


Abstract
Background: Cholinesterase inhibitors (ChEIs) are the only drugs marketed for the treatment of Alzheimer's disease. Despite numerous randomized controlled trials, the efficacy and safety of this group of medications has not been quantified. Our objective was to quantitatively summarize data on the efficacy and safety of ChEIs in Alzheimer's disease in a format useful to clinicians.
Methods: We performed a meta-analysis of randomized, double-blind, placebo-controlled, parallel-group trials of currently marketed ChEIs (donepezil, rivastigmine and galantamine), used in therapeutic doses for at least 12 weeks, from which a cognitive outcome was reported. Studies were identified through 3 electronic databases searched to May 2002, pharmaceutical companies and journals. We extracted the proportions of subjects who responded, experienced adverse events, discontinued treatment for any reason or discontinued treatment because of adverse events.
Results: In the 16 identified trials that met the inclusion criteria, 5159 patients were treated with a ChEI and 2795 received a placebo. The pooled mean proportion of global responders to ChEI treatment in excess of that for placebo treatment was 9% (95% confidence interval [95% CI] 6%–12%). The rates of adverse events, dropout for any reason and dropout because of adverse events were also higher among the patients receiving ChEI treatment than among those receiving placebo, the excess proportions being 8% (95% CI 5%–11%), 8% (95% CI 5%–11%) and 7% (95% CI 3%–10%), respectively. The numbers needed to treat for 1 additional patient to benefit were 7 (95% CI 6–9) for stabilization or better, 12 (95% CI 9–16) for minimal improvement or better and 42 (95% CI 26–114) for marked improvement; the number needed to treat for 1 additional patient to experience an adverse event was 12 (95% CI 10–18).
Interpretation: Treatment with ChEIs results in a modest but significant therapeutic effect and modestly but significantly higher rates of adverse events and discontinuation of treatment. The numbers needed to treat to benefit 1 additional patient are small.
Alzheimer's disease (AD) is an irreversible, progressive disorder characterized by neuronal deterioration that results in loss of cognitive functions, such as memory, communication skills, judgement and reasoning. AD is diagnosed on the basis of the development of multiple cognitive deficits (impairments of both memory and cognition at a minimum) and significant impairment of social and occupational functioning, with gradual onset, continuing decline and lack of alternative explanations (e.g., delirium, other central nervous system or psychiatric conditions, systemic diseases).1 According to the Canadian Study of Health and Aging, 1 in 20 Canadians over age 65 has AD.2 Thus, in 2001 an estimated 238 000 Canadians over 65 had AD,2 and 60 000 new cases were expected per year.3
The Canadian Consensus Conference on Dementia4,5,6 and others7 recommend cholinesterase inhibitors (ChEIs) for standard symptomatic treatment of AD. Currently 3 “second-generation” ChEIs — donepezil, galantamine and rivastigmine — are marketed in Canada for treating the cognitive symptoms of mild to moderate AD. The “first-generation” ChEIs (tacrine, velnacrine and physostigmine) had a short duration of action and lacked specificity for acetylcholinesterase.8
A number of randomized controlled trials have evaluated the efficacy and tolerability of the second-generation ChEIs,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25 reporting that 18%20 to 48%14 of treated patients improved in global measures. Aside from the wide range, response was defined with a cognitive scale that is difficult to translate into clinically meaningful information. The benefit offered by ChEIs, though statistically significant, were described as moderate at best.8,26,27,28
Meta-analysis is a statistical technique often used to quantitatively incorporate outcomes of different studies.29 Although the data from trials of individual second-generation ChEIs such as donepezil and galantamine30 have been combined, there is no report in the literature of a meta-analysis of data for all 3 medications. One analysis determined the numbers needed to treat for donepezil and rivastigmine;31 however, only 5 studies were included, tolerability was not addressed, and trials of galantamine were not yet available. A more recent meta-analysis addressed behavioural and functional outcomes only, included irrelevant ChEIs and did not calculate numbers needed to treat.32
The primary care physician is expected to communicate realistic information concerning treatment options and expectations to patients with AD and their families.5 Therefore, we performed a meta-analysis of second-generation ChEIs to quantify the therapeutic effect of these medications, estimate tolerability and calculate the number needed to treat to benefit 1 additional patient.
Methods
The population to be studied was adults with AD diagnosed on the basis of standardized criteria of the Diagnostic and Statistical Manual of Mental Disorders, 4th edition,1 or the National Institute of Neurological and Communicative Disorders and Stroke/Alzheimer's Disease and Related Disorders Association.33 Treatment included therapeutic doses for at least 12 weeks (the minimum period needed to see a treatment effect) of any of the available second-generation ChEIs. Cognitive outcomes must have been measured, on any validated scale. We accepted only original reports (not secondary publications of previously reported data) of randomized, double-blind, placebo-controlled, parallel-group clinical trials.
We searched the English-language literature, using MEDLINE and EMBASE, from January 1980 to May 2002, since the earliest publication concerning clinical use of a second-generation ChEI appeared in the 1990s.34 Key words were cholinesterase inhibitor AND Alzheimer, and the limits were randomized controlled trials, English and human. Searches were also conducted for individual ChEIs (key words donepezil, E2020 or Aricept; rivastigmine, ENA 713 or Exelon; galantamine or galanthamine; AND Alzheimer). The Cochrane databases were searched from inception. Recent review articles and published reports of clinical trials were manually cross-referenced, as were all references and bibliographies from retrieved articles.
“Differential” photocopying was used to blind raters as to authors and their location and as to date and journal of publication to reduce potential bias. First, 2 raters reviewed the Methods section of all articles identified. Articles meeting the inclusion criteria were then rated on quality by 2 raters using the Jadad scale,35 which is simple to use and has been validated.35,36,37 Disagreements regarding inclusion and quality were settled though consensus discussion.
From the Results section of the included articles 3 raters extracted the numbers of patients in the following categories: responding or not responding to treatment, reporting any adverse event, discontinuing treatment (“dropping out”) for any reason and dropping out because of adverse events. Discrepancies were managed though consensus discussion among all the reviewers.
Data relating to responders were extracted with the use of 2 definitions. Global responders were defined as subjects rated as “improved” (i.e., excluding “unchanged” but including “minimal improvement” and better) on a global assessment scale (Clinical Global Impression of Change [CGIC]38 or Clinician Interview-Based Impression of change plus caregiver input [CIBIC+]39); the intent-to-treat (ITT) population was the denominator for proportions. This meta-analysis focused on global improvement since it is an important outcome and a regulatory requirement that includes treatment effects not captured on strictly cognitive scales, and it measures clinically relevant change.28,40 Cognitive responders were defined as subjects with a 4-point or greater improvement on the Alzheimer's Disease Assessment Scale–cognitive portion (ADAS–cog);41 the ITT population was the denominator for proportions. This is the standard definition of responder, as first defined by the US Food and Drug Administration.42 The denominators for the proportions of subjects reporting any adverse event, dropping out for any reason or dropping out because of adverse events were also the ITT population. Manufacturers were contacted for data missing from the published reports.
For the main analyses, we identified the numbers of responders and nonresponders in each of the 2 groups within each study, calculated response rates for the treated patients (Rt) and placebo recipients (Rp), then calculated an effect size for each study: the difference in response rates (Di = Rt – Rp).
Outcomes (Di values) were pooled across the studies with the random-effects meta-analytic model developed by Cochran,43,44 which essentially weights each study's effect size by its sample size and by the between-study variance. This model yields a pooled mean point estimate and a 95% confidence interval (95% CI). Thus, it generally creates wider confidence intervals than other methods.45 However, because it incorporates between-study differences, it tends to mitigate discrepant results when there is a great deal of variation. Such variation is to be expected because of the wide variations found in this disease and in its response to treatment.
This procedure was followed for global response, cognitive response and other outcomes of interest, which included adverse events, dropout for any reason and dropout because of adverse events. For this research, adverse events were defined as any adverse event that emerged during treatment, as reported by the original authors.
To evaluate publication bias, we generated a funnel plot comparing effect size with sample size46 and evaluated the results with the Begg and Mazumdar adjusted rank correlation test.47
The number needed to treat (NNT) and the number needed to harm (NNH) were calculated according to the method of Cook and Sackett.48 The NNT is the reciprocal of the risk difference when the outcome is positive, and the NNH is the reciprocal of the risk difference when the outcome is negative. NNTs were based on the proportion of global responders and NNHs on the proportion of patients reporting adverse events. For studies in which the difference between treatment groups is not statistically significant, CIs may cross zero and, as such, are difficult to characterize; we used the method described by Altman49 to overcome this difficulty.
We performed subanalyses to assess the impact of ethnicity (Asian v. predominantly white patients), dose, drug, duration of treatment and CGIC definition. Compared with white patients, the Japanese require lower doses of many psychotherapeutic medications50 and may have a higher rate of response to ChEI therapy.14 Dosages were grouped according to common prescribing practice or analysis of the literature, or both, as follows: subtherapeutic (donepezil, 1 to 3 mg/d; galantamine, 8 mg/d), low (donepezil, 5 mg/d; rivastigmine, 3 to 6 mg/d), high (donepezil, 10 mg/d; galantamine, 16 to 24 mg/d; rivastigmine, 9 to 12 mg/d) or above that recommended (galantamine, 32 mg/d); low-dose and high-dose groups were compared. Studies were grouped by duration of treatment, with shorter term defined as 12 to 14 weeks and longer term as 24 to 52 weeks. The ChEIs were also grouped by definition of CGIC. The CGIC scale indicates degrees of change from baseline as follows: 1, marked improvement; 2, moderate improvement; 3, minor improvement; and 4, no change. Thus, CGIC1–4 includes no change and CGIC1–2 is the strictest definition.
Results
Of the 40 articles identified in the literature searches, 2425,34,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72 were excluded for the following reasons: the article was not an original report of a clinical trial (n = 6); the trial was not randomized (n = 3), not double-blind (n = 5), not of parallel (crossover) design (n = 5) or not placebo-controlled (n = 5); treatment lasted less than 12 weeks (n = 4); there was no measurement of cognitive outcome (n = 3); and subjects did not have AD (n = 7). The remaining 16 studies met the inclusion criteria9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24 (Table 1). All 16 studies had a Jadad quality score greater than 3; the median score was 5. These studies examined ChEI therapy in 5159 subjects and placebo treatment in 2795 subjects.
Table 1.
Efficacy
The proportion of global responders could be extracted from 9 studies,10,11,12,14,18,20,21,23,24 involving 4468 subjects of either predominantly white (8 studies) or Japanese (1 study) patients. Heterogeneity among the studies was statistically significant (𝛘2= 23.8, p = 0.002); the study by Homma and colleagues14 was by far the greatest contributor to the heterogeneity and was the only study done exclusively on Japanese patients. Thus, a subanalysis was performed on the white-patient-based studies, which involved 4205 subjects and were not heterogeneous (Table 2).
Table 2.
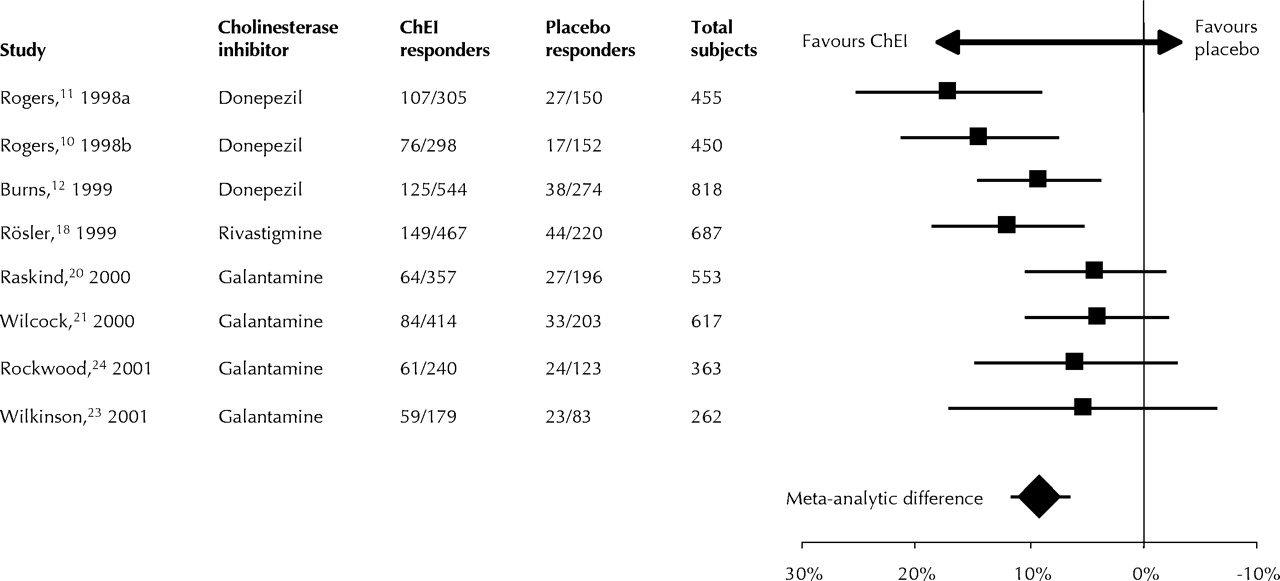
The pooled mean proportion of global responders to ChEI treatment in excess of that for placebo treatment in the 8 studies was 9% (95% CI6%–12%) (Table 2). Fig. 1 shows the contribution of individual studies. A funnel plot indicated no relationship between sample size and effect size.

Fig. 1: Global response to treatment with cholinesterase inhibitors (ChEIs) in 8 randomized, double-blind, placebo-controlled, parallel-group trials. The graph indicates the proportions of global responders to ChEI treatment in excess of the proportions responding to placebo for each of the studies and overall, when the data were pooled, with 95% confidence intervals.
The proportion of cognitive responders could be extracted from 5 studies,10,18,21,23,24 involving 2419 subjects. The pooled mean proportion of cognitive responders to ChEI treatment in excess of that for placebo treatment was 10% (95% CI 4%–17%) (Table 2). The studies were heterogeneous in this analysis, but when the study by Rösler and associates,18 which compared high- and low-dose rivastigmine and found a low proportion of ChEI responders (19%), was excluded, the studies were not heterogeneous (𝛘2= 4.2, p = 0.24); pooling the data from the remaining 4 studies showed a therapeutic effect of 14% (95% CI 8%–18%). There was no obvious reason in the way the Rösler study was designed or conducted for a lower rate of response; furthermore, the global response was not different from that in the other studies. Thus, the heterogeneity remains unexplained.
Safety
The proportion of subjects in whom any adverse event emerged during treatment could be extracted from 14 studies.9,10,12,13,14,15,16,17,18,20,21,22,23,24 Compared with those receiving placebo, significantly more subjects receiving ChEI treatment had adverse events (8%), dropped out (8%) and dropped out because of adverse events (7%) (Table 2). There was significant heterogeneity among the studies in all 3 analyses, perhaps because of different titration schedules, protocol differences or simply random variation.
Numbers needed to treat/harm
The number of patients who needed to be treated with a ChEI compared with placebo in order that 1 additional patient demonstrate a global response was found to be 12 (95% CI 9–16) when the studies of non-Asian patients were analyzed and 4 (95% CI 3–6) in the Japanese study. For cognitive response the NNT was 10 (95% CI 8–15). The number needed to harm 1 additional patient (cause adverse events) was 12 (95% CI 10–18).
Analysis by drug
For donepezil (3 studies; 1147 subjects treated with the ChEI and 576 treated with placebo) and galantamine (4 studies; 1190 and 605 subjects, respectively) the excess pooled mean proportions of global responders were 13% (95% CI 8%–17%) and 5% (95% CI 1%–8%), respectively. The NNTs were 8 (95% CI 6–12) and 22 (95% CI 12–157), respectively. The treatment effect was significant for both drugs. The single study of rivastigmine indicated an excess proportion of 12% (95% CI 5%–19%).
Dropout rates in excess of those for placebo were lowest for donepezil (3%; 95% CI 1%–6%), followed by rivastigmine (9%; 95% CI 5%–12%) and then galantamine (14%; 95% CI 8%–21%; 𝛘2 = 17.6, p = 0.001 for heterogeneity). This trend was repeated for adverse events, the excess rates being donepezil 6% (95% CI 2%–9%), rivastigmine 8% (95% CI 1%–10%) and galantamine 12% (95% CI 7%–18%; 𝛘2 = 12.1, p = 0.01), and for dropouts due to adverse events, the excess rates being donepezil 2% (95% CI -1%–4%; 𝛘2 = 14.0, p = 0.05), rivastigmine 9% (95% CI 6%–12%) and galantamine 14% (95% CI 5%–22%). Only the results for galantamine consistently showed heterogeneity, possibly owing to the use of higher-than-recommended doses in some studies.
Analysis by dose
For global responders, meta-analysis revealed comparable results for low and high ChEI doses, with an excess proportion of 8% for low doses (95% CI 5%–12%; 7 studies, in which 1348 subjects were treated with a ChEI and 1140 with placebo) and 11% for high doses (95% CI 7%–15%; 10 studies, with 1816 and 1739 subjects, respectively), both significantly better than the results with placebo (p < 0.001). However, the studies with high ChEI doses showed unexplained heterogeneity (𝛘2 = 22.1, p < 0.01).
Analysis by duration of treatment
The excess proportion of global responders was similar after short-term ChEI treatment (11%; 95% CI 5%–16%; 3 studies, in which 724 subjects were treated with a ChEI and 356 with placebo; 𝛘2 = 19.3, p < 0.001) and long-term ChEI treatment (9%; 95% CI 5%–12%; 5 studies, with 2080 and 1045 subjects, respectively; 𝛘2 = 7.4, p = 0.12), although only the long-term trials showed no heterogeneity.
Analysis by CGIC definition
When the ChEIs were grouped by increasing degree of global improvement, the excess proportions of responsive subjects were 15% for stability or improvement (p < 0.001, 95% CI 11%–18%; 7 studies, in which 2076 subjects were treated with a ChEI and 1052 with placebo), 9% for any improvement (p < 0.001; Table 2) and 2% for greater than minimal improvement (p = 0.04, 95% CI 1%–4%; 3 studies, with 1001 and 522 subjects, respectively). There was no significant heterogeneity. The corresponding NNTs were 7 (95% CI 6–9), 12 (95% CI 9–16) and 42 (95% CI 26–114).
Interpretation
This meta-analysis confirmed that AD patients treated with ChEIs demonstrate statistically significant global improvement compared with those treated with placebo, supporting current guidelines advocating treatment.4,5,6,7 At 9%, the therapeutic benefit is consistent with the modest benefits described in previous qualitative reviews.8,26,27,28 The NNT of 12 for 1 additional patient to demonstrate a global response is similar to NNTs previously calculated for AD.31 By comparison, reported NNTs are 3 for antipsychotics in schizophrenia,73,74 4 for antidepressants for depression in medical illness75 and 29 to 86 (5-year NNT) for antihypertensives to prevent 1 major event (myocardial infarction, stroke or death).76
The definition of treatment response had an important impact. Although minimal improvement or better was the definition in the main analysis, many authors use stabilization as the definition in studies lasting 6 months or more.16,19,20 Our results confirm that ChEI treatment is associated with significantly better global improvement than placebo treatment for all 3 definitions of response (stabilization or better, minimal improvement or better, marked improvement).
Tolerability of ChEIs is an important consideration when evaluating their place in therapy. The proportion of patients in whom adverse events emerged during treatment was only 8% higher in those receiving ChEIs than in those receiving placebo, which shows that these medications are well tolerated. The adverse events were mostly gastrointestinal, and no related deaths were reported. The rates of dropout and dropout due to adverse events were higher with ChEIs than with placebo (8% and 7%, respectively). The rates seen in clinical practice should be lower when dosage is tailored to the individual.
The study of Homma and colleagues14 detected a very large treatment effect (28%) in a Japanese population receiving low-dose donepezil, which suggests ethnic differences. A lower frequency of the ε4 gene of apolipoprotein E77 and differences in major enzymes that metabolize ChEIs, such as cytochrome P450 2D6,78 in the Japanese may explain this finding. Although no conclusion can be reached on the basis of a single study, our findings support earlier descriptions of purported differences.14
Subanalyses of the data for individual ChEIs indicated similar efficacy but differences in tolerability. The excess proportions of subjects who dropped out for any reason and who dropped out because of adverse events were lowest for donepezil and highest for galantamine. A similar trend was found for overall proportions reporting adverse events. These results must be interpreted with caution, as they were derived from a small number of trials for each medication and were based on a comparison of independent placebo-controlled trials; that is, they were not analyses of head-to-head trials (single trials with random allocation to different ChEIs). When comparing efficacy one must bear in mind that the interrater reliability of global assessment scales may be less well established than that for cognitive measures,40 and the scales used for global assessment may have different psychometric properties. Differences in tolerability may reflect differences in aspects of study design such as rate of titration or use of galantamine in a dose that is not recommended clinically (32 mg/d), which may not translate to the clinical setting, where doses are determined for the individual.
Although the second-generation ChEIs share the ability to inhibit acetylcholinesterase, their pharmacologic variations may distinguish them. Donepezil inhibits acetylcholinesterase but not butyrylcholinesterase;79 the latter is thought to be a component of neuritic plaques and tangles,80,81 the pathological hallmarks of AD. Rivastigmine has central selectivity82 and inhibits both acetylcholinesterase and butyrylcholinesterase.83 Galantamine is unique in that it provides allosteric modulation of nicotinic receptors,84,85,86 a characteristic postulated to confer disease-modifying benefits.86 Preliminary head-to-head trials indicate a slightly greater response to donepezil than to galantamine87 and similar efficacy for donepezil and rivastigmine.88 Those trials also indicate better tolerability of donepezil than of both galantamine87 and rivastigmine.88 Unfortunately, important issues such as open-label design, dose of the comparator and titration rate may account for those results. Nevertheless, our findings were consistent with the findings of those trials.
Our subanalyses indicated similar response to all 3 drugs when studies were grouped by dose or by duration of treatment. Lack of a dose effect could reflect near-maximal cholinesterase inhibition or be the product of an ITT analysis. In such an analysis, if more patients on high doses drop out of the study before responding, the treatment effect will be diluted.89 In addition, since in AD there is deterioration over time, when the last observation for a subject who dropped out is carried forward, the apparent benefit may be false. The lack of an effect of duration of treatment may reflect the fact that these studies were carried out within a relatively narrow time frame (3 to 12 months). Small numbers and heterogeneity limit the ability to draw meaningful conclusions from these subanalyses.
Meta-analyses may suffer from publication bias, since studies with a statistically positive result are more likely to be published than those with a negative result, resulting in an overestimate of treatment efficacy. In this study, there was no significant relationship between effect size and sample size. However, there may be negative studies with small samples that were not published. In addition, since the overall ChEI differences over placebo were not heterogeneous, the studies were summarized by single NNT and NNH estimates, with 95% CIs. Since the control rates in the included studies were heterogeneous, a range of NNTs and NNHs may exist for specific patient groups.90
Overall, the results of this meta-analysis indicate that ChEI therapy in AD is efficacious compared with placebo therapy. In addition, few patients need to be treated to achieve global improvement in 1 more patient and even fewer to achieve stabilization. For future studies, defining treatment response to ChEIs on the basis of clinically important outcomes, such as delay to institutionalization, maintenance of activities of daily living and reduced caregiver burden,40 will clarify the benefits of these medications.
Footnotes
-
This article has been peer reviewed.
Contributors: Drs. Lanctôt and Herrmann conceived and designed the study and contributed substantially to the acquisition, analysis and interpretation of data. Mr. Yau contributed substantially to the acquisition and interpretation of data. Ms. Khan, Dr. Liu and Ms. LouLou contributed substantially to the acquisition of data. Dr. Einarson contributed substantially to the analysis and interpretation of data. All authors drafted or revised the article critically for important intellectual content and gave final approval of the version to be published.
Competing interests: Dr. Lanctôt received research honoraria and/or speaker fees and/or travel assistance from Pfizer, Janssen-Ortho and Neotherapeutics; Dr. Herrmann received research honoraria and/or speaker fees and/or travel assistance from Pfizer, Novartis and Janssen-Ortho; Mr. Yau is currently employed by AstraZeneca Canada; Dr. Liu has received education grants for conferences from Pfizer, Janssen-Ortho and Novartis; Ms. LouLou is currently employed by Merck Sharpe Dohme, Abu Dhabi, United Arab Emirates.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
In this issue
{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- Long-Known Music Exposure Effects on Brain Imaging and Cognition in Early-Stage Cognitive Decline: A Pilot Study
- New Galantamine Derivatives with Inhibitory Effect on Acetylcholinesterase Activity
- Risks and benefits of unapproved disease-modifying treatments for neurodegenerative disease
- Neurotransmitter imbalance in the brain and Alzheimers pathology
- Alzheimer dementia: Starting, stopping drug therapy
- Drugs for Dementia and Excess of Hospitalization: A Longitudinal French Study
- Risk of pneumonia associated with incident benzodiazepine use among community-dwelling adults with Alzheimer disease
- Unraveling Alzheimers: Making Sense of the Relationship between Diabetes and Alzheimers Disease
- Prescribing drugs for Alzheimer's disease in primary care: managing cognitive symptoms
- Rivastigmine for HIV-associated neurocognitive disorders: A randomized crossover pilot study
- Guidelines for the Management of Cognitive and Behavioral Problems in Dementia
- Effect of treatment gaps in elderly patients with dementia treated with cholinesterase inhibitors
- Restoration of Norepinephrine-Modulated Contextual Memory in a Mouse Model of Down Syndrome
- Cholinergic Stimulation Enhances Neural Activity Associated with Encoding but Reduces Neural Activity Associated with Retrieval in Humans
- Treatment of Alzheimer's disease in the long-term-care setting
- Diagnosis and treatment of dementia: 5. Nonpharmacologic and pharmacologic therapy for mild to moderate dementia
- Does analysis using "last observation carried forward" introduce bias in dementia research?
- Sufficiently Important Difference for Common Cold: Severity Reduction
- Questioning the evidence.
- Nonpatentable drugs and the cost of our ignorance
- Cholinesterase inhibitor use in geriatric outpatients with dementia
- Rivastigmine modestly improves dementia associated with Parkinson's disease, but has important adverse effects
- Are there long-term benefits of donepezil in Alzheimer's disease?
- Donepezil did not reduce the rate of institutionalisation or disability in people with mild to moderate Alzheimer's disease
- Drug therapy for Alzheimer's disease
- Drug therapy for Alzheimer's disease
- Drug therapy for Alzheimer's disease
- Smaller trials for better evidence
- Donepezil is somewhat effective for Alzheimer's, probably better than galantamine
More in this TOC Section
Similar Articles

