Article Text

Abstract
BACKGROUND The polymorphism of apolipoprotein E has been suggested to be associated with the cholesterol content of gallstones, the crystallisation rate of gall bladder bile, and the prevalence of gallstone disease (GSD).
AIMS To investigate whether apolipoprotein E polymorphism modulates the susceptibility to GSD at the population level and to study the possible associations between impaired glucose tolerance, diabetes, and GSD.
METHODS Apolipoprotein E phenotypes were determined in a middle aged cohort of 261 randomly selected hypertensive men, 259 control men, 257 hypertensive women, and 267 control women. All subjects without a documented history of diabetes were submitted to a two hour oral glucose tolerance test (OGTT). GSD was verified by ultrasonography.
RESULTS In women with apolipoprotein E2 (phenotypes E2/2, 2/3, and 2/4) compared with women without E2 (E3/3, 4/3, and 4/4), the odds ratio for GSD was 0.28 (95% confidence interval 0.08–0.92). There was no protective effect in men. The relative risk for GSD was 1.2 (0.8–1.7) for hypertensive women and 1.8 (1.0–2.7) for hypertensive men. In a stepwise multiple logistic regression model, E2 protected against GSD in women, whereas two hour blood glucose in the OGTT, serum insulin, and plasma triglycerides were risk factors. Elevated blood glucose during the OGTT was also a significant risk factor for GSD in men.
CONCLUSIONS The data suggest that apolipoprotein E2 is a genetic factor providing protection against GSD in women. In contrast, impaired glucose tolerance and frank diabetes are associated with the risk of GSD.
- apolipoprotein E
- gallstone disease
- diabetes
- impaired glucose tolerance
- cholesterol
Abbreviations
- Apo E
- apolipoprotein E
- BMI
- body mass index
- GSD
- gallstone disease
- HDL
- high density lipoprotein
- LDL
- low density lipoprotein
- OGTT
- oral glucose tolerance test
Statistics from Altmetric.com
The main conventional risk factors for gallstone disease (GSD) are sex, obesity, age, and ethnic background.1-5 The prevalence of gallstones in women is two to three times higher than in men and increases with age.1-4 The high prevalence of GSD in certain ethnic groups5 supports the view that there are genetic factors modulating the susceptibility to GSD. Also, low plasma high density lipoprotein (HDL) cholesterol and high plasma low density lipoprotein (LDL) cholesterol and high triglycerides may be associated with the risk of gallstones.4 ,6-8 A lipid profile of this kind as well as obesity are actually part of the risk factor cluster called the metabolic syndrome, which is associated with hypertension, non-insulin dependent diabetes, and coronary heart disease. Indeed, associations between diabetes and GSD8 ,9have been suggested.
Apolipoprotein E (apo E) is one of the key regulatory proteins in cholesterol and lipoprotein metabolism. Apo E has three common isoforms, E2, E3, and E4, which are coded by the alleles ε2, ε3, and ε4, respectively, at a single locus in chromosomal region 19q13.2. These alleles define six apo E phenotypes: E2/2, 2/3, 2/4, 3/3, 4/3, and 4/4. Apo E4 has been associated with several diseases, such as coronary heart disease10 ,11 and Alzheimer’s disease,12 ,13 which means that the possibility of subjects with apo E4 reaching extreme old age is low.14The ε2 allele is associated with low and the ε4 allele with high serum total and LDL cholesterol concentrations in various populations9 ,10 and with altered enterohepatic metabolism of cholesterol and bile acids.15 The E4 allele may protect against right sided colorectal adenoma and carcinoma.16 We and some other authors have previously shown that the cholesterol content of gallstones tends to be low in subjects with the ε2 allele and high in subjects with the ε4 allele.17 ,18 A recent study suggested that the apo E4 isoform may be a risk factor for cholelithiasis.18
We hypothesised that the ε2 allele of apo E might protect against GSD, while the ε4 allele might increase the risk. To assess the role of apo E in comparison with the conventional risk factors for GSD, we chose a middle aged population with risk factor clustering for both GSD and coronary heart disease, namely a hypertensive cohort, and randomly selected control subjects for them. The following questions were addressed: (1) does the apo E phenotype modulate the risk for GSD and (2) has impaired glucose tolerance any role in the risk for GSD in a population with a high risk of coronary heart disease?
Subjects and methods
From the population of the city of Oulu (106 500 inhabitants at the time of selection), 300 male and 300 female subjects with documented hypertension and age and sex matched controls were recruited for the study. The hypertensive subjects were randomly selected by age stratification (40–60 years) from the Social Insurance Institution register for the reimbursement of antihypertensive medication. The 600 control subjects were randomly selected from the social insurance register covering the whole population of the city of Oulu. Both of these registers are maintained by the Social Insurance Institution. The participation rate was 87.1%. All the subjects gave informed consent for the investigations, which were approved by the ethics committee of our hospital.
An abdominal ultrasound examination was carried out using a Toshiba SSA 270 ultrasound system with a scanning frequency of 5 MHz. Gallstones were diagnosed as mobile intraluminal echodensities with posterior shadowing. For the patients with prior cholecystectomy (n=83), the presence of gallstones was confirmed from the operative records. Gallstones were verified in 74 (89%) of these patients. The body mass index (BMI) was calculated as weight in kilograms divided by the square of height in metres.
Venous blood samples were drawn into EDTA tubes after an overnight fast. The plasma LDL and HDL cholesterol concentrations were estimated as described in the Lipid Research Clinics Manual of laboratory operations.19 Cholesterol and triglycerides were analysed enzymatically with kits from Boehringer Diagnostica, Mannheim GmbH, Germany, using a Kone Specific Selective Chemistry Analyser (Kone Instruments, Espoo, Finland). After fasting blood had been drawn, the subjects were given a 75 g glucose load. One and two hour blood glucose and insulin concentrations were determined, except in previously known insulin treated diabetics. Blood glucose concentrations were measured using the glucose dehydrogenase method (Diagnostica, Merck, Darmstadt, Germany). Serum insulin concentrations were measured using a two site immunoenzymometric assay (AIA-PACK IRI, Tosoh Corp., Tokyo, Japan) as described previously.20Diabetes mellitus was defined according to the WHO criteria21: known diabetes mellitus or fasting blood glucose at least 6.7 mmol/l or two hour blood glucose at least 10.0 mmol/l after the oral glucose tolerance test (OGTT). Impaired glucose tolerance was defined as fasting blood glucose less than 6.7 mmol/l, but two hour blood glucose 6.7–9.9 mmol/l.
The apo E phenotype was determined from the plasma using isoelectric focusing and immunoblotting techniques22 ,23 using commercial antibodies (Daiichi Pure Chemical, Tokyo, Japan; Bio-Makor, Rehovot, Israel). We also analysed the apo E genotype in a blind manner in a separate group of 16 diabetics and 44 controls using a solid phase minisequencing kit (Affigene ApoE, Orion Pharmaceutica Biotechnology, Espoo, Finland) as described previously24 and the phenotype and genotype matched in all cases. Thus, the possible glycation of apo E did not affect the distribution of bands and apo E phenotype classification.
Data storage and statistical analysis were performed using the SAS (Statistical Analysis System Institute, Inc., Cary, North Carolina, USA) software package. The results were expressed as means and 95% confidence intervals (CI) calculated with the CIA program.25 The differences in the means between the patients and controls with and without GSD were calculated by analysis of variance. For triglycerides, the analysis was performed after logarithmic transformation. The χ2 method was used to assess the distribution of apo E phenotypes between the groups. The stepwise multiple logistic regression analysis was performed by using the LOGISTIC procedure of the SAS package.
Results
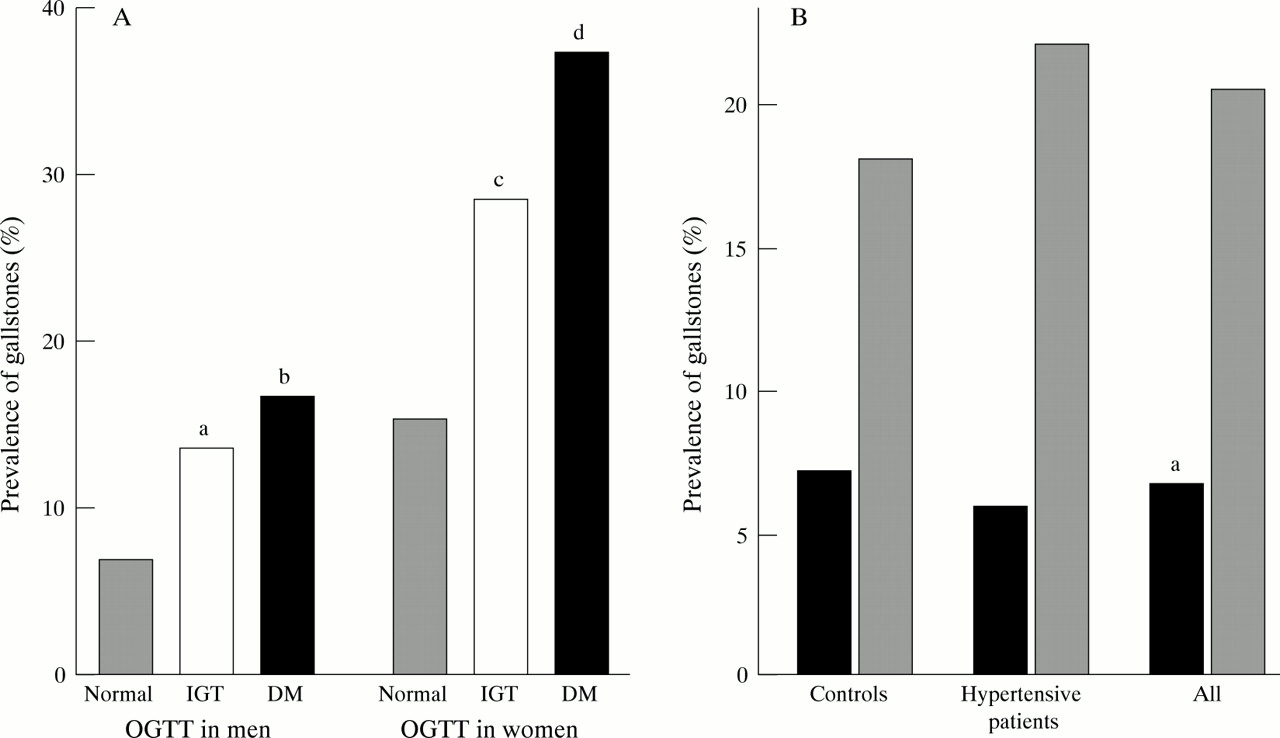
The prevalence of GSD was 9.0% in men and 19.3% in women. Among both sexes, the prevalence of GSD tended to be higher in patients with treated hypertension than in controls so that the relative risk for GSD was 1.2 (95% CI 0.8–1.7) for hypertensive women and 1.8 (1.0–3.1) for hypertensive men compared with the age and sex matched control groups. Thirty seven (24.3%) in the GSD group and 133 (14.8%) in the control group showed impaired glucose tolerance, and 25 (16.89%) in the control group and 72 (8.04%) in the control group were diabetics. The prevalence of GSD was significantly higher in diabetics than in the normoglycaemic group in both sexes (37.2% versus 15.2% for women, respectively, odds ratio (OR) 3.29, 95% CI 1.67–6.47; and 16.7% versus 7.0% for men, OR 2.65, 95% CI 1.17–5.99) (fig 1A). The prevalence of GSD was also higher in the impaired glucose tolerance group than in the normoglycaemic group (24.8% versus 14.9% for women, respectively, OR 2.20, 95% CI 1.29–3.77; and 23.4% versus 14.8% for men, OR 2.08, 95% CI 0.99–4.40).
{kind=link}
(A) Prevalence of gallstone disease in normoglycaemic subjects, subjects with impaired glucose tolerance (IGT), and diabetes mellitus (DM). For (a) OR=2.08 (95% CI 0.99–4.40); (b) OR=2.65 (1.17–5.99); (c) OR=2.20 (1.29–3.77); and (d) OR=3.29 (1.67–6.47) compared with normoglycaemic subjects. (B) Prevalence of gallstone disease in control, hypertensive, and all women with at least one ε2 allele (phenotypes E2/2, 2/3, and 2/4; black bars) and without the ε2 allele (phenotypes E3/3, 4/3, and 4/4; shaded bars). For (a) OR=0.28 (95% CI 0.08–0.92).
Tables 1 and 2 show the basic characteristics, blood glucose, serum insulin, and plasma lipoprotein concentrations of subjects with and without gallstones among hypertensive and control women and men. Triglycerides were higher in subjects with GSD than in those without GSD among both control and hypertensive women. In female subjects with the highest BMI tertile (BMI over 28.6 kg/m2), the prevalence of gallstones was higher (27%) than in the lowest and middle tertiles (17% and 14%, respectively) (χ2=10.7, p<0.005). In men, the prevalence of gallstones also tended to increase along with the BMI, being 7%, 9%, and 11% in the lowest, middle, and highest tertiles, respectively.
Clinical characteristics of control and hypertensive women with and without gallstones
Clinical characteristics of control and hypertensive men with and without gallstones
Table 3 presents the apolipoprotein E phenotype distributions. In all women with at least one ε2 allele (E2/2, E2/3, and E2/4 phenotypes), the presence of gallstones (6.7%) was lower than in women without the ε2 allele (20.5%) (χ2=5.0, p<0.025). The same trend was seen among both hypertensives and controls (fig 1B). For women with the ε2 allele versus those without the ε2 allele, the OR for GSD was 0.28 (95% CI 0.08–0.92). In women with the ε2 allele, plasma cholesterol and LDL cholesterol were lower than in women without the ε2 allele (table 4). In men, no association between apo E and the presence of gallstones was observed (table 3). There were no differences in glucose and insulin concentrations or in the prevalence of diabetes between individuals with or without the ε2 allele (data not shown).
Apolipoprotein E phenotypes in controls and hypertensive patients with and without gallstones
Age, BMI, plasma total cholesterol, LDL and HDL cholesterol, and triglycerides in subjects with the ε2 allele of Apo E (phenotypes E2/2, 2/3, and 2/4) and subjects without the ε2 allele (E3/3, 4/3, and 4/4)
In the stepwise multiple logistic regression model (including two hour glucose and insulin concentrations during the OGTT, fasting blood glucose and serum insulin, apo E2 isoform, age, BMI, plasma total, LDL, and HDL cholesterol, and plasma triglycerides as variables) elucidating the risk for GSD in women, the OR was 0.28 (95% CI 0.08–0.93) for a phenotype with the E2 isoform (phenotypes E2/2, 2/3, and 2/4), 1.098 (1.02–1.17) for an elevation of 1 mmol/l in blood glucose during the two hour OGTT, 1.05 (1.02–1.07) for an elevation of 1 mU/l in serum insulin, 1.54 (1.21–1.96) for an elevation of 1 mM in serum triglycerides, and 1.05 (1.01–1.09) for one additional year of age. The most powerful and consistent predictor for GSD among women was the two hour glucose concentration during the OGTT, followed by fasting serum insulin, apo E2 isoform, serum triglycerides, and age. In men, the OR for an elevation of 1 mmol/l for blood glucose during the two hour OGTT was 1.13 (95% CI 1.05–1.22), and LDL and HDL cholesterol provided protection against GSD with ORs of 0.60 (0.42–0.85) and 0.25 (0.08–0.80), respectively. For men, the strongest predictor of GSD was the two hour blood glucose concentration during the OGTT, followed by LDL and HDL cholesterol. Apo E2 was not a significant protective factor in men.
Discussion
The present findings suggest that the ε2 allele of apolipoprotein E may protect middle aged women against the development of GSD. Impaired glucose tolerance, high plasma triglycerides, and advancing age are confirmed as risk factors for GSD in a stepwise multiple logistic regression model. In men, the risk factor profile seems to be somewhat different, as LDL and HDL cholesterol, but not the apo E isoform E2 are significant risk factors. In both men and women, GSD seems to be associated with impaired glucose metabolism, obesity, and hypertension. It is notable that the prevalence of GSD in men was less than half of that in women, and a larger population of men would possibly have been needed to assess all the risk factors for GSD.
According to the present findings on the control (non-hypertensive) subjects, the prevalence of GSD is 17.6% in Finnish middle aged women and 6.6% in men. The prevalence of GSD in a neighbouring white population in Sweden has recently been reported to be 11% and 25% in women aged 40 and 60 years, respectively, and 4% and 15% in men3; this prevalence is quite similar to that observed in the present study.
Previous studies on the relation between clinical GSD and blood pressure have been negative.8 However, the present study suggests that ultrasonographically detected GSD may be more prevalent in hypertensive subjects, at least in men. Obesity is an established risk factor for hypertension and GSD, and might thus be a factor explaining this association.
Of the classic risk factors in women, age and triglycerides were significant in the multiple stepwise logistic regression model, even though age ranged only between 40 and 60 years. Unfortunately, we were unable to analyse the subjects with cholesterol and pigment gallstones separately, because it is unethical to perform cholecystectomies on non-symptomatic subjects. The risk factors for the different types of GSD are different,1 ,26 but cholesterol gallstones are overwhelmingly the most prevalent gallstones (74%) in our population.17 In accordance with the previous reports,1-5 we found obesity to be an important risk factor for GSD. In men, HDL and LDL cholesterol were negatively associated with the risk for GSD. An association between low HDL and GSD has been observed, especially in women,6-8 but the relation between LDL cholesterol and GSD has been weaker.6The classic risk factors were included in this study to estimate the relative power of new risk factors. As all the classic risk factors seemed to be important in our analysis, we believe that our population based sample is not biased by any means and is suitable for the search for potential new risk factors.
Previous studies have revealed significant genetic components in biliary cholesterol saturation27 and biliary lipid composition,28 both of which are affected by apo E.15 ,18 The present and previous18 data suggest that the apo E phenotype belongs to the shared genetic factors influencing cholesterol metabolism and the susceptibility to GSD. A recent analysis of the variations in other genes affecting lipoprotein metabolism, such as the genes for apo B, apo A-I, and CETP, did not establish significant associations between a number of DNA polymorphisms of these genes and GSD.29
The prevalence of GSD tended to be higher in the hypertensive than in the control subjects. In the San Antonio Heart Study,8where the diagnosis of GSD was based on self reporting, the adjusted odds ratio for GSD was 1.16 in hypertensive women and 1.25 in hypertensive men, showing the same trend as in our study. Does hypertension render subjects more prone to GSD? Our hypertensive subjects had higher BMIs and triglyceride, glucose, and insulin concentrations than the control group, showing the classic risk factor cluster known as the metabolic syndrome. All of these risk factors for coronary heart disease also seem to be risk factors for GSD according to the present and previous studies.1-4 ,9 Some inpatient studies on the association of GSD have been controversial,30 ,31 but our results are in agreement with earlier epidemiological studies on self reported, clinical gall bladder disease.8 In addition, the earlier findings on the association between hyperinsulinaemia and GSD are further expanded.32 Furthermore, environmental factors, such as a diet leading to abnormalities in cholesterol and bile acid metabolism and excess weight, may also render subjects susceptible simultaneously to impaired glucose metabolism, hypertension, and GSD.
According to the present data, the E2 isoform seems to provide protection against GSD in women. In our previous study on patients with symptomatic GSD, the prevalence of the E2 isoform was 9.5% versus 8.5% in patients versus controls, respectively. In another previous study,18 the prevalence of E2 also tended to be even slightly higher in female (9.6%) and male (10.9%) gallstone patients than in female (7.3%) and male (7.0%) controls. The E4 isoform was not overrepresented in the present patients with GSD, whereas it was clearly overrepresented in the GSD patients in another study.18 It is possible that in studies on selected symptomatic patients,17 ,18 the distribution of apo E phenotypes may be different from that in a randomly selected population.
How might the ε2 allele protect against GSD? Supersaturation of gall bladder bile with cholesterol is a precondition for crystallisation.33 ,34 Lithogenic bile may be a result of enhanced cholesterol synthesis, a reduced bile acid pool, or both.35 ,36 The protective effect of ε2 may lie in the metabolic pathways leading to supersaturation, as subjects with the ε2 allele show low cholesterol absorption and a high rate of bile salt synthesis.14 Furthermore, the nucleation time of gall bladder bile is suggested to be long in subjects with the ε2 and ε3 alleles and short in subjects with the ε4 allele,17although this effect has not been observed in all studies.18 Apo E, which is present in gall bladder bile,17 may also act as a nucleating or antinucleating factor itself. For example, apo E binds to monosodium urate crystals37 and promotes polymerisation of the 42 amino acid amyloid β peptide.38 Apo E may also interact in this way with proteins that control the nucleation of cholesterol crystals and their growth into stones.
The present findings confirm the role of the classic risk factors for GSD in a population based cohort examined by ultrasonography, and suggest that hypertension and GSD may have common genetic and environmental risk factors. The previously observed inhibitory effects of the ε2 allele of apolipoprotein E on cholesterol crystallisation17 and bile composition18 also seem to affect the risk for GSD at the population level. The data of the present work and a recent population based study9confirm that impaired glucose tolerance and diabetes may also be added to the list of risk factors for GSD.
Acknowledgments
This work was supported by the Medical Council of the Academy of Finland. The skilful technical and secretarial assistance of Ms Saija Kortetjärvi, Ms Liisa Laine, and Ms Leena Ukkola is greatly appreciated.
Abbreviations
- Apo E
- apolipoprotein E
- BMI
- body mass index
- GSD
- gallstone disease
- HDL
- high density lipoprotein
- LDL
- low density lipoprotein
- OGTT
- oral glucose tolerance test