Article Text

Abstract
AIMS To assess the long term therapeutic effectiveness, safety, and tolerability of low daily doses of isosmotic PEG electrolyte solutions (PMF-100) administered for a six month period for the treatment of functional constipation, in a double blind, placebo controlled, parallel group study.
METHODS After an initial four week run in period with PMF-100 (250 ml twice daily; PEG 14.6 g twice daily), 70 patients suffering from chronic constipation (58 females, aged 42 (15) years) with normalised bowel frequency (>3 bowel movements (bm)/week) were randomly allocated to receive either PMF-100 or placebo, contained in sachets (one sachet in 250 ml of water twice daily) for 20 weeks. Patients were assessed at four week intervals, and reported frequency and modality of evacuation, laxative use, and relevant symptoms on a diary card. At weeks 1, 12, and 24, a physical examination and laboratory tests were performed.
RESULTS Complete remission of constipation was reported by a significantly (p<0.01) higher number of patients treated with PMF-100 compared with placebo at each four week visit. At the end of the study, 77% of the PMF-100 group and 20% of the placebo group were asymptomatic. Compared with placebo, patients treated with PMF-100 reported hard/pellety stools and straining at defecation less frequently, a significantly higher bowel frequency (week 12: 7.4 (3.1) v 4.3 (2.5) bm/week, 95% CI 1.64, 4.42; week 24: 7.4 (3.2)v 5.4 (2.1) bm/week, 95% CI 0.13,3.93), reduced consumption of laxative/four weeks (week 12: 0.7 (2.7)v 2.2 (3.3), 95% CI −2.29, 0.03; week 24: 0.2 (0.8) v 1.4 (2), 95% CI −2.07, −0.023), reduced mean number of sachets used (week 12: 33 (13)v 43 (12), 95% CI −17.24, 4.56; week 24: 33 (13) v 44 (12), 95% CI −19.68, −2.24), and reduced number of drop outs for therapy failure (16v 3; p<0.005). Adverse events, physical findings, laboratory values, palatability, and overall tolerance of the solutions did not differ between groups.
CONCLUSIONS Administration of small daily doses of isosmotic PEG electrolyte balanced solutions was effective over a six month period for the treatment of functional constipation. A mean daily dose of approximately 300 ml of PEG solution (PEG 17.52 g) appeared to be safe, well tolerated, and devoid of significant side effects.
- constipation
- polyethylene glycol
- safety
- tolerability
Statistics from Altmetric.com
Polyethylene glycol (PEG) solution has been used favourably in high daily doses for acute treatment of faecal impaction1 2 and severe constipation.3 4Low daily doses of PEG solution are also effective for the treatment of chronic constipation. The therapeutic effectiveness of PEG solutions has been assessed for only a few days5 6 and, more recently, over a two month period in chronic non-organic constipation.7 In the latter study, PEG solution at a mean daily dose of 440 ml (PEG 25.7 g) was effective in increasing bowel frequency and accelerating colorectal transit time. It also improved difficult defecation. The treatment appeared to be effective for the period of administration and was devoid of significant side effects. It is not known, however, if prolonged administration of PEG solution at a low daily dose is effective, safe, and well tolerated for the long term treatment of chronic constipation.
The aims of this multicentre, double blind, placebo controlled, parallel group study were to assess the therapeutic effectiveness, safety, and tolerability of low daily doses of isosmotic PEG solutions for the long term treatment of chronic non-organic constipation.
Materials and methods
PATIENTS
Patients seeking medical advice for chronic constipation were investigated over a 24 month period in the outpatient clinics of the participating centres.
Inclusion criteria were patients aged 18–75 years and presenting with chronic constipation, defined in accordance with the Rome diagnostic criteria (less than two bowel movements (bm) a week for at least 12 months or the presence of two or more of the following complaints when laxatives and/or enemas were not used: less than three bowel movements a week; straining at defecation; sense of incomplete evacuation; and hard stools on at least 25% of occasions). Other criteria were: negative tests for organic disorders of the digestive tract; no anorectal lesions; no abnormality at barium enema or colonoscopy; and normal laboratory tests (routine laboratory examinations and serum calcium, phosphorus, T3, T4, and TSH).
Exclusion criteria were: patients not meeting the inclusion criteria; inflammatory bowel disease; pregnant women or women not using effective contraceptive measures; previous surgery on the gastrointestinal tract, except appendicectomy and cholecystectomy; chronic use of drugs affecting gastrointestinal motility; and chronic systemic, metabolic, neurological, and psychiatric illnesses. The study was approved by the local ethics committee. All subjects gave written informed consent.
STUDY DESIGN
This was a multicentre (five centres) trial. The study was subdivided into two consecutive periods. In the first initial period of four weeks' duration, all patients received active treatment (PMF-100). In the second period of 20 weeks duration', responders to the initial treatment entered into a trial run according to a randomised, double blind, placebo controlled, parallel group design.
After a medical history and physical examination were performed at visit 1, patients entered the initial four week period during which they were treated with PMF-100 and were instructed to standardise their diet so as to have a mean daily intake of 15 g of fibre and 1500 ml of water and to refrain from laxatives, rectal evacuants, and enemas. Patients who responded at the end of the initial four week period (visit 2) were allocated to receive, in a double blind manner for the following 20 weeks, active treatment with PMF-100 (group I) or placebo (group II), according to a randomisation code independent for each centre. Patients were defined as responders at visit 2 if they referred and reported on the diary card that during the previous two weeks of treatment they had at least 2 bm/week and no other defecatory disturbances or at least 3 bm/week with or without defecatory disturbances.
During the study no other medication was allowed. Laxatives were allowed only when patients had no bowel movements for at least five consecutive days. After each four week period of treatment and at the end of the study, patients were required to attend for a visit (visits 3–7).
At each visit, patients were given 56 sachets for the subsequent four week period and four weekly diary cards on which they reported daily the number of sachets taken, number of evacuations, stool consistency (soft, firm, hard, pellety), straining (absent or present) at defecation, use of laxatives (oral, suppository) or enemas, and the following symptoms: abdominal pain, abdominal bloating, flatulence, borborygmi. The presence of the abdominal symptoms were specifically asked for by the physician who rated them as: absent; mild, not interfering with daily activities; moderate, interfering with daily activities; moderately severe, requiring medication; severe, requiring urgent medical assistance. At visits 2, 3, 4, 5, 6, and 7, patients returned the completed diary cards and the remaining sachets.
At visits 1, 4 and 7, patients underwent a physical examination, and heart frequency and blood pressure were recorded, together with the following laboratory analyses: full blood count, serum concentrations of sodium, potassium, creatinine, glucose, transaminases, and alkaline phosphatases, and BUN. Serum levels of calcium and phosphorus, and ESR were assessed at visit 1.
At visits 2 and 7, patients were asked about tolerability of the PEG solution in terms of taste (pleasant, indifferent, unpleasant); daily volume ingested (low, adequate, excessive); and modality of preparation (easy, difficult).
TREATMENT
Active treatment (PMF-100; Normopeg (Selg 250 in Italy), Promefarm Srl Milan, Italy) was supplied as a granular preparation contained in sachets. Each 17.5 g sachet contained the following active ingredients: polyethylene glycol 4000 14.6 g; anhydrous sodium sulphate 1.42 g; sodium bicarbonate 0.42 g; sodium chloride 0.36 g; potassium chloride 0.18 g; simethicone (activated dimethicone) 0.01 g; and orange flavour. Placebo, containing 16.92 g of orange flavoured maltodextrine, was supplied in an identical form, and the smell, colour, and taste of both preparations were similar. Patients were instructed to dissolve the contents of each sachet in 250 ml of water before ingestion. The dose was one sachet twice daily; patients were allowed to reduce the dose to once daily according to bowel movement frequency. In no case were they allowed to increase the dose.
PATIENT ASSESSMENT
Bowel frequency, straining at defecation, stool consistency, use of oral and rectal laxatives or enemas, and relevant symptoms were collected from data reported on the diary card and assessed at each visit. Bowel frequency was expressed as the number of evacuations per week, and normal frequency was considered to be at least three evacuations per week.
The severity of each symptom was scored by the physician on a five-point scale: absence of symptoms (0), mild (1), moderate (2), moderately severe (3), and very severe (4). The score for each symptom was evaluated separately.
Treatment compliance was assessed by direct interview of the patient, checking the diary cards on which the daily number of sachets taken was recorded, and counting the sachets brought back by the patient at each visit.
DATA ANALYSIS
To assess the therapeutic effectiveness of PMF-100, the primary criteria were complete remission of constipation consisting of ⩾3 bm/week, no use of laxatives, no straining at defecation, feeling of complete evacuation, and no hard/pellety stools. Secondary criteria were: bowel frequency and normalisation of bowel frequency, use of laxatives, straining at defecation, stool consistency, and presence of other symptoms.
It was hypothesized that patients assigned to the placebo group could more likely interrupt the study than those treated with PMF-100. Thus the number of drop outs caused by no response to treatment was assessed and used as an additional criterium to evaluate the therapeutic effectiveness of PMF-100.
Because of the high number of drop outs in the placebo group after the first eight weeks of treatment (see results), data were analysed for the entire treatment period and for the first eight week period (visit 4).
Results are expressed as mean and standard deviation (SD). Fisher's exact test was used to compare the frequency of symptoms in the two groups under basal conditions and at the end of the run in period. Non-parametric tests (Mann-Whitney) and analysis of variance (Koch) were used to assess bowel frequency, daily sachet intake, use of laxatives, straining at defecation, stool consistency, and abdominal symptom score. Patients' judgments about taste and volume of any single dose of solution at the end of the run in period and at the end of the study were evaluated using McNemar's test.
Results
The five participating centres enrolled 78 patients, eight of whom did not enter the study: three presented side effects (vomiting, abdominal pain); two could not guarantee that they were using adequate contraceptive measures; one disliked the taste of the solution; one gave no reason; and one did not respond at the end of the first four week run in period.
Thus 70 patients entered the study (12 men, 58 females, mean age 43 (SD 15) years, range 18–73 years); 33 patients were assigned to PMF-100 treatment (group I) and 37 patients to placebo (group II). Patient profiles are summarised in table 1. The two groups were comparable in sex, age, and baseline features of constipation.
Demographic data (mean (SD) or number) and baseline features of constipation (percentage of patients) in the two patient groups
There was no significant difference between groups in stool frequency, straining at defecation, stool consistency or use of laxatives at the end of the run in period (table 2).
Bowel habits (mean (SD) or percentage of patients) in the two patient groups at the end of the run in period with PMF-100 treatment
At the end of the run in period, bowel frequency was normal in 32/33 patients in group I and in all patients in group II (NS).
Of the 33 patients assigned to PMF-100, all but one completed the first eight week period, and 23 completed the entire study of 20 weeks. Of the 37 patients assigned to the placebo group, four did not complete the initial eight week period and an additional 18 patients did not complete the entire study. Overall, 69.7% of group I completed the trial compared with 30.3% of group II (p<0.01). Non-response to treatment was the cause of withdrawal in 6.7% of patients in group I and in 45.9% of those in group II (p<0.005). Other causes of withdrawal did not differ between groups: three patients did not present at the visit and one patient received medications other than the study medications in each group; in the PMF-100 group, three patients dropped out (two for adverse events and one for taste intolerance).
The number of sachet intake/four weeks did not differ between groups at the end of the run in period (38.1 (12.1) sachets/four weeks in group I and 38 (15) sachets/four weeks in group II; 95% CI −6.04, 6). In the PMF-100 group, mean daily sachet intake decreased progressively from visit 2 to visit 7 (33 (13) sachets/four weeks; 95% CI −1.5, 12.24); in the placebo group, it increased progressively from visit 2 to visit 7 (44 (12) sachets/four weeks; 95% CI −14.3, 3.16). Difference in intake of daily sachets during the treatment period in the active and placebo groups was statistically significant (p<0.001).
Complete remission of constipation symptoms (i.e. bowel frequency exceeding three evacuations per week with no use of laxatives, no straining at defecation, feeling of complete evacuation, and no hard/pellety stools) was reported by 67% of patients in group I and by 68% of those in group II (NS) at the end of the run in period (fig 1). Complete remission of constipation symptoms was reported by a significantly (p<0.001) greater number of patients in the PMF-100 group than in the placebo group at each visit throughout the study. At the end of the study, 77% of the PMF-100 group and 20% of the placebo group were asymptomatic (fig 1).

Percentage of patients with complete remission of constipation symptoms consisting of more than three bowel movements per week, no use of laxatives, no straining at defecation, feeling of complete evacuation, and no hard/pellety stools during PMF-100 and placebo treatment. The two groups did not differ at the end of the run in period; a significantly higher number of patients with complete remission of constipation was observed in the PMF-100 group at each visit throughout the study (***p<0.001).
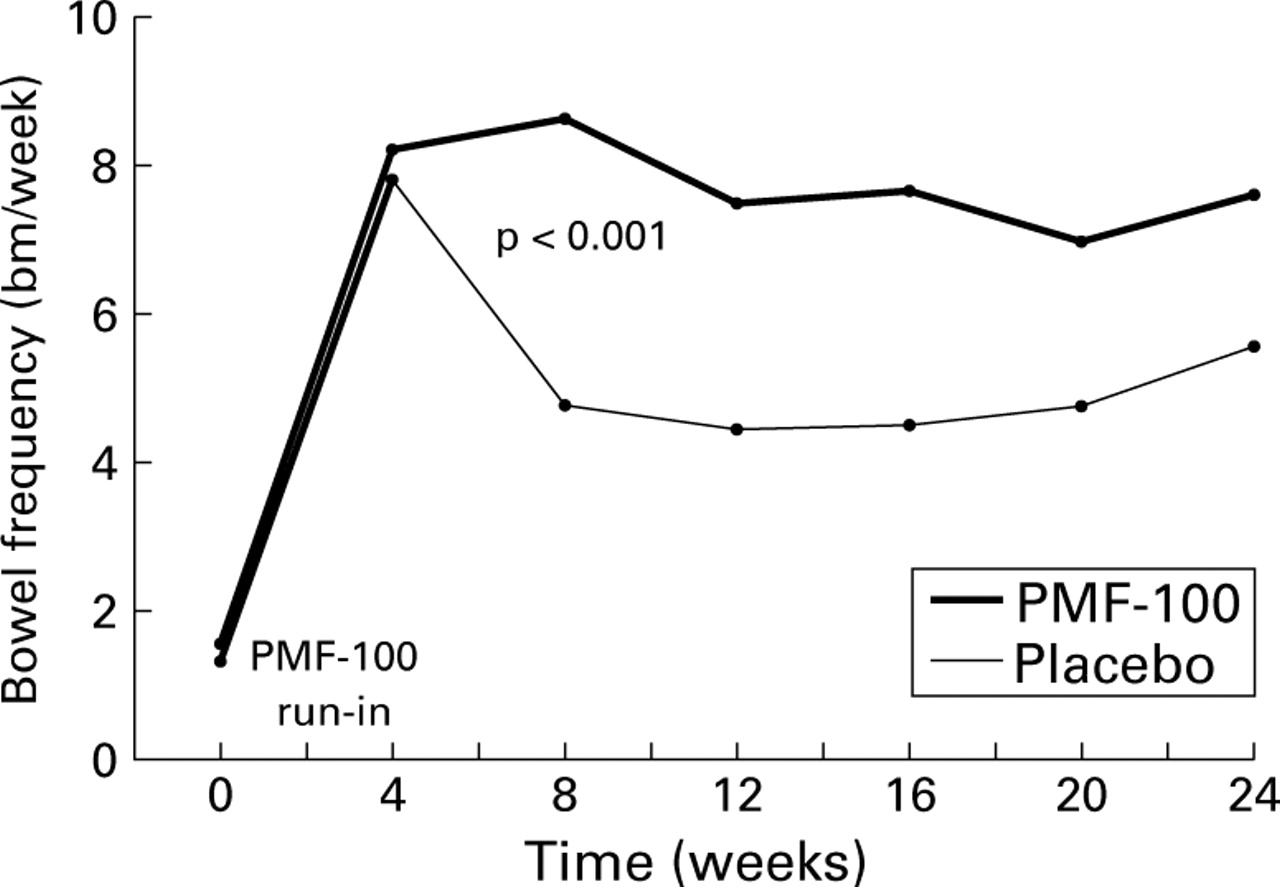
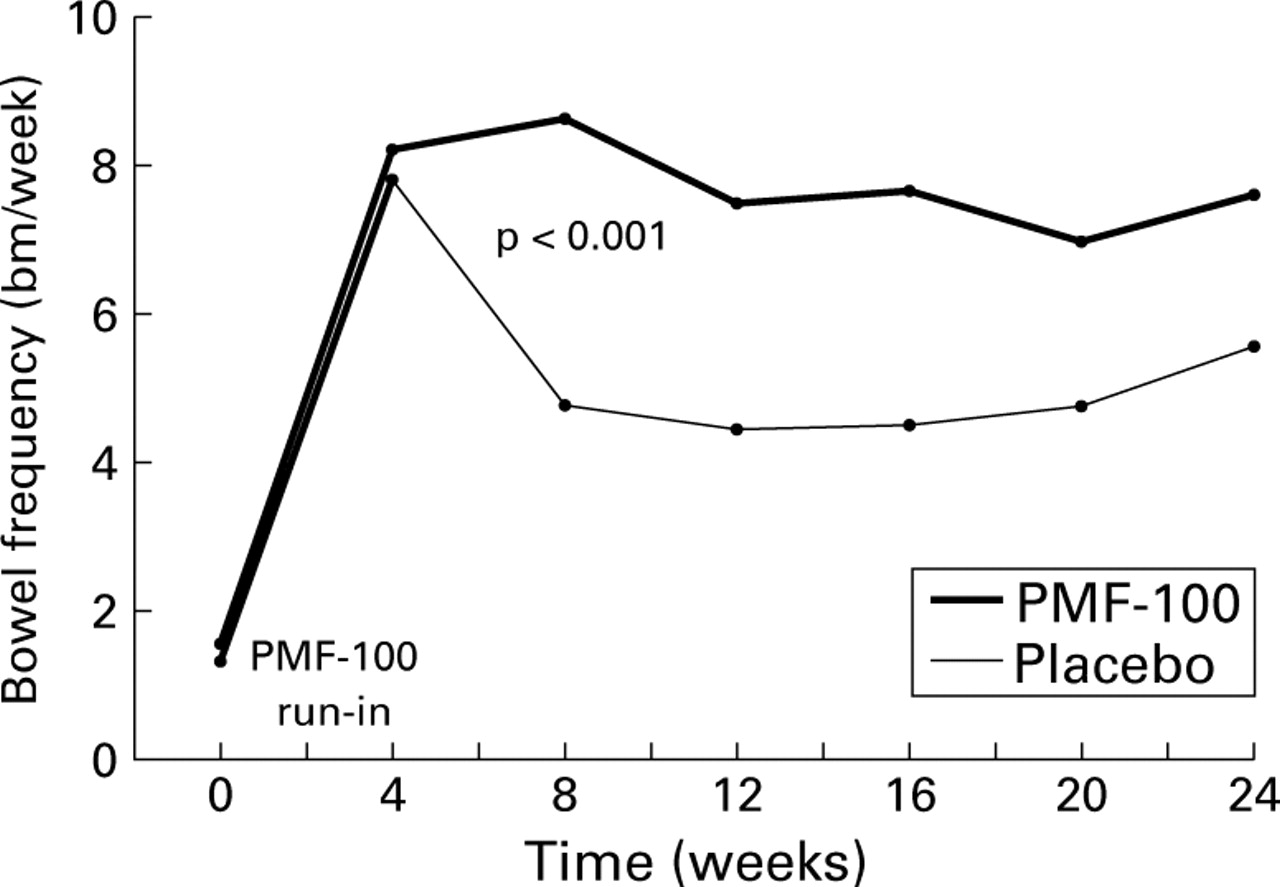
Throughout the 20 week study, weekly bowel frequency in group I patients did not vary significantly, ranging from 8.3 (4) at visit 2 to 7.4 (3.1) bm/week at visit 7 (95% CI −1.18, 2.88). In the placebo group, bowel frequency decreased significantly from 7.7 (4) bm/week at visit 2 to 4.3 (2.5) bm/week at visit 4 (95% CI 1.61, 5.03). From visit 4 to visit 7 it did not vary significantly (95% CI −2.56, 0.46) (fig. 2). Compared with basal values, bowel frequency was normal in 96% of patients in the PMF-100 group and in 80% of those in the placebo group (p<0.001).
{kind=link}
{kind=link}
Bowel frequency during the run in and study periods with PMF-100 and placebo treatments. After the run in period, bowel frequency was significantly higher in the PMF-100 group throughout the study.
Straining at defecation was reported less frequently during PMF-100 treatment (p<0.001 at visit 4). On completion of treatment, pronounced straining was still reported by 49% of placebo patients and by 22% of those who received active treatment (p<0.001).
Hard/pellety stools were reported more frequently during the entire study in the placebo than in the PMF-100 group; at the end of treatment, 27% of patients in the placebo group complained of hard/pellety stools compared with 4% of the PMF-100 group (p<0.05).
The use of oral laxatives, rectal evacuants, suppositories, and enemas was more frequent in the placebo than in the PMF-100 group (p<0.001, at visit 4). In the PMF-100 group, intake of laxatives progressively decreased during the whole study (1.06 (2.82) bm/week at visit 2v 0.22 (0.81) bm/week at visit 7, 95% CI −0.38, 2.06); conversely, in the placebo group, laxative consumption progressively increased (0.31 (0.74) bm/week at visit 2v 1.37 (1.93) bm/week at visit 7, 95% CI −1.8, −0.32).
The score for abdominal bloating progressively decreased from 2 at visit 2 to 0.96 at visit 7 in the active treatment group; it did not vary (1.5 at visit 2 and 1.6 at visit 7) in the placebo group. Abdominal bloating was less severe in the PMF-100 than in the placebo group throughout the study (p<0.001, at visit 4).
Abdominal pain, flatulence, and borborygmi progressively decreased in the PMF-100 group and did not vary substantially in the placebo group. Abdominal pain score progressively decreased in the PMF-100 group from 0.84 at visit 2 to 0.64 at visit 7 and increased in the placebo group from 0.66 at visit 2 to 0.75 at visit 7.
The taste of the active treatment was judged to be either pleasant or indifferent by 80% of patients. Modality of preparation was judged to be easy by all but one patient. The volume of any single dose of solution was considered adequate by 75% of patients.
Adverse events, including gastrointestinal and extragastrointestinal symptoms, are reported in table 3, and their occurrence was not significantly different between groups. In only two patients in group I did adverse events (abdominal bloating and fissura in the anus, respectively) cause withdrawal from treatment.
Number of adverse events during treatment in the PMF-100 and placebo groups
Heart frequency, blood pressure, blood count, and laboratory values were within normal limits at visit 1 and did not vary significantly during the study or between groups.
Discussion
In our study, low daily doses of isosmotic and electrolyte balanced PEG solution were administered after the four week run in period for an additional 20 weeks in patients who complied with an international standardised definition of chronic constipation. The entry criteria guaranteed that the population selected had a longstanding history of constipation which presented with reduced bowel frequency. Reduced bowel frequency and difficult evacuation are the two most common complaints of patients with chronic non-organic constipation. This placebo controlled trial showed that prolonged administration of PMF-100 maintained complete remission of constipation symptoms, with a normal weekly bowel frequency, no straining at defecation, and normal stool consistency. The marked improvement in modality and frequency of evacuation accompanied by the progressive reduction of laxative-enema administration demonstrated the long term efficacy of small daily doses of PEG solution in the treatment of chronic constipation.
In contrast with treatment based on traditional laxatives, the doses of which are usually increased over time, prolonged administration of small daily doses of isosmotic PEG solutions remained effective throughout the study while the mean daily dose of PEG solution was progressively reduced from the initial dose of 340.8 ml (PEG 19.9 g) at the end of the run in period to 288.4 ml (PEG 16.84 g) at the end of the treatment period. A similar finding of dose reduction of PEG solution has been reported by Attar and colleagues.8
Differences between the two treatment regimens were less evident for some variables in the last 12 weeks of the trial. This should not be interpreted as loss of efficacy of the PMF-100 treatment, which maintained its effects throughout the study, but rather as a consequence of the numerous drop outs for treatment failure in the placebo group. Exclusion of these non-responding patients meant that the placebo group represented less severe cases of constipation and hence were clinically more similar to the PMF-100 group. This interpretation is supported by the observation that from the eighth week to the end of the trial, bowel frequency increased in the placebo group from 4 (3) bm/week to 5.4 (2.1) bm/week, while straining effort and laxative-enema consumption decreased.
Prolonged treatment with PMF-100 solutions appears to have favourable effects on abdominal bloating, abdominal pain, flatulence, and borborygmi, suggesting that a long period of normal evacuation may improve abdominal symptoms.
During administration of placebo, bowel movements decreased significantly after the end of the run in period but were significantly more frequent compared with the basal period throughout the entire trial. Similarly, in the placebo group, straining efforts at defecation increased significantly after the end of the run in period but they were none the less less frequently reported throughout the whole trial than in the pretreatment basal period.
Worsening of bowel evacuation after the end of the run in period can be interpreted as withdrawal of the active treatment. The observation that during placebo administration, (a) bowel movements were significantly more frequent and straining efforts less frequent compared with basal conditions and (b) 80.3% of patients reported at least 3 bm/week, cannot be viewed as a placebo response which usually fades away after three months, whereas in the present study bowel frequency and clinical conditions remained relatively stable for the 20 week observation period. Other explanations include: (a) standardised and relatively high fibre content of the diet9; (b) underestimation of bowel frequency under basal conditions reported by patients10 11; (c) high use of laxatives (oral and rectal) and enemas; (d) high rate of drop outs caused by no response to treatment that could have selected out those patients with more troublesome constipation, leaving those with minor alterations in bowel frequency to end the trial. Finally, we cannot exclude the fact that the one month treatment with PMF-100 may have favourably affected bowel evacuations, interrupting a longstanding cycle maintained by continuous use of laxatives or by the detrimental effect of hard pellety stools on large bowel transit and evacuation.
Overall, the tolerability and safety of long term treatment with the PMF-100 preparation at the dose administered in the present study appeared to be satisfactory. In particular, laboratory data, vital signs, and physical examination were normal in all patients before the study and did not vary throughout.
Adverse events likely to be associated with PMF-100 administration were reported by 4.4% of patients; they consisted of vomiting, abdominal bloating, and abdominal pain, and all disappeared on treatment withdrawal.
In summary, administration of isosmotic PEG electrolyte balanced solution (PMF-100) at a mean daily dose of approximately 300 ml (PEG 17.52 g) was more effective than placebo over six months for the treatment of chronic constipation. The chronic constipation symptoms disappeared in 77% of PMF-100 treated patients and in 20% of the placebo treated patients. At the dose administered, isosmotic PEG electrolyte balanced solution was devoid of significant side effects and was well tolerated.
Acknowledgments
We thank Professor P E Lucchelli for criticisms and suggestions, Professor A Bissanti for statistical analysis, and Laura Vinciguerra for typing the manuscript. The study was supported by Promefarm Srl, Milan, Italy
Footnotes
- Abbreviations used in this paper:
- PEG
- polyethylene glycol
- bm
- bowel movements