





Abstract
Airways resistance measured by the interrupter technique (Rint) requires little patient cooperation and has been successfully used in young children, but little studied in infants. The authors aimed to evaluate the measurement of Rint in infants, using a commercially available device (the MicroRint), by comparing it with an established technique to measure respiratory resistance: the single breath occlusion technique (SBT); and a measure of airflow obstruction during forced expiration.
Infants <18 months old with a history of wheeze, sedated with triclofos for pulmonary function testing, had measurements taken and compared to Rint (using the MicroRint), respiratory system resistance (Rrs) by SBT, and to maximal flow at functional residual capacity (V′maxFRC).
Paired data from 25 of 37 infants studied was obtained. There was a significant difference between Rint (mean 2.94±0.68) and Rrs (4.02±0.87), but the two measures were strongly correlated (r=0.7). Rint was negatively correlated with V′maxFRC (r=−0.63). Smaller infants failed to trigger the MicroRint.
Interrupter resistance values in infants are significantly lower than values of respiratory system resistance obtained by passive mechanics. However, there is a strong correlation between the two measurements, as well as between resistance measured using the interrupter technique and maximal flow at functional residual capacity, which indicates that resistance measured using the interrupter technique may be a useful marker of airway obstruction in infants. There remain a number of theoretical and technical problems which require further exploration.
- Chest wall mechanics
- infant
- interrupter technique
- interrupter resistance in infants
- lung mechanics
- passive mechanics
Respiratory disorders form a major part of infant morbidity. Monitoring the progression of a condition, the response to treatment or the requirement to change therapy is usually based on subjective observation or indirect measurement. Measuring pulmonary function may give further objective evidence on which to base clinical decisions. Conventional measures of pulmonary function in infants remain complex procedures. The requirement for sedation and the duration of the tests have limited the use of most to research purposes only.
The interrupter technique is not new: it was first described in 1927 by von Neergaard and Wirz 1, and further evaluated in 1954 by Mead and Whittenberger 2. The principle is simple: airflow is briefly occluded during inspiration or expiration, and measured pressure at the mouth (Pao) equilibrates with alveolar pressure (PA). This initial rapid change in Pao (ΔPinit), an estimate of driving pressure across the airways, is divided by flow immediately before (or after) the occlusion to give a measure of airflow resistance termed interrupter resistance (Rint). Unfortunately, pressure oscillations immediately after airway occlusion make it impossible to measure ΔPinit directly, and it is also necessary for valve closure to occur very rapidly. Because of such theoretical and technical concerns, the method was mostly neglected from the 1950s until the 1980s, when these concerns were addressed in a series of papers by Bates and coworkers 3–7; and studies exploring clinical potential have followed 8–12.
The technique requires no active subject cooperation as the measurements are made during quiet tidal breathing: it is, therefore, particularly suitable for young children, and the recent published clinical studies reflect this interest. Perhaps surprisingly, there has been little previous work in infants.
The MicroRint (Micro Medical, Rochester, Kent, UK) is a commercially available device that has been developed to measure Rint, based on a prototype reported by Chowienczyk et al. 8, 13. It is marketed for use in all age ranges from neonates to adults. Its use has been well documented in preschool children 12, 14. The authors investigated whether this device could also be used, and produce meaningful results, in young infants. They aimed to do this by comparing measurements of Rint with measurements of respiratory system resistance (Rrs) obtained by the widely-used single breath occlusion technique (SBT) 15.
Methods
Infants (n=34) with a history of recurrent or persistent wheeze had pulmonary function tests performed as part of a larger study into bronchodilator response. All infants had been reported by parents to have either persistent wheeze for ≥6 weeks, or at least three episodes of wheeze over 3 months, and all had a family or personal history of atopy. Their characteristics are summarized in table 1⇓. The pulmonary function tests were performed when the infants were asymptomatic or had only mild symptoms.
Infant characteristics
The infants were sedated with 100–120 mg·kg−1 triclofos sodium syrup. Once asleep they were laid supine on a cot with a neck roll. A semirigid, transparent silicon facemask (Size 2; Pari, Starnberg, Germany) was placed over their mouth and nose with therapeutic putty (Carters, Wiltshire, UK) used to form an airtight seal. Measurements were made when the infants were in quiet sleep, as judged by a regular respiratory rate, stable end-expiratory volume, and no obvious eye movements. Oxygenation was monitored continuously by pulse oximetry.
The order of testing was: SBT; rapid thoracoabdominal compression technique (RTC); interrupter resistance (IR). For the SBT and RTC measurements, a pneumotachograph (series 3500; Hans Rudolph Inc., Kansas City, Mo, USA) was attached to the mask. Airflow and mouth pressure were measured by Validyne transducers (Validyne MP45, Validyne Corp., Miltipas, CA, USA) and the data was then digitized and recorded by RASP (PhysioLogic Ltd, Newbury, Berks, UK). The IR measurements were carried out after the other procedures to avoid unnecessary disturbance to the infant, due to the need to change between pneumotachograph and the MicroRint apparatus.
Rrs and respiratory system compliance (Crs) were measured using the SBT. This technique and analysis of data is well described elsewhere 15. Briefly, airway occlusions were made at end-inspiration to induce a Hering-Breuer reflex, then released: the resulting Pao plateau and relaxed expiration were analysed to derive Crs, the respiratory system time constant, and hence Rrs. The mean Rrs from the five most technically satisfactory occlusions were used, with a minimum correlation coefficient of ≥0.995 over at least 40% of the expiratory flow/volume trace. Up to 20 manual occlusions were performed to obtain technically satisfactory data suitable for analysis.
Partial forced expiratory flow measurements were performed by RTC, with the mean maximal flow at functional residual capacity (V′maxFRC) taken from three technically acceptable manoeuvres as described previously 16.
Once this data had been collected, the pneumotachograph was disconnected and the MicroRint connected to the face mask. The cheeks were supported and the airway was manually supported by a chin lift technique to optimize airway patency. The MicroRint apparatus incorporates a screen pneumotachograph, a piezo-resistive transducer, and an oval shutter pivoted about its short axis, placed distal to the pneumotachograph and transducer ports. The shutter is actively rotated about its short axis to close the airway for a duration of 100 ms then actively rotated to reopen the airway. The time for shutter closure (and opening) to take place is 5–6 ms 17, which satisfies the criteria established by Bates et al. 7. The device also incorporates a microcomputer, which controls the shutter, samples the flow and pressure data at 100 Hz, and performs the analysis. ΔPinit is estimated by two-point linear regression from mean pressure readings over 10-ms intervals, centred at 30 ms and 70 ms into the occlusion. This regression line is back extrapolated to the point of complete occlusion. Complete occlusion is defined as the time at which 25% of the peak of the first oscillation pressure upstroke is reached.
The device can be set to occlude in inspiration or expiration, at a preset flow or at peak flow. The authors opted to occlude during expiration at a flow of 100 mL·s−1. This was the minimum fixed flow available for triggering from the MicroRint software, and this option was elected rather than triggering at peak flow to avoid variability due to flow dependence of resistance. Expiratory occlusion was chosen to be more comparable with the SBT, which measures resistance during expiration. The median Rint was calculated automatically by the device software from five consecutive satisfactory occlusions.
Analysis
Rint was compared with Rrs and with V′maxFRC by correlation. Paired t-tests and Bland-Altman analysis 18 were also performed to compare Rint with Rrs. Characteristics of the infants in whom Rint was successfully measured were compared with the measurement failure group by unpaired t-tests and confidence interval analysis, except for V′maxFRC, which was non-normally distributed and compared by the Mann-Whitney U-test.
Results
The infants (n=37) were studied over a 1-yr period. The authors obtained 25 sets of paired data for Rint and Rrs. In 11 patients the MicroRint failed to occlude and in one patient Rrs could not be calculated due to the alinearity of the flow/volume trace. Paired data for Rint and V′maxFRC were obtained in 21 infants.
The infants in whom there was a failure to obtain values for Rint were younger, shorter and had lower peak tidal expiratory flow values compared to those in whom successful values were obtained (table 1⇑). They did not have more airway obstruction as gauged by Rrs or V′maxFRC. Although their peak tidal flows were significantly lower, the majority still had flows exceeding the target value of 100 mL·s−1 yet failed to trigger the MicroRint.
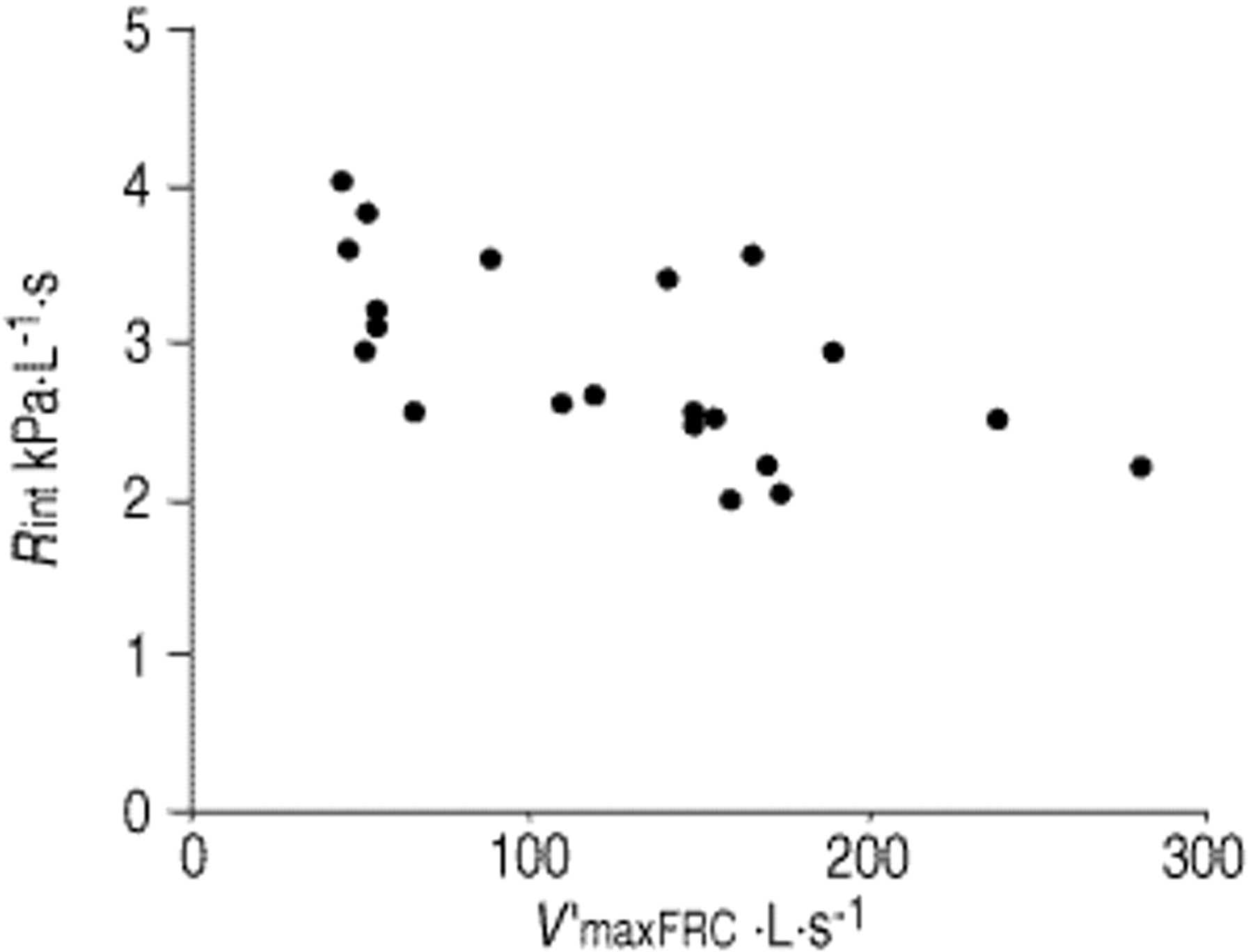
For the 25 infants with paired data, mean±sd Rint was 2.94±0.68 kPa·L·s−1, and was substantially lower than Rrs at 4.02±0.87 kPa·L·s−1. However, there was a strong correlation between the two measurements (fig. 1⇓) with a correlation coefficient of 0.7 (p<0.01). The Bland-Altman plot (fig. 2⇓) demonstrates the bias, with all the Rint values being lower than the corresponding Rrs. There was also a strong (negative) correlation between Rint and V′maxFRC (fig. 3⇓) with a coefficient of 0.63 (p<0.01) in the 21 infants with paired data.

Correlation of airways resistance measured by the single breath occlusion technique and interrupter technique (Rint). Rrs: respiratory system resistance. r=0.70.

Bland-Altman plot. Rint: interrupter technique; Rrs: respiratory system resistance. -----: mean difference −1.08 kPa·L−1·s; ═: limits of agreement i.e. mean±sd, −2.31±0.16.

{kind=link}
{kind=link}
{kind=link}
Interrupter technique (Rint) correlation with maximal flow at functional residual capacity (V′maxFRC). R=0.63.
Discussion
It has been demonstrated that, in sedated infants with a history of recurrent wheeze, respiratory resistance measured by Rint with a commercially available device shows a strong correlation with two other widely-used measures of airway narrowing: Rrs and V′maxFRC. This suggests that the technique may be capable of giving a meaningful indication of airflow resistance in infants. However, the values obtained for Rint were markedly lower than for Rrs. This is not entirely surprising in view of what is known firstly about the physiology of the two techniques, and secondly about their respective assumptions and sources of error.
Rrs, as measured by single breath passive mechanics, gives a measure of resistance to airflow of the entire respiratory system during expiration: i.e. airways, lung tissue and chest wall. It is obtained indirectly from calculating compliance and the time constant of the respiratory system, and carries the assumptions of absent respiratory muscle activity and a single compartment model, with a single resistance value applicable over the range of the expiration 15.
Conversely, Rint gives a measure of resistance to airflow at one point during (in this study) expiration, and hence at the particular volume and flow at which occlusion occurred. It does not assume muscle relaxation nor a single value for resistance independent of flow and volume. The precise components of the respiratory system which contribute to Rint remain controversial, have been extensively reviewed by Bates and Milic-Emili 19, and will depend on exactly how the pressure change used to calculate Rint is estimated.
The pressure changes occurring after airflow interruption can be divided into three phases: a rapid rise (ΔPinit), a series of damped oscillations masking the transition, and a slower rise (ΔPdif). ΔPinit is caused by equilibration between Pao and PA, and if it could be measured directly (impossible due to the oscillations), Rint calculated from this would correspond very closely to pure airway resistance 3, possibly with a small component from chest wall resistance 4. Hence, even without sources of error; Rint would be expected to be lower than Rrs, which includes airway, tissue and chest wall resistance. ΔPdif, on the other hand, is a result of the visco-elastic behaviour of lung tissues and, in disease, “pendelluft” from equilibration between disparate lung compartments 20. The greater the component of ΔPdif which is incorporated into Rint measurement, the more Rint might be expected to approach Rrs. When Rint has been compared to airway resistance (Raw, measured by body plethysmography) in adults and older children, it has again correlated strongly, but been higher than Raw 8, 10. This may be because of an added chest wall element in ΔPinit and/or because of incorporation of an element of ΔPdif, as well as ΔPinit, in the calculation of Rint.
The two main sources of inaccuracy in Rint measurements are: insufficiently rapid airway occlusion, and inaccurate estimation of ΔPinit. The first is a problem because airflow is measured before valve closure, but pressure afterwards. If during the time the valve takes to close fully, significant airflow in relation to lung volume occurs, the pressure change will not accurately reflect the driving pressure which existed at the time flow was measured. The MicroRint shutter meets the criteria suggested by Bates et al. 7 in this regard, and therefore, would not be expected to be a serious source of error in these measurements. Accurate estimation of ΔPinit remains a major problem. The linear back-extrapolation used by the MicroRint is acceptable provided that ΔPdif follows a linear trajectory: the more curvilinear or irregular it becomes, the more inaccurate the estimation. The direction and magnitude of the error will depend on the nature of the curve and the points chosen to back-extrapolate. The MicroRint (unlike an earlier prototype) does not give the option to visually inspect the pressure waveform before accepting a result. Other approaches suggested have included: curvilinear back-extrapolation 6, or taking the pressure at a set time after occlusion and accepting that this includes part of ΔPdif as well as ΔPinit 17. This latter approach is the one taken by the other current commercially available Rint system (Masterscreen Rocc, Jaeger, Hoechberg, Germany) which calculates Rint from the pressure just before release of occlusion (i.e. 100 ms after flow interruption).
The other important issue in discussing the results is that of upper airway compliance. Infants have relatively large and compliant upper airways, and with the present experimental setup, “upper airway” includes the face mask. The effect of airway compliance is both to reduce ΔPinit (and hence reduce calculated Rint) and to blur the distinction between ΔPinit and ΔPdif (and hence add a further inaccuracy to estimating ΔPinit) 19. These effects are more marked in the presence of high airway resistance and low lung volumes, as found in infants particularly with airway disease 21.
In summary, Rint as measured by the MicroRint device in infants is closely related to other measures of airway obstruction commonly used in infants, but is consistently and substantially lower than Rrs. Likely reasons for this difference are: the different components of the respiratory system which contribute, the effect of upper airway compliance, errors in the estimation of ΔPinit, and errors and unjustified assumptions in the SBT for measuring Rrs. These sources of error in both techniques probably explain why the correlation demonstrated between Rint and Rrs was somewhat less good than that previously reported between Rint and Raw in adults and older children 8, 10. The results also demonstrate the difficulty of using a preset flow value for triggering in small infants whose maximal flows may barely exceed this value. The Rint appears promising, but requires further assessment in infants, before it can be recommended for widespread use, either as a clinical or research tool.
The device studied is not suitable in its present form to study very small infants or those with very low peak tidal flows due to lung disease. Apart from the concerns discussed earlier, this study did not address the issue of reproducibility, though this has been looked at in preschool children 12. It is also unclear whether measurements are best made in inspiration or expiration 14, whether occlusion should be triggered at a preset flow, peak flow or some other standard, and what type (if any) of back-extrapolation of mouth pressure is optimal 17. Finally, and perhaps most critically, the measurements were made under optimal conditions in sedated infants, yet the most likely niche for the interrupter technique would seem to be as a “quick and easy” measure of airway obstruction at the cotside in clinical and epidemiological work. Use in unsedated infants is likely to pose a whole new crop of problems which will need further study.
- Received February 28, 2000.
- Accepted April 25, 2001.
- © ERS Journal Ltd
References









