplementary appendix 4: eFigure 1).
GRADE summary of findings of PFO closure plus antiplatelet therapy vs antiplatelet therapy alone in patients with cryptogenic stroke
Summary of GRADE evidence profile of PFO closure plus antiplatelet therapy vs anticoagulation in patients with cryptogenic stroke
Summary of GRADE evidence profile of anticoagulation vs antiplatelet therapy alone in patients with cryptogenic stroke
Along with the three RCTs in which all medical patients received only antiplatelet therapy,14 15 36 we included a meta-regression model data from an additional five RCTs that enrolled patients in which >20% of medically treated patients received anticoagulation (Figure 2).6 8 14 16 The reduction in stroke with PFO closure decreased as the proportion of patients receiving anticoagulation in the medical therapy arm increased (p=0.036).

Meta-regression curve based on the proportion of anticoagulant in the medical therapy arm for ischaemic stroke.
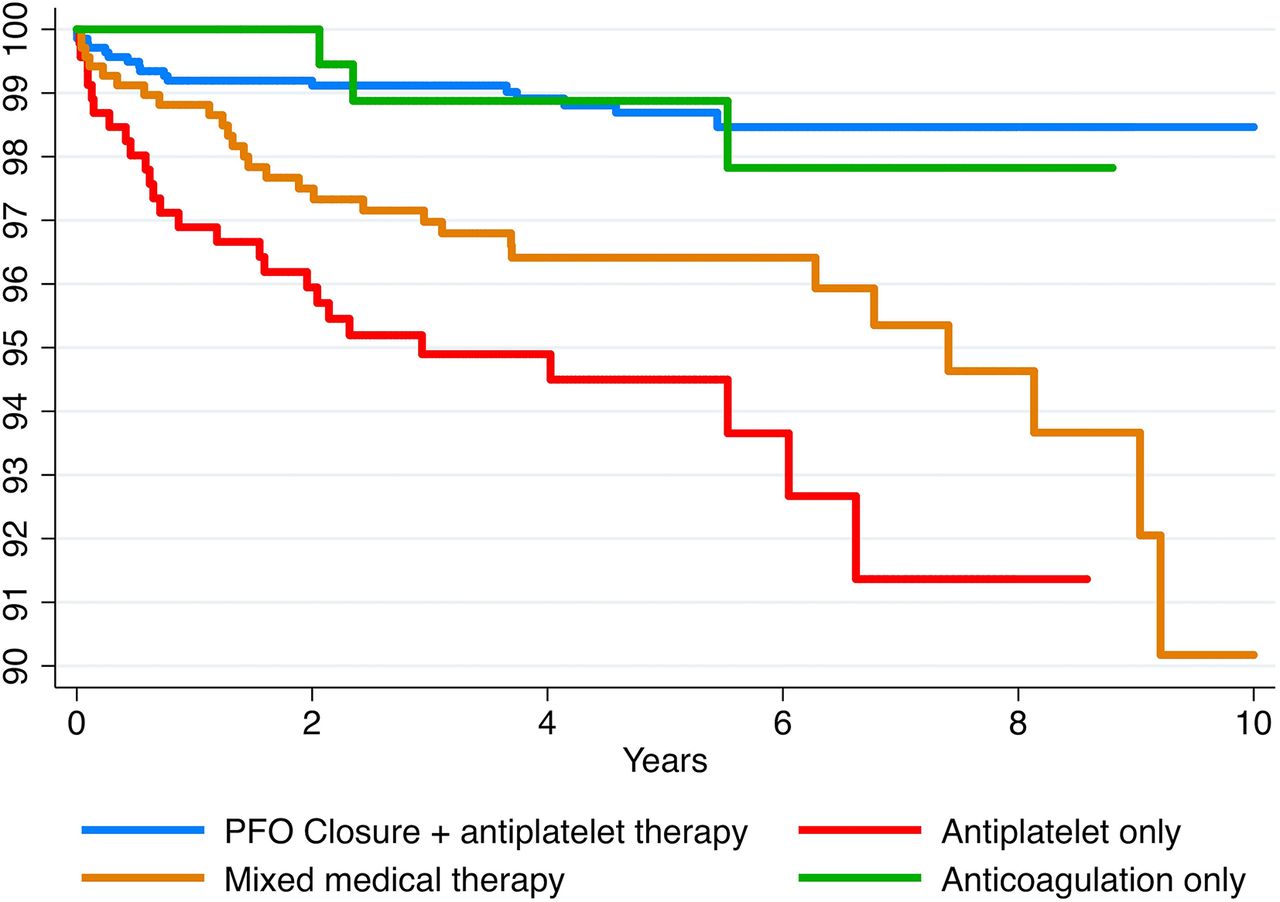
Figure 3 presents a Kaplan-Meier curve of individual patient time-to-event data for each of the randomised interventions, including PFO closure plus antiplatelet versus antiplatelet therapy alone and is again consistent with large relative reductions in hazard with PFO closure versus antiplatelet therapy and smaller benefits of PFO closure when compared with mixed populations of patients receiving anticoagulants and antiplatelet agents.

{kind=link}
{kind=link}
{kind=link}
Combined Kaplan-Meier curves with individualised patient data based on the type of intervention for ischaemic stroke. (1) Y-axis is truncated from 90% to 100% event-free survival. (2) Mixed medical therapy includes studies where the proportion of antiplatelet agents was <80% and the proportion of anticoagulant was >25%. (3) Proportion of patients: patent foramen ovale (PFO) closure+antiplatelet therapy (n=1829; 50%), mixed medical therapy (n=1153; 32%), antiplatelet therapy (n=458; 13%) and anticoagulation (n=210; 6%). (4) Kaplan-Meier curves were available for the outcome of ischaemic stroke in the CLOSE study14 (PFO closure, anticoagulation and antiplatelet), the PC Trial6 (PFO closure and mixed medical therapy), the RESPECT trial16 (PFO closure and mixed medical therapy) and the REDUCE trial15 (PFO closure and antiplatelet).
PFO closure did not appear to reduce the risk of TIA compared with antiplatelet therapy alone: NMA OR 0.82, 95% CrI 0.32 to 2.11; RD −6, 95% CrI –34 to +15; moderate certainty (table 2, online supplementary appendix 4: eFigure 2).
Systemic emboli were rare: there were five events in one study,15 and none in another14; we therefore calculated the risk difference directly. There was no important difference between PFO closure and antiplatelet therapy: NMA OR 0.83, 95% CrI 0.12 to 7.25; RD −1, 95% CrI –6 to +4 per 1000 patients; high certainty (table 2, online supplementary appendix 4: eFigure 3).
Death occurred infrequently: in the PFO closure group a median of 9 per 1000 patients died over a period of 5 years. The relative effect estimate for mortality was very imprecise, and the absolute estimates included a small increase or decrease in deaths: NMA OR 3.28, 95% CrI 0.2 to 174.22; RD +6, 95% CrI −3 to +9; moderate certainty (table 2, online supplementary appendix 4: eFigure 4).
The risk of major bleeding did not differ significantly between the PFO closure plus antiplatelet therapy and antiplatelet therapy alone groups: NMA OR 0.48, 95% CrI 0.20 to 1.12; RD −7, 95% CrI −14 to +1, moderate certainty (table 2, online supplementary appendix 4: eFigure 5). Pulmonary embolism was rare and no more frequent in the PFO closure group (3/679, 0.4%) than the antiplatelet therapy alone group (1/458, 0.2%). No additional NMA evidence was available for pulmonary embolism because none of the RCTs that included an anticoagulation arm reported pulmonary emboli; thus, we present a pairwise estimate for PFO closure versus antiplatelet therapy alone: Peto OR 1.01, 95% CI 0.09 to 11.21; RD +0, 95% CI −5 to +48, high certainty (table 2, online supplementary appendix 4: eFigure 6).
PFO closure plus antiplatelet therapy versus anticoagulation
Table 3 provides estimates of effect and quality of evidence for all patient-important outcomes including, as presented below, complications of PFO closure. One RCT randomised patients to PFO closure plus antiplatelet therapy (n=173) or anticoagulation (n=180).14 In the NMA, compared with anticoagulation, PFO closure did not significantly reduce the risk of ischaemic stroke, but the CrI around the relative effect was very wide (NMA OR 0.44, 95% CrI 0.08 to 3.83; RD −16, 95% CrI −29 to +10; low certainty). Figure 3 presents a Kaplan-Meier curve of individual patient time-to-event data for each of the randomised interventions, including PFO closure plus antiplatelet versus anticoagulation alone.
Results from the meta-regression analysis described previously suggest that PFO closure was less effective relative to medical therapy as the proportion of patients receiving anticoagulation increased (figure 2).
To complement the above analyses, we added the effect estimate from a systematic review of RCTs comparing low-dose ASA with anticoagulation with a VKA for the secondary prevention of VTE to the NMA.17 Similar to the primary analysis, the analysis with the external evidence failed to show a difference between PFO closure and anticoagulation for ischaemic stroke, with a point estimate substantially closer to 1.0: NMA OR 0.93, 95% CrI 0.31 to 2.76; RD −2, 95% CrI –20 to +47; low certainty (table 3, online supplementary appendix 5: eFigure 1). For this complementary analysis, we rated down our certainty in the evidence to low because of very serious indirectness because this analysis relies on the assumption that the relative effect of anticoagulation versus antiplatelet therapy is the same for secondary prevention VTE as it is for secondary prevention of cryptogenic stroke in patients with a PFO.
There was no important difference in TIA: NMA OR 1.27, 95% CrI 0.40 to 4.52; RD+ 6, 95% CrI −22 to +22; moderate certainty (table 3, online supplementary appendix 5: eFigure 2). No patient experienced a systemic embolism in either arm of the RCT that included an anticoagulation arm (see online supplementary appendix 5: eFigure 3).
Few patients randomised to PFO closure plus antiplatelet therapy experienced a pulmonary embolism (median risk 5 per 1000 patients over 5 years). The RCT that randomised patients to PFO closure versus anticoagulation did not measure pulmonary emboli.14 Using external evidence from a systematic review of RCTs that compared ASA with anticoagulation with a VKA for secondary prevention of VTE in the NMA, PFO closure plus antiplatelet therapy probably has a higher risk of pulmonary embolism than anticoagulation: RD +4, 95% CI +1 to +13; moderate certainty (table 3, online supplementary appendix 5: eFigure 4).
Patients randomised to PFO closure plus antiplatelet therapy had a lower risk of major bleeding than those randomised to anticoagulation: NMA OR 0.26, 95% CrI 0.07 to 0.82; RD −20, 95% CrI −27 to −2, moderate certainty (table 3, online supplementary appendix 5: eFigure 5). Adding the effect estimate for major bleeding of low-dose ASA compared with anticoagulation with a VKA from a systematic review of RCTs enrolling patients with atrial fibrillation, VTE or heart failure37 to the NMA, resulted in an almost identical point estimate, but a narrower CI: OR 0.28, 95% CrI 0.13 to 0.55; RD −17, 95% CrI −21 to −11; moderate certainty (table 3).
There was no difference in death between PFO closure and anticoagulation (OR 0.69, 95% CrI 0.02 to 32.36 ; RD −4, 95% CI –13 to +9, moderate certainty) (table 3).
Complications of PFO closure
PFO closure, when compared with medical therapy, probably substantially increases the risk of atrial fibrillation (including transient, persistent and paroxysmal): six RCTs with 3560 patients; RR 4.50, 95% CI 2.35 to 8.60; RD per 1000 patients +39, 95% CI +15 to +84; moderate certainty (table 3, online supplementary appendix 6: eFigure 1). All six studies assessed persistent atrial fibrillation at a follow-up of 2.0–5.9 years. PFO closure probably increases the risk of persistent atrial fibrillation: RR 4.84, 95% CI 1.91 to 12.26; RD +18, 95% CI +5 to +56; moderate certainty (table 3, online supplementary appendix 6: eFigure 2). PFO closure also probably increases the risk of transient atrial fibrillation: RR 3.76, 95% CI 1.74 to 8.10; RD +12, 95% CI +3 to +31; moderate certainty (table 3, online supplementary appendix 6: eFigure 3). The studies were limited by risk of bias because they did not report sufficient detail to know how persistent atrial fibrillation was detected (tables 2 and 3).
Serious device or procedure-related adverse events occurred in approximately 36 per 1000 patients, 95% CI 23 to 50, high certainty (table 2, online supplementary appendix 6: eFigure 4). The most common device or procedure-related complications were vascular complications (1%), conduction abnormalities (1%), device dislocation (0.7%) and device thrombosis (0.5%). Although serious, air embolism (0.4%), cardiac tamponade (0.3%) and cardiac perforation (0.2%) were rare (tables 2 and 3). No deaths were attributed to the procedure or the device placement (tables 2 and 3).
Anticoagulation versus antiplatelet therapy
Table 4 provides estimates of effect and certainty of evidence for all patient-important outcomes comparing the two medical therapies. There may be fewer ischaemic strokes in patients randomised to anticoagulation than to antiplatelet therapy, but the CI included no effect: NMA OR 0.27, 95% CrI 0.03 to 1.21; RD −71, 95% CrI −100 to +17; low certainty (table 4, online supplementary appendix 7: eFigure 1). Figure 3 presents a Kaplan-Meier curve of individual patient time-to-event data for each of the randomised interventions, including anticoagulation versus antiplatelet therapy suggesting a lower rate of stroke in patients receiving anticoagulant than antiplatelet therapy.
The complementary model including external evidence from a systematic of RCTs comparing low-dose ASA with anticoagulation with a VKA for secondary prevention of VTE yielded a somewhat larger reduction in strokes with anticoagulants and substantially narrowed the CI: OR 0.17, 95% CrI 0.08 to 0.36; RD −81, 95% CrI −91 to −62; low certainty (table 4).37
There may be little or no difference in risk of TIA between anticoagulation and antiplatelet therapy (NMA OR 0.65, 95% CrI 0.19 to 1.98; RD −12, 95% CrI −34 to +24; low certainty (table 4, online supplementary appendix 7: eFigure 2). There were no reported systemic emboli, although it is not clear what the monitoring and ascertainment processes were.
Our analysis suggested more major bleeding events among patients randomised to anticoagulation than to antiplatelet therapy, but the CI included no effect: NMA OR 1.90, 95% CrI 0.68 to 5.53; RD +12, 95% CrI –5 to +65; moderate certainty (table 4, online supplementary appendix 7: eFigure 3). Including external evidence from a systematic review of RCTs comparing low-dose ASA with anticoagulation with a VKA in patients with atrial fibrillation, VTE and heart failure yielded a very similar point estimate and substantially narrowed the CI: OR 1.77, 95% CI 1.36 to 2.31; RD +11, 95% CI +5 to +18; moderate certainty (table 4).37
The RCT that included an anticoagulation arm did not report pulmonary emboli; the risk of pulmonary embolism was low in other RCTs that included an antiplatelet arm (median 5 per 1000 patient-years over 5 years). External evidence from a systematic review of secondary prevention of VTE suggests that the risk of pulmonary embolism is probably lower with anticoagulation than antiplatelet therapy: RD −4, 95% CI −5 to −3; moderate certainty.17
Deaths were extremely rare and there was no appreciable difference between the anticoagulation and antiplatelet therapy: RD +10, 9% CI −3 to +357, low certainty (table 4, online supplementary appendix 7: eFigure 4).
Subgroup analyses
Data proved insufficient to perform the prespecified subgroup analyses when anticoagulation and antiplatelets were assumed to have different effects, as we had prespecified. We performed one post hoc meta-regression analysis to explore the effect of PFO shunt size on the relative effectiveness of PFO closure compared with medical therapy. Five RCTs reported ischaemic stroke and the proportion of patients with a moderate or large shunt versus small shunt, all with slightly different definitions. PFO closure was more effective in the RCTs that enrolled a higher proportion of patients with a moderate or large shunt (interaction p=0.047) (see online supplementary appendix 8: eFigure 1). However, this is confounded by the fact that the RCTs that enrolled a higher proportion of patients with moderate or large PFO shunts also had a larger proportion of patients with antiplatelet agents rather than anticoagulation (see online supplementary appendix 8: eFigure 2). When both possible effect modifiers were included in the model neither was statistically significant: p=0.44 for proportion with moderate or large shunt and p=0.61 for proportion receiving anticoagulation; however, this model is severely underpowered with two effect modifiers and only five studies.
Discussion
We found moderate certainty evidence that in patients aged <60 years with a PFO and cryptogenic stroke, PFO closure plus antiplatelet therapy results in a substantial reduction in the risk of recurrent ischaemic stroke compared with antiplatelet therapy alone by approximately 8.7% over 5 years, but increases the risk of persistent atrial fibrillation (approximately 1.8%) and device-related adverse events (approximately 3.6%) in the first year after procedure (table 2).
Although the evidence regarding anticoagulation versus alternatives is of low quality and comes in large part from indirect evidence, it is possible that anticoagulation and PFO closure may achieve a similar reduction in the risk of recurrent ischaemic stroke—and thus appreciably fewer strokes than antiplatelet agents alone. Anticoagulation, compared with either PFO closure plus antiplatelet therapy or antiplatelet therapy alone probably increases the risk of major bleeding by approximately 2% over 5 years and probably reduces the risk of pulmonary embolism by approximately 0.4%. There does not appear to be an important difference in the risk of death or in the risk of systemic emboli between any of the interventions.
Our results provide further strong support for the hypothesis that stasis-related paradoxical venous thromboemboli and/or intracardiac thrombi cause a large proportion of cryptogenic strokes in younger patients with PFO. Given that is the case, it is plausible, although uncertain, that anticoagulation has a similar relative benefit versus antiplatelet agents in preventing cryptogenic strokes in patients with PFO as it does in preventing recurrent VTE. Our results, including the meta-regression examining comparisons of PFO closure versus studies in which varying proportion of patients received anticoagulants (figure 2) support this inference.
Only one of the RCTs included an arm in which all patients were offered anticoagulation or PFO closure; as a result, the direct evidence includes relatively few patients and very few events. Moreover, the evidence from studies of VTE is very indirect. Thus, we categorised the evidence regarding anticoagulation versus PFO closure, and versus antiplatelet therapy, in preventing stroke as low certainty (tables 3 and 4). Resolving the uncertainty that currently bedevils decision-making will require larger RCTs that compare anticoagulation with PFO closure.
A recent systematic review suggested that PFO closure may be more effective in patients with larger shunt.38 We show that this subgroup analysis has low credibility because it is confounded by the anticoagulation in the patients randomised to medical therapy in RCTs with a higher proportion of patients with smaller shunts. PFO closure may be less effective relative to medical therapy when patients receive anticoagulation and/or have smaller shunts. The results of the NMA, in addition to indirect evidence from patients with a VTE, suggest that the subgroup effect by type of medical therapy may be the most credible explanation.
PFO closure comes with infrequent but important risks: an approximately 3%–4% chance of serious device or procedure-related complications and an approximately 4% increased incidence of atrial fibrillation, of which approximately half is persistent. Anticoagulation with VKAs carries a 1%–2% increase in major bleeding over 5 years in this patient population. The risk of major bleeding may be marginally lower with some direct-acting oral anticoagulants than with VKAs.17 Patients must also consider the important practical implications of taking anticoagulants, including limitations to diet and activities with an appreciable risk of trauma, possible drug interactions and, with VKAs, the need for repeat laboratory testing.
Strengths and limitations
Our study has several strengths. In contrast with recent systematic reviews summarising the recent RCTs on PFO closure,38–41 we separately addressed the three management alternatives of PFO closure plus antiplatelet therapy, anticoagulation alone and antiplatelet therapy alone. In doing so, we applied several analytical approaches, including NMA, meta-regression and individual patient analyses from survival curves, as well as judicious use of external evidence, to bring to bear all the relevant evidence for decision-making. In addition, we used the GRADE approach to assess the certainty of evidence informing the estimates in the study. Our review also includes one recently published study not included in prior reviews. We thus summarised all of the highest quality available evidence, providing optimal insight into the comparative effects of the alternative management strategies for patients with PFO who have experienced a cryptogenic stroke.
The results are limited primarily by the available evidence. Of the 10 RCTs that we included in this review, 3 compared PFO closure with a medical therapy arm that was not predefined—the key choice between antiplatelet and anticoagulation was left to the discretion of the physician and patient. As corroborated in our evidence synthesis, there are probably important differences between anticoagulation and antiplatelet therapy. As a result, these three RCTs cannot directly inform the clinical decisions in which antiplatelet therapy and anticoagulation are two distinct choices, and we could not include them in many of the analyses bearing on the choice between PFO closure and antiplatelet therapy. Our meta-regression analysis that included these studies suggested an inverse relationship between stroke reduction and proportion of patients in the medical therapy arms prescribed anticoagulation, thus providing support for the benefit of anticoagulants versus antiplatelet therapy (figure 2).
The NMA also has limitations: the network is sparsely populated (see online supplementary appendix 8: eFigure 3), it includes patients with no contraindications to any of three management strategies, those with patients with contraindications to anticoagulants, and those with contraindications to PFO. Nevertheless, we found no suggestion of incoherence between direct and indirect estimates in the NMA and suggest that it provides the best estimates available (see online supplementary appendix 9, eTable 1).
The applicability of these findings to older patient populations, particularly those over 60 years of age, and those with traditional cerebrovascular risk factors such as exposure to diabetes, hypertension and hyperlipidaemia, is uncertain. The proportion of patients with a cryptogenic stroke caused by paradoxical emboli rather than large vessel atheroembolism or intracardiac thrombus almost certainly decreases with age. Thus, we expect that the benefits of PFO closure would be smaller in older patients and the harms (eg, atrial fibrillation) greater.
Conclusions
In patients aged <60 years with cryptogenic stroke and a PFO, PFO closure plus antiplatelet therapy probably confers a substantial reduction in the risk of ischaemic stroke recurrence compared with antiplatelet therapy alone, with a modest risk of persistent atrial fibrillation or flutter and serious device or procedure-related complications. Based on low certainty evidence, anticoagulation may confer a similar reduction in the risk of ischaemic stroke compared with PFO closure, but likely confers a modest increased risk of major bleeding. Future RCTs comparing anticoagulation with PFO closure would substantially reduce uncertainty for several critical outcomes.
Acknowledgments
The authors would like to thank members of the BMJ Rapid Recommendations panel for critical feedback on outcome selection, subgroup selection, GRADE judgements and manuscript feedback. The authors would also like to thank Rachel Couban for helping develop the search strategy.
References
Footnotes
Contributors GHG and RACS conceived the study idea. HM performed the literature search and data analysis. HM, RACS, TA, GHG, POV interpreted the data analysis. HM, RACS and GHG wrote the first draft of the manuscript. TS, LL and MF acquired data and judged risk of bias in the studies. FF extracted patient level survival data from Kaplan-Meier curves. LG provided statistical advice. RACS, GHG, TA, POV, TK, J-LM and MF critically reviewed the manuscript. HM had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. HM is guarantor.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer The lead author (HM) affirms that the manuscript is an honest, accurate and transparent account of the study being reported; that no important aspects of the study have been omitted and that any discrepancies from the study as planned have been explained.
Competing interests All authors have completed the BMJ Rapid Recommendations disclosure form, which asks about any possible financial, intellectual and professional conflicts of interest (available on request). To summarise, J-LM has received consulting honoraria from Bayer, Bristol-Myers Squibb, Boehringer-Ingelheim, Daiichi Sankyo, GECKO and Servier. HM, RACS, TK, PV, TA and GHG are also panel members of the linked Rapid Recommendation guideline panel.
Patient consent Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi: 10.5061/dryad.ng017rc