Article Text

Abstract
Aim: To evaluate if functionally relevant deficits in reading performance exist in children with essential microstrabismic amblyopia by comparing the monocular and binocular reading performance with the reading performance of normal sighted children with full visual acuity in both eyes.
Methods: The reading performance of 40 children (mean age 11.6 (SD 1.4) years) was evaluated monocularly and binocularly in randomised order, using standardised reading charts for the simultaneous determination of reading acuity and speed. 20 of the tested children were under treatment for unilateral microstrabismic amblyopia (visual acuity in the amblyopic eyes: logMAR 0.19 (0.15); fellow eyes −0.1 (0.07)); the others were normal sighted controls (visual acuity in the right eyes −0.04 (0.15); left eyes −0.08 (0.07)).
Results: In respect of the binocular maximum reading speed (MRS), significant differences were found between the children with microstrabismic amblyopia and the normal controls (p = 0.03): whereas the controls achieved a binocular MRS of 200.4 (11) wpm (words per minute), the children with unilateral amblyopia achieved only a binocular MRS of 172.9 (43.9) wpm. No significant differences between the two groups were found in respect of the binocular logMAR visual acuity and reading acuity (p>0.05). For the monocular reading performance, significant impairment was found in the amblyopic eyes, whereas no significant differences were found between the sound fellow eyes of the amblyopic children and the control group.
Conclusion: In binocular MRS, significant differences could be found between children with microstrabismic amblyopia and normal controls. This result indicates the presence of a functionally relevant reading impairment, even though the binocular visual acuity and reading acuity were both comparable with the control group.
- CPS, critical print size
- logRAD, logarithm of the reading acuity determination
- MRS, maximum reading speed
- RR charts, Radner reading charts
- wpm, words per minute
- amblyopia
- microstrabismus
- reading performance
- reading speed
- CPS, critical print size
- logRAD, logarithm of the reading acuity determination
- MRS, maximum reading speed
- RR charts, Radner reading charts
- wpm, words per minute
- amblyopia
- microstrabismus
- reading performance
- reading speed
Statistics from Altmetric.com
- CPS, critical print size
- logRAD, logarithm of the reading acuity determination
- MRS, maximum reading speed
- RR charts, Radner reading charts
- wpm, words per minute
- amblyopia
- microstrabismus
- reading performance
- reading speed
- CPS, critical print size
- logRAD, logarithm of the reading acuity determination
- MRS, maximum reading speed
- RR charts, Radner reading charts
- wpm, words per minute
- amblyopia
- microstrabismus
- reading performance
- reading speed
Reading is an important vision dependent ability in everyday private and business life. For adults and children, reading impairments may reduce the individual’s quality of life by negative effects on work and school education.1,2 With an overall prevalence of 2% to 4%, amblyopia is the most frequent cause of visual impairment in children and young adults in our population.3–5 The incidence of amblyopia is high among children with strabismus, and the child with obvious strabismus is likely to come to medical attention earlier than the child with microstrabismus or amblyopia in the absence of strabismus.6–9 This delayed beginning of amblyopia treatment may significantly influence the visual outcome.9–12 In particular, a typical monocular “reading amblyopia” was described in microstrabismus, causing functionally relevant impairments in the amblyopic eyes.13 In a previous study evaluating the reading performance of children with unilateral microstrabismic amblyopia, functional discrepancies in monocular reading performance could be reliably elucidated between the amblyopic eyes and the normal sighted fellow eyes.14 In order to avoid functional deficits, it has been recommended to continue occlusion treatment until reading performance has fully recovered.15
However, monocular reading tests do not imply that children with unilateral amblyopia are poor readers under binocular conditions. It has even been postulated that children with microstrabismus causing a monocular reading amblyopia have no difficulty in binocular reading.16,17 In contrast, others reported functionally relevant deficits.18 Therefore, the present study was designed to compare the binocular reading performance of children with unilateral microstrabismic amblyopia with the measurements of the monocular reading tests in the amblyopic and the normal fellow eye as well as with the binocular reading performance of a control group of children with full visual acuity in both eyes.
In order to obtain comparable and reliable measurements, a standardised reading chart system with three equivalent reading charts for the simultaneous determination of reading acuity and speed was used in the present study.19 The highly comparable sentence optotypes of the Radner reading charts (RR charts) have been designed, considering the international standards for vision tests,20–25 as well as the characteristics of amblyopic vision.19,26 The print sizes of the optotypes were logarithmically scaled to provide constant geometric proportions controlling contour interaction. For adults, the RR charts represent a valuable clinical test for evaluating functional differences in reading performance.27 All children performed the reading test without any difficulties. The reading tests were quick to administer and well accepted by the children. Considering the syntactic complexity of the test sentences, the RR charts are a suitable and reliable reading test for children starting from the third school grade19 and were used in the present study to investigate the binocular reading performance of children with unilateral microstrabismic amblyopia.
MATERIALS AND METHODS
This prospective clinical study evaluated the reading performance of 40 children (21 males and 19 females). The mean age was 11.6 (SD 1.4) years, ranging from 10 years to 12 years. In 20 of the tested children a unilateral amblyopia caused by primary microstrabismus had been diagnosed; the other 20 children were normal controls without any ocular disease. The two study groups were comparable in age, sex distribution, educational level, and the mean school marks (p>0.05). The study was performed in accordance with the Declaration of Helsinki. Before all examinations, the parents’ oral informed consent was obtained. The demographic characteristics of the study population are given in table 1.
Demographic characteristics of the study population
In the first group, 20 children with monocular amblyopia caused by microstrabismus were included. Microstrabismus is defined by a small angle of squint (either convergent or divergent) with less than 5 degrees.13,16 Children with a large angle strabismus or a secondary microstrabismus (microstrabismus that remains after operation for a large angle of strabismus) were not included in the study population. Also, patients with other ocular diseases or dyslexia were excluded from the study population.
Cover-uncover tests and alternate cover tests were performed for the clinical diagnosis of microstrabismus. The squint angle was evaluated with simultaneous prism alternate cover test (<5 prism dioptres). Accommodation was tested by dynamic retinoscopy. Convergence and motility were tested and monocular fixation was evaluated by direct ophthalmoscopy. As a sensory test, the Worth four dot test was performed. Near stereoacuity was tested with the Titmus stereo test.
All children included in the amblyopic group were under continuing amblyopia treatment. Treatment was started before the age of 4–5 years when microstrabismic amblyopia has been first diagnosed. Treatment included correction of any refractive error and occlusion therapy, resulting at least in the expected age dependent physiological improvement of visual acuity.18 In all children, the improvement in visual acuity ranged from two to five acuity lines in the past 2 years.
For the control group, children with no ocular disease and full visual acuity (<logMAR 0.1) in both eyes under monocular and binocular conditions were included after complete eye examination. Any interocular difference in visual acuity or reading acuity of more than one line led to exclusion from the study population.
All tests were performed with the patient’s optimal correction. In the amblyopic group, refractive errors were evaluated objectively by retinoscopy (cyclopentolate 1%) 1 week before the reading tests and subjectively adjusted at the beginning of the testing session. All tests were performed with the child’s optimal correction for far and near vision. Accommodative deficits were compensated by an adequate near addition to guarantee best corrected near performance.10
In all tested children, best corrected reading ability was tested using the RR charts19 at a reading distance of 25 cm. All tests were performed at a constant luminance of 80–90 cd/m2. The sentences were covered with a piece of paper, and the children were asked to uncover sentence after sentence, reading each one aloud as quickly and accurately as possible. The children were instructed to read each sentence to the end without correcting any reading errors. Reading time was measured with a stopwatch. Reading speed in words per minute (wpm) was calculated based on the number of words in a sentence and the time needed to read the sentence. The maximum reading speed (MRS) was the best reading speed achieved in the test. Reading acuity was set at the smallest print size the patient was able to read completely and expressed in terms of logRAD ( = logarithm of the reading acuity determination/reading equivalent of logMAR). LogRAD print size is defined by the height of a lower case “x” and is calculated as follows: log10 [(angle subtended by x height)/(5 arc min)]. Based on the psychophysical function of reading speed, defining that reading speed increases with print size up to the critical print size (CPS; the smallest print size the patients read with optimal reading speed), and then plateau at the MRS,29 larger print sizes were tested until this asymptotic level was reached. Visual acuity was tested at a testing distance of 4 metres, using ETDRS logMAR charts.22 Both eyes were tested monocularly and binocularly in randomised order according to the orthogonal Latin square design, using equivalent RR charts.27,28
Statistical methods
All calculations were performed with SAS Release 8.2. Differences between the two groups in respect of the binocular reading performance were analysed by two sample t tests. Differences between the normal eyes and the amblyopic eyes with respect to visual acuity, reading acuity, maximum reading speed (MRS), and CPS were analysed for significance by paired t test. For non-parametric data, the Mann-Whitney U test was used. For all analyses, a two sided p value <0.05 was considered to indicate statistical significance.
RESULTS
Comparing the monocular and binocular reading performance of children with unilateral microstrabismic amblyopia
In the microstrabismic group, the reading performance of the sound fellow eyes was comparable to the binocular reading performance. No significant differences were found for any of the tested reading parameters (p>0.05).
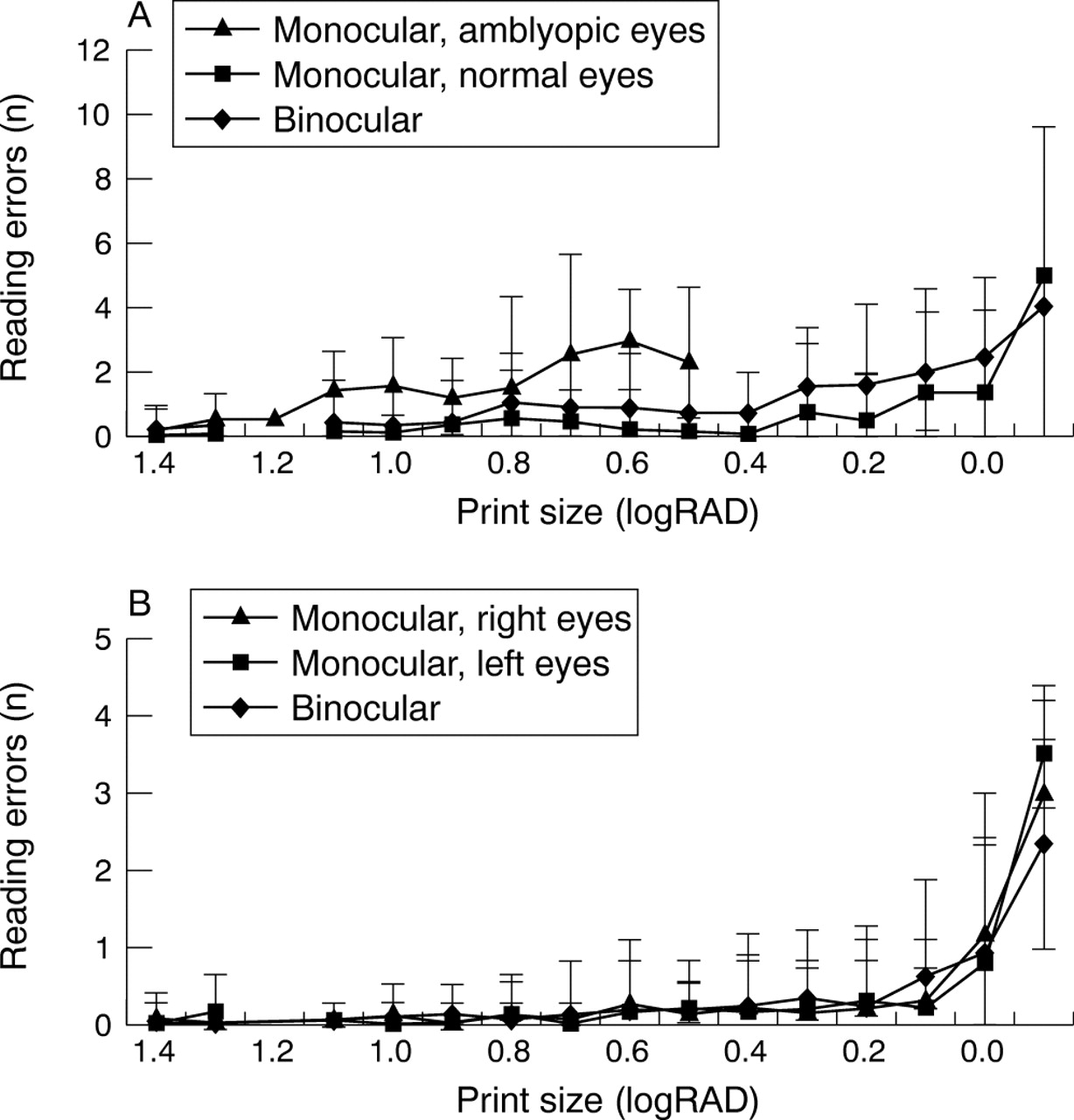
Reading performance was significantly impaired in the amblyopic eyes. In comparison with the sound fellow eyes and the binocular reading tests, significant differences were found for the monocular reading acuity and the MRS (p<0.05; table 2). In the amblyopic eyes, the functionally relevant impairment was also found in respect of the reading speed based on print size (fig 1) and the reading errors based on print size (fig 2). Also for the visual acuity, a small, but significant residual deficit was found between the amblyopic eyes (logMAR 0.19 (0.15)) and the sound fellow eyes (logMAR −0.1 (0.07)).
Monocular visual acuity and reading parameters in children with unilateral microstrabismic amblyopia (n = 20)

Reading speed (words per minute = wpm) based on print size (logRAD) (A) in children with unilateral microstrabismic amblyopia; (B) in normal sighted controls (n = 40).
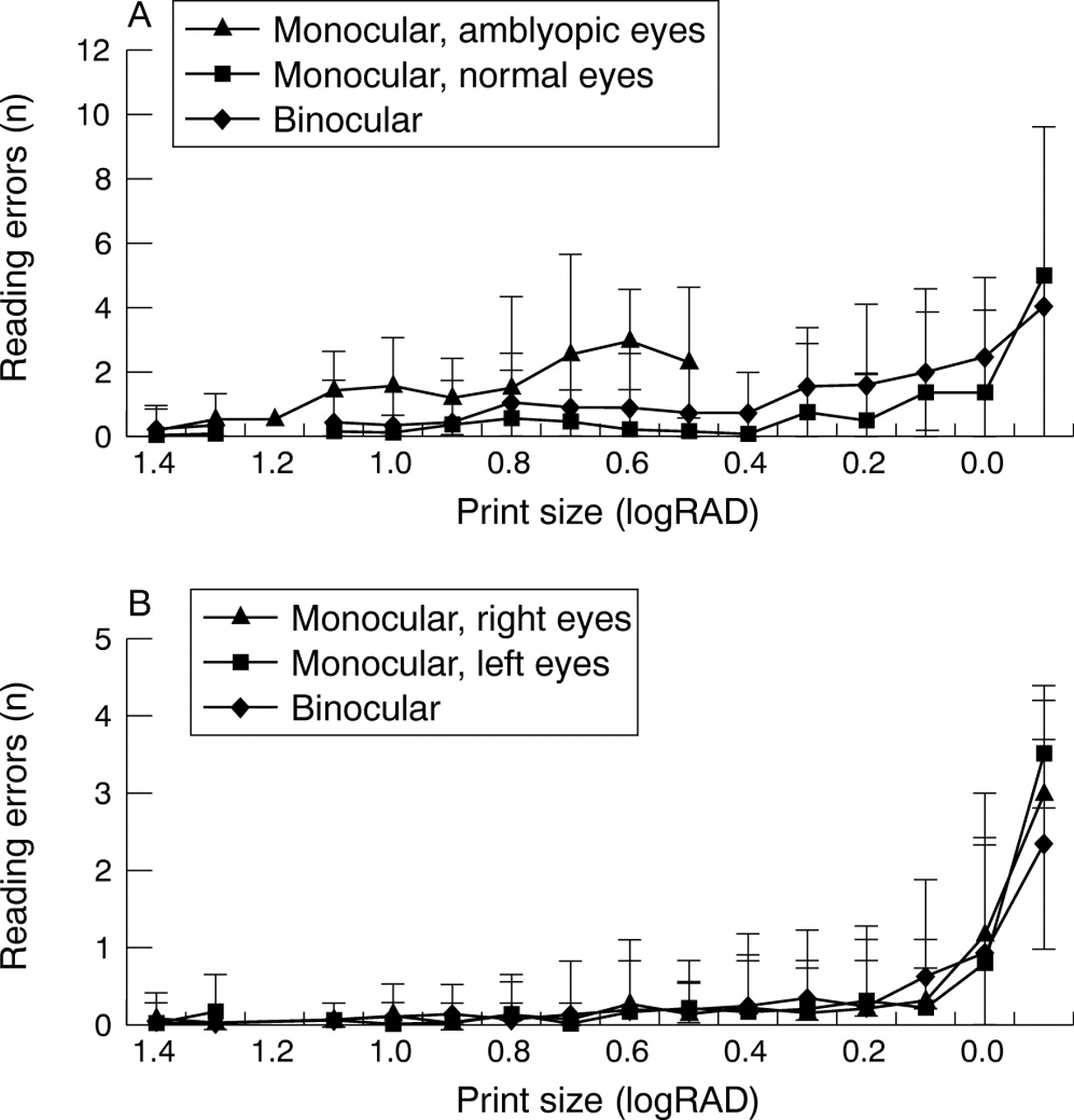
Reading errors based on print size: (A) in children with unilateral microstrabismic amblyopia; (B) in normal sighted controls (n = 40).
Comparing the reading performance of the amblyopic group and the normal sighted control group
No significant differences between the two groups were found in respect of the binocular logMAR visual acuity and reading acuity (p>0.05; table 4).
Monocular visual acuity and reading parameters of the control group (n = 20)
Comparing monocular visual performance of the sound fellow eyes of the amblyopic group (n = 20) and the right eyes of the control group (n = 20)
In respect of the binocular MRS, significant differences were found between the children with unilateral microstrabismic amblyopia and the normal sighted controls (p = 0.03; fig 3): whereas the controls achieved a binocular MRS of 200.4 (11) wpm, the children with unilateral amblyopia achieved only a binocular MRS of 172.9 (43.9) wpm.

{kind=link}
{kind=link}
{kind=link}
A statistically significant difference in binocular maximum reading speed (words per minute) was found between the children with unilateral microstrabismic amblyopia and the normal sighted control group (p = 0.03).
There was also a small, but statistically significant difference in the number of reading errors between the two groups for the binocular tests (p<0.05; fig 2).
Comparing the sound eyes of the amblyopic group with the normal sighted controls in respect of the monocular visual acuity and reading parameters, no significant differences were found (visual acuity: p = 0.4; reading acuity: p = 0.2; MRS: p = 0.11; CPS: p = 0.77; logRAD/logMAR ratio: p = 0.07).
In the amblyopic group, nine of the tested children achieved a relatively high MRS of more than 180 wpm. Additional analyses were performed, searching for significant differences in the main visual and demographic characteristics between the microstrabismic children with higher and lower MRS: No significant differences were found for the children’s age, visual acuity, accommodative impairment, strabismic angle, and refractive error (p>0.05). In contrast, significant differences were found for fixation: for the children with high MRS, fixation was central or unstable central in all patients, none had an eccentric fixation in the deviating eye. Analysing the mean duration of amblyopia treatment, the children with high MRS were significantly longer under treatment (mean duration 7.2 (0.7) years v 6.3 (1) years; p = 0.03). Also for the sensory Worth four dot test and the Titmus stereo test, the children with the high MRS showed a significantly better performance.
DISCUSSION
In this study, the average binocular maximum reading speed of children with microstrabismic amblyopia was significantly reduced when compared to normal sighted, age matched controls (p = 0.03; table 5), indicating a functionally relevant reading impairment. Whereas the controls achieved a binocular MRS of 200.4 (11) wpm, the children with unilateral amblyopia achieved only a binocular MRS of 172.9 (43.9) wpm. These differences in reading speed were found to be above the level for a “real change” in vision evaluated for the RR charts.27 In contrast, no significant differences between the two groups were found in respect of the binocular logMAR visual acuity and reading acuity (p>0.05, table 5). Since reading speed is known to be closely related to visual function,29–32 these findings indicate the presence of a functionally relevant deficit that would be underestimated by acuity measurements. Differences in reading practice between the groups cannot be considered to significantly bias the above mentioned results, since no significant differences were found for the monocular visual acuity and reading parameters in the sound eyes of the amblyopic group when compared to the normal sighted controls (p>0.05; table 4).
Binocular visual acuity and reading parameters of the amblyopic and the control group (n = 40)
Reading speed measurements provide more information about functional impairment than the visual acuity.33–36 Also for amblyopic children, it has been shown that high contrast visual acuity is not always representing the full visual deficit.37 Testing adults with unilateral anisometropic amblyopia, reading speed measurements evaluated relevant functional differences in monocular reading speed, when compared with the normal fellow eyes.38 Also in children with unilateral microstrabismic amblyopia, functional discrepancies in reading performance could be reliably elucidated between the amblyopic eyes and the normal sighted fellow eyes.14 Even relatively mild forms of microstrabismic amblyopia with no persistent acuity deficit lead to an impairment of monocular reading ability.16 On the other hand, it has been reported that these children had no difficulty in binocular reading, explained by the fact that patients with primary microstrabismus rarely alternate.16 The present study, however, evaluated a significantly lower binocular MRS in children with monocular microstrabismic amblyopia when compared with normal sighted controls, indicating the presence of a functional reading impairment.
The significance of particular changes in reading speed has been evaluated recently for various eye diseases— age related macular degeneration, cataract, and anisometropic amblyopia.27,29,30,33,38 As in the present study, statistically significant differences in reading speed were found, which have been used for discriminating affected and sound eyes or different eye diseases by reading tests.29,33
Patients with primary microstrabismus have a high degree of binocularity, which may suggest that the ocular misalignment may have a sensory rather than an oculomotor origin, as in large angle strabismus.39 However, as in large angle strabismus, the anomalous retinal correspondence and defective stereopsis of microstrabismus appear to be consequences of abnormal visual experience caused by an interocular deviation or by anisometropia.39 In addition, reading impairment may be significantly influenced by one of the following deficits: abnormal contour interaction,40 which can be assessed using the difference between linear and single optotypes acuity; abnormal eye movements,41 which can be assessed using the difference between a high contrast and repeat letter format acuity measure; and positional uncertainty.42 Consequently, fixation is only one of many aspects influencing the visual performance in amblyopic patients and may not be considered to sufficiently explain visual function in amblyopic vision. Nevertheless, binocular confusion, deficits in quality of binocular coordination of saccades, or the presence of suppression scotomata centred around the fixation point of the squinting eye may explain the significantly impaired binocular MRS of the amblyopic group.39,43 However, in the present study, the reading performance of children with microstrabismic amblyopia was compared with the reading performance of normal sighted controls, not with monofixators without amblyopia. In future research, it will be interesting to investigate if monofixators without amblyopia show similar reading impairment, in order to discriminate between reading impairment caused by amblyopia or fixation disparity.
In the amblyopic group, nine of the tested children achieved relatively high MRS measurements of more than 180 wpm. In comparison with the other children of the amblyopic group with a significantly lower MRS, significant differences were found in respect of fixation, sensory tests, and the duration of treatment, which was significantly longer in the better reading group.
Besides the above mentioned visual factors influencing reading performance, it is important to also consider the fundamental influence of comprehension. Reading and understanding a sentence is a complex process that requires comprehension of the meaning of the individual words and also the assignment of the structural relations between these words.44
In case of dyslexia, a type of learning disability that affects reading ability, the child may have problems remembering, recognising, and or reversing written letters, numbers, and words, might read backwards, and may have poor handwriting. Neurological dysfunction is suspected as the cause of the reading disability in dyslexia, since the development of intelligence, learning ability, and visual function may be normal. Consequently, dyslexic children might have an impaired reading acuity and speed in reading tests using short test sentences and were excluded from the present study.
In summary, this study determined that monocular reading tests do not imply that children with unilateral amblyopia are poor readers under binocular conditions. The binocular visual acuity and reading acuity of the amblyopic group were both comparable with the control group. However, the binocular MRS was significantly reduced in the amblyopic group, indicating functional reading impairment in comparison with normal sighted controls.
REFERENCES
Footnotes
-
Supported by the “Jubiläumsfonds der österreichischen Nationalbank.”
-
Competing interests: none declared