Article Text

Abstract
AIM To compare three different strategies for determining admission dates for patients awaiting cataract extraction after scoring for visual impairment.
METHODS 357 patients attending for assessment for cataract surgery were scored for visual impairment. These scores were used as a basis for ranking patients into three impairment strata. A computer simulation was used to compare 3 years' operation of different admission strategies—a first come first served booking system, a triage booking system, and a waiting list system in which admissions were strictly ordered according to priority stratum. Differences in priority weighted delays before treatment were analysed.
RESULTS Both the triage system and the priority based waiting list system gave considerable reduction in priority weighted delay compared with a first come first served admission policy. The percentage reduction achieved (30%–60%) is strongly influenced by the number of weeks fully booked when the booking systems are introduced. The priority weighted delay of the triage system, where booking decisions were made at the time of the outpatient assessment, was consistently and substantially outperformed by the priority based waiting list system where the decision to allocate an admission date was delayed as long as possible.
CONCLUSIONS There is considerable scope for reducing delays to high priority patients if simple rules are used to determine admission dates. Using these rules, booking patients at the time of the outpatient assessment gives substantially less benefit in terms of reducing delays to high priority patients than if the decision about the admission date is deferred.
- cataract
- waiting list
- priority scoring
- computer simulation
Statistics from Altmetric.com
Cataract extraction is one of the most common and cost effective surgical procedures performed within the National Health Service.1-3 There is mounting pressure on resources as the threshold for cataract surgery has reduced and the number of elderly patients who could benefit from surgery has increased.45 Therefore, unless productivity improves or more operating sessions become available it is probable that waiting lists for cataract surgery will lengthen. An alternative strategy for dealing with the cataract load is to ration surgery by limiting access to waiting lists.6 Given that the average waiting time for cataract surgery in the UK exceeds 6 months,7 it is useful to consider how waiting lists can be managed so that patients with severe visual impairment are treated as soon as possible. There are two key elements to this problem. Firstly, there must be a valid method for ranking patients in terms of their impairment and need. Secondly, effective use must be made of this information by managing the waiting list efficiently.
In practice, a waiting list is easiest to manage if patients are not scored and they are admitted in the order in which they are seen in clinic, irrespective of their visual impairment. In principle, it is desirable to manage a waiting list by first assessing visual impairment and then admitting the worst off patients first. However, with such a system, patients with low scores suffer lengthy waits or there is the option of referring them back to their community physician until their vision deteriorates. Uncertainties regarding the date of admission has led to moves towards booking systems in which patients are given a firm date for admission at the time of their initial assessment. Although this may be preferable for the patient in terms of peace of mind, it is by no means certain that this is compatible with efficient waiting list management. Indeed, the possibility exists that for a busy surgical unit operating close to capacity a well intentioned booking system might conflict with other factors related to load management.
There has been little work on the quantitative evaluation of booking systems in relation to their effects on the structure of the waiting list and waiting times.8 Although the reliability of priority assessment for cataract surgery is still debated, we have compared three different strategies for waiting list management. We have investigated this in the context of a cataract clinic and describe a pretrial evaluation and comparison of the different admission policies. Computer modelling has been used to compare the effects of different waiting list management options in terms of a number of performance measures related to the overall operation of the service.
Materials and methods
THE COMPUTER MODEL
A computer simulation method known as PASTA (Priority Admission STrategy Analysis) has been developed by the second author as a research tool for investigating operational consequences of different booking or admissions systems.9 The basis of the simulation method is a notional set of referrals to a single clinic. For each patient, the records contain information about the date of referral, date of outpatient assessment, and priority weighting. Randomisation is used to generate fictitious referral data. In doing this, the overall number of referrals per week is taken as fixed. Each week's referrals are randomly apportioned among the different impairment categories in such a way that the long term proportions in each category accord with prespecified values. The dates of outpatient assessment and treatment are then determined by the simulation using an algorithm to replicate the waiting list management rules being investigated.
Within the simulation, after patients receive an outpatient assessment, they are booked for surgery as a day case admission. The booking date depends on the particular admission policy being tested. A “priority weighting factor” is central to this simulation. This is a number between 0 and 100, associated with each case, which expresses the percentage importance attached to each day a patient waits before being treated.6
BOOKING SYSTEMS
The PASTA simulation allows comparison between different potential booking systems. The only requirement is that a booking system can be expressed in terms of a set of rules that allow it to be expressed as an algorithm. The present study concerns three systems for determining treatment dates. The baseline system is a “first come first served” system whereby patients are booked in the order that they are seen in clinic, irrespective of visual impairment.
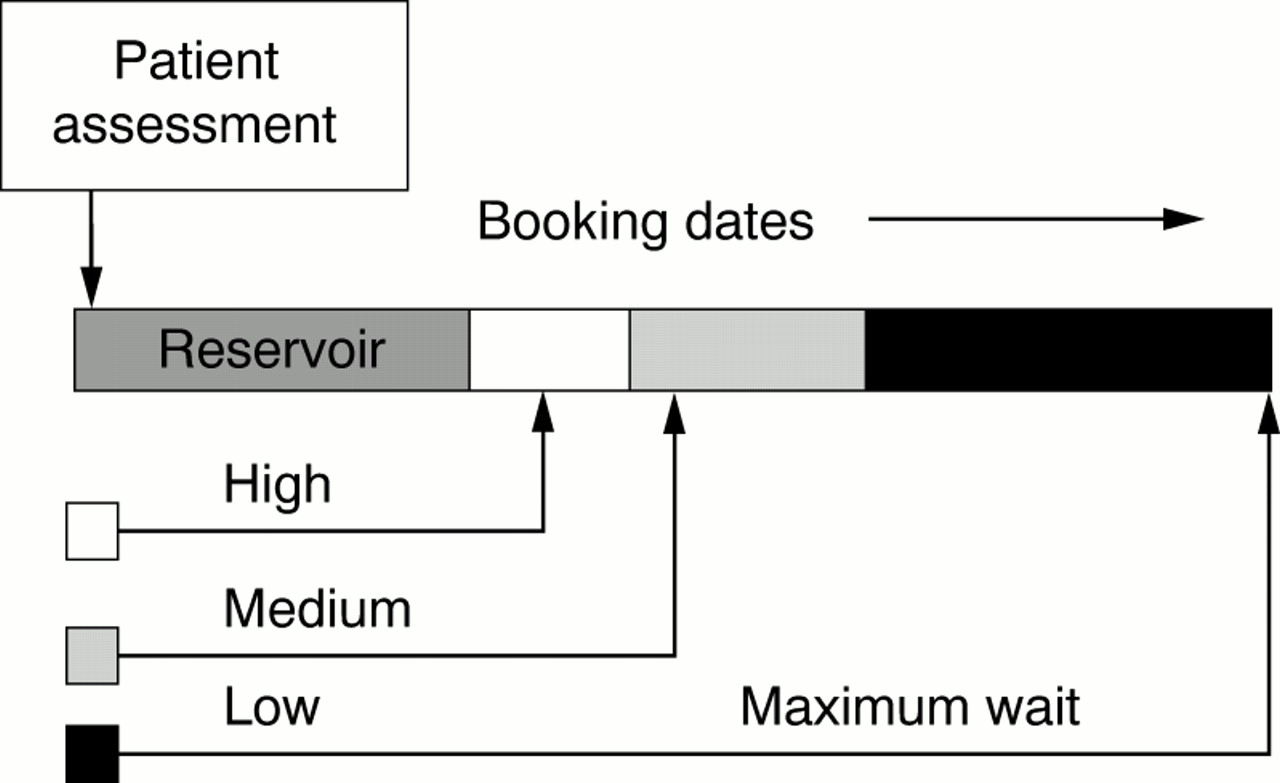
The second system reflects the common clinical practice of “triage” where patients are categorised into a small number of priority strata. In principle, many such strata could be specified, but in the current study only three are used: high, medium, and low priority. The principle of the system's operation is illustrated in Figure 1. The figure illustrates the possible decisions that can be made at the time of an outpatient assessment. The horizontal bands represent future potential theatre bookings, and can be thought of as consecutive pages in a diary, one week to a page. Different bands are shown with different shading. Although each band will usually represent a different number of weeks, the total time span of each band remains constant from one week of operation of the system to the next. A practical implementation of the system could be achieved by marking the future bands in a week to a page diary with colour coded paper clips.

The operation of the triage priority booking system, allocating patients to different booking zones according to their priority score.
Booking decisions for the triage system are made for each patient seen in turn at the time of the outpatient assessment. The system operates according to the following hierarchy of rules, with rule A taking precedence over B and C.
- (A)
A “reservoir” of operating slots in the near future is kept fully booked. If a spare slot appears in this reservoir it is filled with a patient from the next outpatient clinic irrespective of their priority. The duration of this reservoir period would normally be a few weeks.
- (B)
Patients assessed as being in the lowest priority stratum are booked into an operating slot as far into the future as acceptable.
- (C)
Patients assessed as being in priority strata other than the lowest are booked for the first available free slot in the theatre diary band designated for their priority strata. If there are no free slots available within the appropriate band, then a booking is made for the first available theatre slot thereafter.
The third treatment management system, a priority based waiting list, reflects the clinical practice of using a waiting list as opposed to a booking system. Patients are placed on a waiting list and not given an admission date at the time of their outpatient assessment. Booking decisions are made as late as possible, assigning available theatre slots to the highest priority patients currently on the waiting list. An exception to this is that no patient can wait longer that the maximum time deemed acceptable, and if this becomes a possibility, the patient concerned is assigned an artificially high priority score.
PERFORMANCE INDICATORS
The PASTA methods allows the following outcome measures to be considered, some of which make use of the priority weighting factor assigned to patients: cumulative waiting time (patient days), cumulative priority weighted waiting time (priority adjusted patient days), cumulative admissions (number of operations), maximum waiting time (days), number on waiting list (patients)
SETTING THE SYSTEM PARAMETERS
A total of 357 consecutive patients presenting to a cataract assessment clinic between February 1998 and August 1999 were scored as part of their clinical assessment using a template adapted from Hadornet al.6 In this system only those factors that have been shown to benefit from cataract surgery are assessed, and these are based on the VF14, which is a validated instrument for measuring loss of visual function.10 In practice, the visual acuity was measured (contributing 0–40 points) and ocular co-morbidity and health related quality of life (ability to live independently, mobility, restricted activity, etc) was assessed (contributing 0–60 points); these two scores were then combined to give a total priority score (0–100 points) which gave a ranking for admission. The option of discharge of low priority patients was not included in our analysis. These data were used to provide information about the variability of visual impairment among patients referred for surgery. For the purposes of this study, three priority strata were used. The highest and lowest strata were determined by the upper and lower quartiles from the distribution of visual impairment. The priority weighting factor used for each stratum was the mean priority score for patients from the stratum concerned. The maximum wait after assessment was chosen as 14 months as this was policy within the Moorfields Eye Hospital NHS Trust in April 2000.
Within the triage system, it was assumed that high priority patients would be booked as soon as possible. This was subject to the proviso that theatre lists should be kept fully booked for at least 4 weeks ahead. The target wait for patients from the middle stratum was 16 weeks, although other values were also investigated. To initialise the computer model it is assumed that at the start of the simulations theatre sessions are fully booked for a number of weeks into the future. A range of different values was considered for this initial booking load ranging from 10 to 50 weeks. For each initial booking load, 10 separate simulations were carried out comparing outcomes for the three admission policies operating over a period of 300 weeks. The decision to use 10 separate simulations was the result of initial experimentation with the simulation, which revealed relatively small variance in the system's output. Using 10 rather than a smaller number of simulations errs very much on the side of caution; however, computer running time constraints were not an issue.
Results
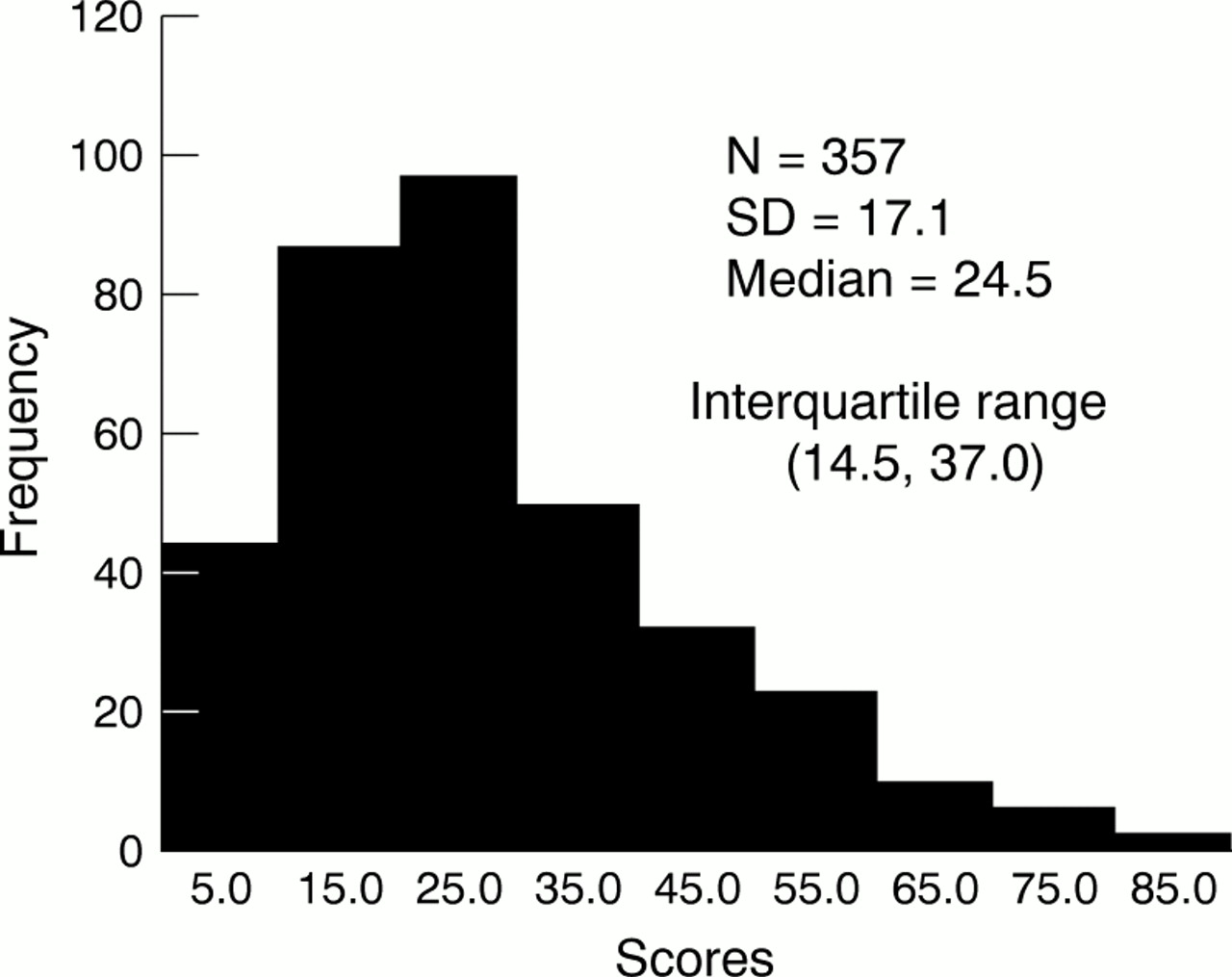
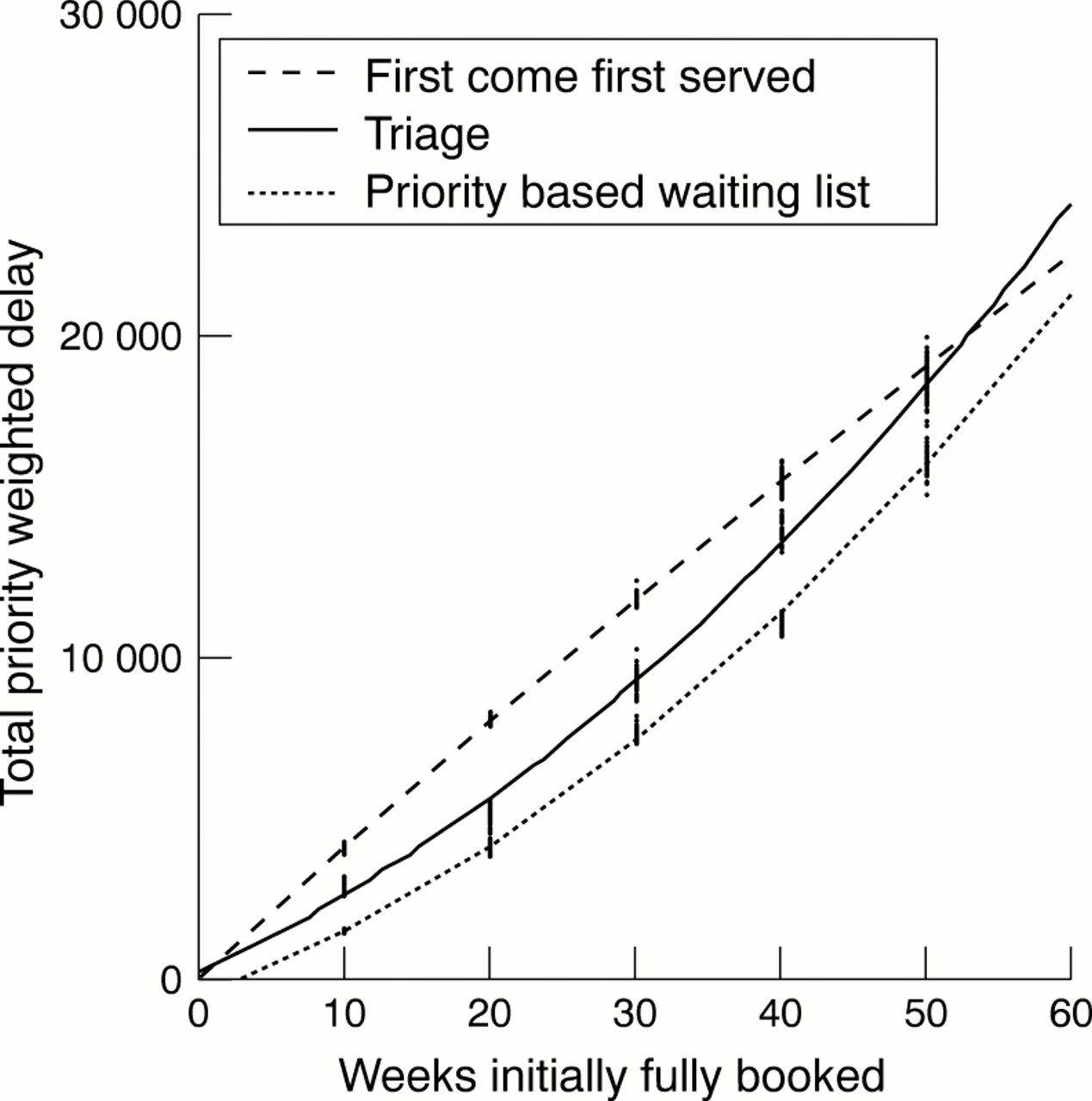
The distribution of the visual impairment scores is shown as a histogram in Figure 2. Based on this distribution the priority classes and other data used by the model are shown in Table 1. Since all admissions within the simulation were for day case surgery, the only effect of different admission systems is to alter the order in which patients are treated; there were no differences in outcome in terms of overall waiting list size, throughput, or mean waiting time. Both the triage and the waiting list systems gave rise to increased delays for low priority cases that are assigned the maximum acceptable wait; however, there were substantial and consistent reductions in total priority weighted delay. The scale of such changes varied considerably depending upon the number of weeks of surgery fully booked at the start of the simulations. Figure 3 shows an overall comparison of the performance of the three systems depending on the number of weeks initially fully booked. For each treatment allocation system, the 10 independent simulations produced clusters of points with considerable overlap. Interpolation curves are displayed derived from best fit quadratic regression, which gave a good fit in each case.

Distribution of the visual impairment scores.
Parameter values used during computer modelling

Comparison of total priority weighted delay incurred over 3 years of operation of the treatment scheduling systems. Curves represent best fit quadratics through clusters of 10 points each representing an independent simulation.
For the first come first served booking system, in which no account is taken of priority scores, the overall priority weighted delay increases in direct proportion to the number of weeks initially fully booked. This provides a benchmark against which to compare the other systems, and the degree of efficiency achieved is the percentage reduction in priority weighted delay compared to the first come first served system. Figure 4 shows the variation in such percentage reductions depending on the number of weeks initially fully booked. It is useful to display the clusters of data, both to demonstrate the fact that clusters from different systems are disjoint, but also because quadratic regression interpolation was less satisfactory.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage reduction in priority weighted delay in comparison with first come first served booking system. Each point represents 3 years' operation of the system for different periods fully booked at the initiation of the simulation.
Discussion
There is concern in the United Kingdom about the size of waiting lists and the length of time patients have to wait for cataract surgery. In addition, it is recognised that there are still many individuals in the community with cataract who could benefit from surgery who have not been identified by medical services.1112 The pressure on resources is therefore likely to increase. There have been efforts to contain costs and increase efficiency as, even in the absence of restricted resources, there is a natural desire to maximise the effectiveness of health care.1314 Although considerable attention has been directed towards increasing the throughput of cataract operating lists, little has been published on the effects of different strategies of waiting list management.
Inherent in our analysis of waiting list management is the assumption that patients with cataract can be ranked according to their visual impairment. We used the New Zealand prioritisation system to determine the weighting of patients' impairment and thus their priority for treatment.6 Mathematical modelling was used as this allows the effects of different strategies for patient admission to be investigated for identical patterns of patient referrals. It also provides results rapidly as opposed to clinical studies that can take years to complete and indeed may not be feasible to conduct. For example, this study is based on 300 simulations of cataract admissions over 3 years. Cataract surgery is a good template for this type of study as the majority of operations are day case procedures, the outcome of the procedure is rarely affected by the time spent on the waiting list, and validated instruments exist to assess visual impairment due to cataract.
Our results show that the most effective admission system for minimising priority weighted delay is to admit high priority patients from a waiting list, rather than booking them at the time of the outpatient assessment. This highlights a potential conflict when determining admission policy. The advantage of a waiting list for the clinician, and some patients, is the ease with which the most needy patients are selected from the pool awaiting surgery. The disadvantages for the majority of patients is that they are not given a fixed date for admission and they are called for their surgery at relatively short notice. Achieving a balance between these competing demands may be impossible. Interestingly, booking at the time of outpatient assessment following priority scoring (triage) also achieves useful benefits in terms of reducing delays for high priority patients when compared with a first come first served system, although this benefit was not quite as dramatic as for the waiting list system. Both of the priority admission systems that we evaluated have the disadvantage that patients with low scores have a longer wait for admission than with a first come first served system, typically the longest wait that is politically acceptable. This is an inevitable consequence of a priority system. Indeed, the very act of ensuring that low priority patients have a long wait reduces delays for the higher priority patients if throughput is maintained.
Our simulation is based on a mechanistic and simplistic view of a waiting list. Many variables that could influence the implementation of a waiting list, such as availability of staff, fluctuations in referral rates, and failure to attend for surgery were ignored. The model was framed in simple terms for the pragmatic reason that a system which does not operate effectively within a simple simulation framework will almost certainly have a worse performance if implemented clinically. The model was also based on priority scoring, which is an attractively simple concept to rank patients for treatment, but which has yet to be subject to validation. Nevertheless, when we have evaluated different operating systems to determine which is the optimal way to transfer priority scores to waiting lists or booking systems, we have highlighted the potential advantage of a waiting list. This raises the possibility that what may be politically desirable may be inefficient in terms of service delivery.