Article Text

Abstract
Objectives To investigate the relationship between multimorbidity and healthcare utilisation patterns among the highest cost patients in a large, integrated healthcare system.
Design In this retrospective cross-sectional study of all patients in the U.S. Veterans Affairs (VA) Health Care System, we aggregated costs of individuals’ outpatient and inpatient care, pharmacy services and VA-sponsored contract care received in 2010. We assessed chronic condition prevalence, multimorbidity as measured by comorbidity count, and multisystem multimorbidity (number of body systems affected by chronic conditions) among the 5% highest cost patients. Using multivariate regression, we examined the association between multimorbidity and healthcare utilisation and costs, adjusting for age, sex, race/ethnicity, marital status, homelessness and health insurance status.
Setting USA VA Health Care System.
Participants 5.2 million VA patients.
Measures Annual total costs; absolute and share of costs generated through outpatient, inpatient, pharmacy and VA-sponsored contract care; number of visits to primary, specialty and mental healthcare; number of emergency department visits and hospitalisations.
Results The 5% highest cost patients (n=261 699) accounted for 47% of total VA costs. Approximately two-thirds of these patients had chronic conditions affecting ≥3 body systems. Patients with cancer and schizophrenia were less likely to have documented comorbid conditions than other high-cost patients. Multimorbidity was generally associated with greater outpatient and inpatient utilisation. However, increased multisystem multimorbidity was associated with a higher outpatient share of total costs (1.6 percentage points per affected body system, p<0.01) but a lower inpatient share of total costs (−0.6 percentage points per affected body system, p<0.01).
Conclusions Multisystem multimorbidity is common among high-cost VA patients. While some patients might benefit from disease-specific programmes, for most patients with multimorbidity there is a need for interventions that coordinate and maximise efficiency of outpatient services across multiple conditions.
- GERIATRIC MEDICINE
- HEALTH SERVICES ADMINISTRATION & MANAGEMENT
- PRIMARY CARE
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study describes rates of 33 chronic conditions and condition combinations, and associated utilisation and cost patterns, among the 5% highest cost patients in a large nationwide US healthcare system.
Multimorbidity was examined using chronic condition counts and a clinical construct that incorporated conditions involving multiple body systems/specialties.
Chronic condition and utilisation data were drawn from a single year; longitudinal patterns were not evaluated.
Introduction
Across a range of healthcare settings and populations, a small number of patients account for disproportionate costs. Within the USA, 5% of the population accounts for approximately half of the healthcare spending,1 and similar patterns have been observed among patients covered by Medicare and Medicaid.2 ,3 Approximately 20–60% of these individuals remain in the highest cost categories in the following year.4–6 Given the pressing demands to contain escalating healthcare costs, many healthcare systems seek to understand and address the needs of these patients.7
Previous evaluations of high-cost patients have identified a high prevalence of common chronic conditions such as diabetes, asthma and hypertension, as well as disproportionate rates of complex and severe conditions such as heart failure and cancer.2 ,6 Mental health conditions are also observed at increased rates among these patients.2 ,6 ,8 However, while it is widely appreciated that many high-cost patients have multiple chronic conditions,1 ,9 little is known about the association between multimorbidity and healthcare utilisation patterns among these individuals. In the general population, multiple chronic conditions have been associated with increased rates of hospitalisations and physician visits,10 but these relationships have not been investigated among high-cost patients.
Understanding high-cost patients’ chronic condition patterns and associated healthcare needs is likely to be of particular interest within healthcare systems that are accountable for high-risk patients. In order to inform programme development, we sought to investigate chronic conditions, multimorbidity patterns and utilisation of services among individuals with high costs in a single year in the Veterans Affairs (VA) Health Care System, the largest integrated healthcare system in the USA. Our objectives were to: (1) characterise the VA's 5% highest cost patients over a 1-year period in terms of their chronic conditions and multimorbidity patterns and (2) determine the associations between multimorbidity and healthcare utilisation and costs among these patients.
Methods
Population and data sources
The VA Health Care System serves close to six million veterans of the US military per year through 150 medical centres and 820 community-based outpatient clinics. The VA is considered a leader in the delivery of high-quality care in the USA.11 ,12 Patients in the VA are predominantly male and typically have higher rates of physical and mental illness, and are poorer, than age-matched non-Veterans. In addition, younger Veterans (individuals deployed after 9/11) have high rates of physical and emotional trauma, including post-traumatic stress disorder. Patients are eligible not only for health benefits, but also for substantial social support including disability payments, pensions, educational benefits, housing support and vocational rehabilitation.
For this cross-sectional study, we used VA medical data files to identify 5 233 994 patients who received any inpatient or outpatient VA care during fiscal year 2010 (1 October 2009 to 30 September 2010). We calculated the total cost of VA care for each patient, aggregating costs of inpatient, outpatient, pharmacy and VA-sponsored contract care (non-VA inpatient and outpatient services that are covered by the VA). Since there are no billing records in the VA, we used 2010 Average Costs data files to obtain cost estimates for inpatient and outpatient care based on non-VA relative value weights.13–15 We used 2010 Decision Support System pharmacy files to obtain costs of prescription drugs filled in the VA, and 2010 Fee Basis files to obtain service-specific payments made to non-VA providers for contract care.
Patient characteristics
Chronic conditions and sociodemographics
For all patients, we identified the presence of 33 chronic conditions that have been the focus of previous quality improvement efforts and research within the VA due to their prevalence, management challenges and/or cost16–19 (see online supplementary appendix table 1). We restricted our determination to conditions that were documented by ICD-9 codes at least twice across different inpatient or outpatient encounters to avoid unconfirmed or rule-out diagnoses. We also obtained sociodemographic characteristics, including age, sex, race/ethnicity, marital status and documented homelessness during the year of investigation. Missing data were categorised as unknown and occurred at rates less than 10% for all variables. We categorised patients based on their non-VA health insurance status as having no outside medical insurance, having Medicare and/or Medicare supplemental coverage, or having other private or public insurance.
Multimorbidity measures
We assessed multisystem multimorbidity by grouping chronic conditions into body systems using an algorithm established by the Agency for Healthcare Research and Quality.20 We used this as the primary multimorbidity measure in analyses to account for the possibility that healthcare utilisation patterns may be influenced less by the number of specific conditions than by the number of different specialists and different diagnostic and treatment modalities that are required for chronic disease management. In sensitivity analyses, we also measured multimorbidity using a count of chronic conditions listed in online supplementary appendix table 1. Both multimorbidity measures were analysed as ordered categorical variables in regression models.
Healthcare costs and utilisation
For each patient, we calculated the total cost of care and the share of costs generated through inpatient, outpatient, pharmacy and VA-sponsored contract care using the data sources and estimation methods described above.13–15 We also determined the number of primary, medical specialty and mental healthcare visits, emergency department visits, and admissions for medical, surgical or mental healthcare, categorising encounters by clinic identifier codes (for outpatient utilisation) and treating specialty codes that indicate location of care (for inpatient utilisation).
Analyses
We categorised patients as high cost if their total costs of care were among the top 5% for all patients assessed. We used χ2 and t tests in bivariate analyses to compare high-cost patients with individuals in the remaining population on the basis of sociodemographic characteristics, chronic conditions and multimorbidity prevalence, using an a priori significance level of p<0.01 to adjust for multiple comparisons.
Multimorbidity patterns
We explored patterns of multimorbidity in several ways. First, we compared the chronic condition prevalence, number of chronic conditions and number of body systems affected by chronic conditions (multisystem multimorbidity) among high-cost patients and the remaining patient population. Next, we examined multisystem multimorbidity patterns by identifying body system dyads affected by chronic conditions and comparing the relative prevalence of dyads among high-cost patients and all other patients. We also coded chronic condition triads, as described in previously published studies of VA patient populations.19 ,21 All coded conditions were searched for all patients and all existing trios of comorbid conditions were identified. The quantity of high-cost patients with each of these identified trios was tabulated to determine the trios that were present in at least 5% of patients. Finally, we explored variations in multimorbidity rates among patients with the five most common medical conditions and the five most common mental health conditions.
Association between multimorbidity and healthcare utilisation and cost
Using multivariate regression, we examined the relationship between multisystem multimorbidity and (1) total annual healthcare costs, (2) absolute and share of total costs generated through outpatient, inpatient and pharmacy care and (3) number of primary, specialty and mental healthcare visits, emergency department visits, and hospitalisations over the year of investigation. All regressions adjusted for patient age, sex, race/ethnicity, marital status, documented homelessness during the year of investigation, health insurance status and correlation within facilities. In sensitivity analyses, we repeated regressions substituting comorbidity count for multisystem multimorbidity. We also repeated regressions after excluding individuals who died in the year of investigation, to determine whether findings were influenced by end-of-life utilisation and costs.
To examine differences in absolute costs (total and specific categories), we utilised ordinary least squares regression. To examine differences in the share of costs generated through inpatient care, outpatient care and pharmacy care, we used fractional logit regression.22 Finally, to evaluate differences in utilisation (count variables with excess zeros), we used zero-inflated negative binomial regression and zero-inflated Poisson regression, and we report findings for the models with best fit. For each model, we present predicted values of the outcome for each level of multimorbidity, holding other covariates at their mean value in order to illustrate the effect of multimorbidity on the outcome of interest. We also present the average difference across multimorbidity groups, which represents the average predicted change in the dependent variable (absolute cost, share of total cost or utilisation count, respectively) per each additional body system affected by chronic conditions. Average differences are estimates, via unweighted ordinary least squares, of the slope of a linear regression of cost on multimorbidity count, where body system counts of seven and greater were coded as seven. Statistical significance was calculated using estimated coefficients and SEs from the regressions. We explored alternative regression models, including linear regression for all analyses, to ensure optimal fit of our selected models.
We used Stata V.12.0 (StataCorp 2011, College Station, Texas, USA) to perform all analyses. Analyses used de-identified data and were approved by the Stanford University Institutional Review Board.
Results
High-cost patients (n=261 699) accounted for 47% of total VA costs in 2010. In aggregate, inpatient care accounted for 50% of costs, outpatient care for 32% of costs, and pharmacy and VA-sponsored contract care for 8% and 10% of costs, respectively. Table 1 describes healthcare costs and sociodemographic characteristics for high-cost patients compared with the remaining 95% of VA patients (table 2).
Characteristics of the 5% highest cost patients compared with the remaining population receiving VA care in 2010
Relationship between multimorbidity and absolute† and share‡ of total costs generated through inpatient, outpatient and pharmacy care among high-cost VA patients
Chronic conditions and multimorbidity patterns
Chronic condition prevalence was greater among high-cost patients than among the remaining 95% of patients for all specific conditions assessed (see online supplementary appendix table 1). The most common chronic conditions among high-cost patients included hypertension (63%), diabetes (34%), depression (29%) and ischaemic heart disease (27%). One in four patients (25%) had a diagnosis of cancer, and close to half (48%) of high-cost patients had a diagnosed mental health condition.
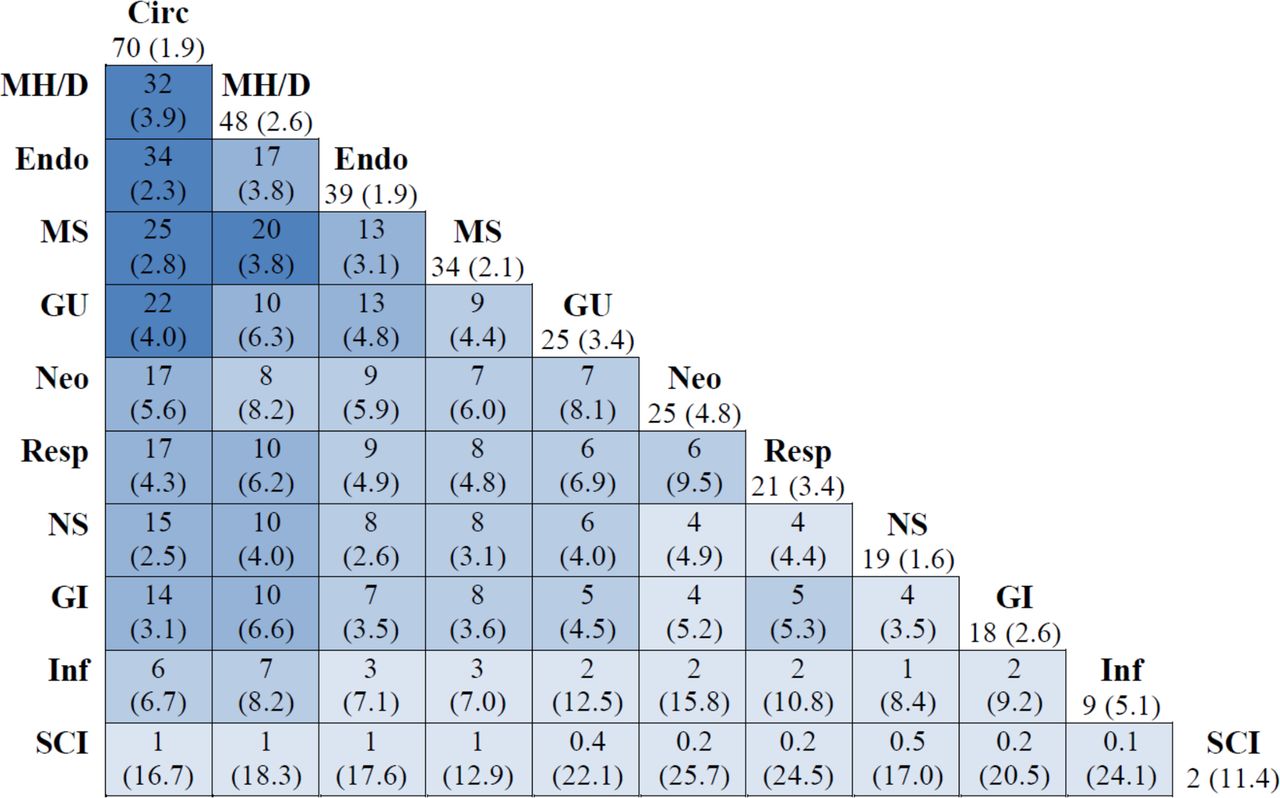
Multimorbidity was extremely common among high-cost patients, with 77% and 41% having ≥3 and ≥5 chronic conditions, respectively, and 64% and 18% having ≥3 and ≥5 body systems affected by chronic conditions, respectively (table 1). Multisystem multimorbidity most commonly involved circulatory conditions paired with endocrine conditions (34%), mental health conditions (32%) and musculoskeletal conditions (25%). Mental health conditions also frequently co-occurred with musculoskeletal conditions (20%) and endocrine conditions (17%) (figure 1). The most prevalent triads of specific chronic conditions are listed in online supplementary appendix table 2.

Prevalence of body systems affected by chronic conditions and multisystem multimorbidity among high-cost VA patients (relative to remaining 95% of patients). Numbers at the top of each column represent the percentage of high-cost patients with one or more chronic conditions affecting the specified body system. Numbers within each cell represent the percentage of high-cost patients with chronic conditions affecting the dyad of body systems on both horizontal and vertical axes. Numbers in parentheses represent the relative prevalence when comparing high-cost patients with the remaining population. Shades highlight different prevalence levels, with darker shades representing higher rates (<5%, 5–9%, 10–19% and ≥20%, respectively). For the prevalence and relative prevalence of specific chronic conditions, see online supplementary appendix table 1. Circ, circulatory; Endo, endocrine; GI, gastrointestinal; GU, genitourinary; Inf, infectious; MH/D, Mental Health and Dementia; MS, musculoskeletal; Neo, neoplasm; NS, nervous system/sense organs; Resp, respiratory; SCI, spinal cord injury; VA, Veterans Affairs.
Figure 2 illustrates multimorbidity rates among patients with the five most common medical and five most common mental health conditions. For the majority of specified conditions, as many as two-thirds of affected patients had ≥5 total comorbidities. For certain conditions, however, such as cancer and schizophrenia, fewer than half of the affected patients had this level of multimorbidity. Among patients with cancer and schizophrenia, 22% and 18% had no more than one comorbid condition, respectively. In contrast, among patients with all other conditions listed, only 5–11% of affected patients had no more than one comorbid condition.

{kind=link}
{kind=link}
Variation in number of comorbidities among high-cost Veterans Affairs (VA) patients with common medical and mental health conditions (PTSD, post-traumatic stress disorder).
Association between multimorbidity and healthcare utilisation and costs
Among high-cost patients, there was a positive association between multimorbidity and healthcare costs, with an average increase of $1774 in total costs for each body system affected by chronic conditions (p<0.01). However, the association between multisystem multimorbidity and costs varied for outpatient versus inpatient care. For outpatient care, each additional body system affected by chronic conditions was associated with an average increase of $1444 in outpatient costs, which translated to a 1.6 percentage point increase in outpatient share of total costs (p<0.01). In contrast, for inpatient care, each additional body system affected by chronic conditions was associated with an average increase of $577 in inpatient costs, but this translated to a 0.6 percentage point decrease in inpatient share of total costs (p<0.01). Patterns did not change markedly after excluding individuals who died in the year of investigation (see online supplementary appendix table 3).
Sensitivity analyses examining cost differences by number of specific chronic conditions rather than by number of affected body systems can be found in online supplementary appendix table 4. While the positive and strong association between multimorbidity and predicted share of outpatient costs was unchanged, higher chronic condition counts were associated with a small but statistically significant increase in inpatient share of total cost and a decrease in the share of costs attributed to pharmacy. These findings are most likely related to the high rates of cancer and schizophrenia among patients with one condition, as both of these diseases are associated with frequent inpatient utilisation and many cancer medications are extremely costly.
Multisystem multimorbidity was associated with an increase in utilisation of most healthcare services (table 3). Each additional body system affected by chronic conditions was associated with an average increase of 0.2 hospitalisations and 0.4 emergency department visits, as well as an average increase of 1.5 primary care visits and 0.7 specialty care visits. All associations between multisystem multimorbidity and these utilisation categories were significant at p<0.01. No association was detected between multisystem multimorbidity and number of mental healthcare visits when all patients were included in analyses. However, among the subgroup of patients with a mental health diagnosis (n=125 962), there was a decrease in 1.9 mental healthcare visits per each body system affected by chronic conditions (p<0.01).
Relationship between multisystem multimorbidity and mean annual healthcare utilisation† among high-cost VA patients
Discussion
The 5% highest cost patients in the US VA Health Care System in 2010 accounted for approximately half of the total healthcare spending. Multimorbidity is common among these patients, and approximately two-thirds have chronic conditions affecting three or more body systems. We observed a number of multimorbidity patterns and associated healthcare utilisation trends that may inform healthcare delivery models for complex, high-cost patients.
First, our findings suggest that programmes for high-cost patients need to address individuals’ challenges across multiple conditions. Several systematic reviews and guidelines have described strategies to improve care for patients with multimorbidity, for example through specialty care coordination, medication reconciliation, self-management support, and elimination of redundant testing and services.23–25 Recent reviews of primary care interventions and guidelines for managing multiple chronic conditions have also emphasised the importance of considering patient preferences, functional difficulties and prognosis when developing care plans.23 ,25 By incorporating these strategies, intensive primary care programmes could potentially reduce the volume and burden of healthcare for high-cost patients with multiple chronic conditions.
Second, while programmes for high-risk, high-cost patients frequently concentrate on preventing hospitalisation and reducing length of stay,26 ,27 our findings suggest that high-cost patients with multiple chronic conditions may also benefit from attention to the appropriateness of outpatient services. We found that greater multisystem multimorbidity was associated with marked increases in outpatient services and a higher share of costs generated in the outpatient setting, and a lower share of costs generated in the inpatient setting.
These findings contribute to a growing body of literature that aims to inform healthcare delivery models for high-cost patients. Recently, a study published in JAMA determined that among high-cost Medicare patients, only a small percentage of costs from hospitalisation and emergency department visits were related to health deteriorations that may have been prevented through high-quality primary care. The authors concluded that it will be challenging to lower costs for these patients through better outpatient care.2 However, we found that outpatient care was a major contributor to costs in high-cost VA patients, especially among patients with high levels of multimorbidity, suggesting that at least among a subset of high-cost patients there may be an opportunity to influence total cost through highly coordinated and efficient services in the outpatient setting.
Third, our findings suggest a need for strategies that address high-cost patients’ mental health. Close to half of our study population had a mental health diagnosis, and similarly high rates have been observed among high-cost Medicaid patients.8 In VA and Medicaid high-cost patients, mental health diagnoses frequently co-occur with cardiovascular, endocrine and musculoskeletal conditions—conditions for which there is substantial literature describing increased risk and higher utilisation when comorbid mental illness is present.28–32 Interestingly, among patients in our sample who had a mental health diagnosis, frequency of outpatient mental healthcare was inversely correlated with greater multisystem multimorbidity. This finding may be driven by patients with serious mental illness and low multimorbidity who incur high costs through their frequent use of mental health services. However, another potential explanation is that patients with multiple chronic conditions may be overwhelmed and saturated with care and do not receive the intensity of mental healthcare that they need. This latter scenario would support a role for integrated care models that address comorbid mental illness together with complex and costly medical conditions.
Finally, this study highlights the heterogeneity of patients with high costs, and suggests that a one-size-fits-all intervention may not be the optimal approach. The evidence base for intensive interventions is still limited, and important questions remain about how best to identify patients and match services to their needs. There may be individuals with stable chronic conditions and strong social support who are unlikely to benefit substantially from intensive management programmes. Other patients may have highly specialised needs. For example, while the majority of high-cost patients in our study had multiple chronic conditions, we identified subgroups of patients with cancer and schizophrenia who have lower levels of multimorbidity. This finding is notable because intensive primary care programmes that are focused on coordinating care for multiple chronic conditions may not be the best fit for patients whose care needs are dominated by these types of conditions. Health systems may instead choose to ensure that high-cost patients who have cancer or a serious mental illness but few comorbidities receive care within multidisciplinary programmes that are focused on these diseases.
These analyses are limited by several factors. First, our findings reflect patterns observed among patients who were identified as high cost over a 1-year period, and might not be generalisable to the 20–60% of high-cost patients who persist in this category over 2 years.4–6 Second, there is little consensus about how best to define multimorbidity and how to categorise conditions in studies of multimorbidity. We attempted to address this by examining both comorbidity counts and multisystem multimorbidity (the latter of which may better reflect patients’ requirements for different specialists and services33). Third, we chose to limit our analyses to 33 chronic conditions that have been the focus of previous studies within the VA because of their prevalence, management challenges and/or cost.16 While not exhaustive, we feel that this list represents the most common, complex and costly conditions across a range of body systems. Fourth, the VA does not routinely bill for healthcare services, so we used cost estimates based on non-VA relative value weights13 ,14 which compare favourably to activity-based costing methods without needing to adjust for local input prices.34
In addition, observed chronic condition (and multimorbidity) prevalence may be influenced by coding accuracy. Certain conditions, such as dementia, are frequently under-coded,35 and comorbidity under-coding may occur more frequently in a patient with a severe and complicated condition such as cancer or serious mental illness. VA providers are not incentivised to assiduously code conditions in the way that providers in Medicare Managed Care are, which could lead to under-coding. We also used a fairly stringent coding definition based on ICD-9 diagnoses being present at least twice in inpatient or outpatient records. However, previous assessments have found that using more restrictive coding definitions can reduce the observed prevalence of individual conditions but does not change their rank order in a meaningful way.21 Finally, the relationships that we observed may be limited to the VA population; however, the VA is a very large healthcare system and its patients’ high rates of physical and psychosocial health problems are similar to those observed in safety net systems worldwide.
In conclusion, our analyses of high-cost patients in the VA healthcare system suggest that while certain individuals such as some patients with cancer or serious mental illness may benefit from disease-specific interventions, the majority most likely require programmes that address their heterogeneous health needs. As multimorbidity affects a greater number of body systems, patients incur a higher share of their costs as outpatients, suggesting a role for intensive primary care programmes that coordinate specialty care and eliminate redundant testing and unnecessary visits. In order to achieve maximal value, these programmes should ensure that their focus extends beyond preventing hospitalisation and should identify opportunities to reduce the volume and burden of outpatient care for patients with multiple chronic conditions.
Acknowledgments
The authors thank Jennifer Yang Scott for her assistance in database development and management.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors DMZ conceptualised the study and wrote the article. DMZ, CPC and DMC conducted data analyses. THH provided guidance in statistical analyses. All authors contributed to the design of the study, helped interpret the findings and approved the final version of the manuscript.
Funding DMZ is supported by a U.S. Department of Veterans Affairs (VA) HSR&D Career Development Award (CDA 12-173). CPC, THW, and JY received core funding SDR-ECN-99017-1 to the VA Health Economics Resource Center. THH and DMC are supported in part by the VA Office of Specialty Care Services (Specialty/Surgical Care Neighborhood Team Based Model Pilot Program). CR is supported by the Advanced Illness and Multimorbidity Geriatric Academic Leadership Award (1K07AG31779).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.