Article Text

Abstract
BACKGROUND Procalcitonin has been advocated as a marker of bacterial infection.
OBJECTIVE To evaluate diagnostic markers of infection in critically ill children, comparing procalcitonin with C reactive protein and leucocyte count in a paediatric intensive care unit (PICU).
METHODS Procalcitonin, C reactive protein, and leucocyte count were measured in 175 children, median age 16 months, on admission to the PICU. Patients were classified as: non-infected controls (43); viral infection (14); localised bacterial infection without shock (25); bacterial meningitis/encephalitis (10); or septic shock (77). Six children with “presumed septic shock” (without sufficient evidence of infection) were analysed separately. Optimum sensitivity, specificity, predictive values, and area under the receiver operating characteristic (ROC) curve were evaluated.
RESULTS Admission procalcitonin was significantly higher in children with septic shock (median 94.6; range 3.3–759.8 ng/ml), compared with localised bacterial infection (2.9; 0–24.3 ng/ml), viral infection (0.8; 0–4.4 ng/ml), and non-infected controls (0; 0–4.9 ng/ml). Children with bacterial meningitis had a median procalcitonin of 25.5 (7.2–118.4 ng/ml). Area under the ROC curve was 0.96 for procalcitonin, 0.83 for C reactive protein, and 0.51 for leucocyte count. Cut off concentrations for optimum prediction of septic shock were: procalcitonin > 20 ng/ml and C reactive protein > 50 mg/litre. A procalcitonin concentration > 2 ng/ml identified all patients with bacterial meningitis or septic shock.
CONCLUSION In critically ill children the admission procalcitonin concentration is a better diagnostic marker of infection than C reactive protein or leucocyte count. A procalcitonin concentration of 2 ng/ml might be useful in differentiating severe bacterial disease in infants and children.
- sepsis
- infection
- procalcitonin
- C reactive protein
- leucocyte count
Statistics from Altmetric.com
The non-specific nature of signs and symptoms in febrile infants and children makes the clinical differentiation of bacterial and viral infection difficult even for the experienced clinician. It may be even more problematic to identify children with severe bacterial disease, such as septicaemia or meningitis, especially if no localising signs are present.1
Because the diagnosis of “possible sepsis” has implications for antibiotic usage and hospital stay, management strategies have evolved based on a combination of clinical and laboratory information.2-6 Although laboratory markers of infection might aid in differentiating the type of infection in infants and children, opinions vary on the interpretation of tests such as the leucocyte count, neutrophil count, band cell count, and C reactive protein concentration.2 5 7-15
A polypeptide identical to a prohormone of calcitonin, procalcitonin, was initially described as a potential marker of bacterial disease by Assicot et al.16 Procalcitonin is almost undetectable under physiological conditions (pg/ml range), but rises to very high values in response to bacteraemia or fungaemia, and appears to be related to the severity of infection.16This response can be duplicated by in vivo endotoxin administration, which results in a rapid rise in procalcitonin, paralleling that of tumour necrosis factor and interleukin 6.17 Sequential measurements in patients with bacteraemia have shown a rapid fall within 48 hours of antibiotic administration.16 An immunoluminometric procalcitonin assay is now commercially available (BRAHMS Diagnostika, Berlin, Germany) and values can be obtained on a routine basis within two hours of blood sampling.
Several authors have postulated that procalcitonin measurement might be superior to commonly used tests, such as C reactive protein measurement, as an aid to the early diagnosis of childhood bacterial sepsis.18-21 Others have cautioned that procalcitonin values should be interpreted with caution in the early neonatal period, because of the transient physiological rise in procalcitonin in apparently well newborns.18 22 23 We present a prospective observational study of markers of infection in children admitted to a paediatric intensive care unit. The diagnostic value of admission procalcitonin measurement is compared with that of C reactive protein and the leucocyte count.
Methods
Over an 18 month period, 175 children, median age 16 months (range, 0.03–193), were enrolled in the study on admission to the paediatric intensive care unit (PICU). Forty six patients (26%) were aged less than 3 months, and 64 (37%) between 3 and 36 months. Most children (n = 156; 89%) were admitted by a PICU retrieval team, within 24 hours of hospital presentation. Patients were excluded if they had received parenteral antibiotics in the past seven days (except within the preceding 24 hours) or if they had undergone surgery.
Children were classified according to their clinical and laboratory data into one of five categories: non-infected controls—for example, toxin ingestion, trauma, or seizures (n = 43; 25%); viral infection (n = 14; 8%); localised bacterial infection without shock—for example, pneumonia, tracheitis, or urinary tract infection (n = 25; 14%); bacterial meningitis/encephalitis (two patients with mycoplasma encephalitis were included in this group) (n = 10; 6%); and septic shock (n = 77; 44%). Table 1 shows the underlying aetiology in patients with septic shock.
The aetiology in 77 patients with septic shock
Septic shock was defined as hypotension or poor capillary refill responding to fluid or pharmacological intervention, in the presence of hyperthermia or hypothermia, tachycardia, and tachypnoea, in addition to at least one of the following: acute mental changes, hypoxaemia, hyperlactataemia, or oliguria.24 In addition to these features, evidence of infection was required for final inclusion in the category of septic shock—for example, bacteriological isolate (not necessarily positive blood culture); characteristic meningococcal or staphylococcal rash; or cerebrospinal, bronchoalveolar, or peritoneal fluid profile consistent with bacterial infection. Six children (3%) who were enrolled with diagnoses of presumed septic shock, but who subsequently had no documented focus of infection, were excluded from the group analysis and evaluated separately.
On admission to the PICU, blood was sampled for routine laboratory investigations including blood culture, C reactive protein, and leucocyte count, in addition to 2 ml clotted blood for procalcitonin measurement. The procalcitonin sample was centrifuged, the serum separated, frozen at −70°C, and measured in batches by immunoluminometric assay (BRAHMS Diagnostika). Samples with procalcitonin concentrations at or above the 500 ng/ml upper limit of the assay were diluted 1/4 and repeated. Laboratory results were not available to investigators until after patient classification had taken place, although investigators were not blinded for patient outcome. Leucocyte counts were measured by the hospital haematology laboratory, and C reactive protein was measured by enzymatic heterogeneous sandwich immunoassay (Vitros 950 analyser; Johnson and Johnson, Rochester, New York, USA) by the hospital biochemistry laboratory.
Data were analysed by sensitivity and specificity derived from the receiver operating characteristic (ROC) curve, and area under the ROC curve. Comparison between groups was made by the Mann-Whitney test, Kruskal-Wallis non-parametric analysis of variance (ANOVA), and Dunn’s test for multiple comparisons. Statistical analysis was performed using GraphPad Instat (GraphPad Software, San Diego, California, USA) and Analyse-It (Analyse-It Software, Leeds, UK). The study was approved by the hospital ethics committee and verbal consent was obtained from parents for the additional blood sampling.
Results
Table 2 shows admission procalcitonin, C reactive protein, and leucocyte count values. Procalcitonin differed significantly across the five categories of infection (p < 0.0001; Kruskal-Wallis). Procalcitonin was higher in children with septic shock compared with all other groups (p < 0.001; Dunn’s) except bacterial meningitis. Procalcitonin was significantly higher in bacterial meningitis compared with viral infection and controls (p < 0.05 and 0.001, respectively). In the subgroup of children with meningococcal disease (n = 37; 21%) admission procalcitonin was no higher (median, 104 ng/ml; range, 7.7–760) than in non-meningococcal septic shock (median, 92 ng/ml; range, 3.3–736; p = 0.32). Separate post hoc analysis of the six patients with presumed septic shock excluded from further comparison showed a median procalcitonin of 182.5 ng/ml (range, 5.1–500), comparable to that of the septic shock group.
Admission procalcitonin (PCT), C reactive protein (CRP), and leucocyte count (WCC) values for all children
C reactive protein also differed significantly across the five categories of infection (p < 0.0001; Kruskal-Wallis) and was higher in septic shock compared with localised bacterial, viral infection, and controls (p < 0.01, 0.01, and 0.001, respectively), but not bacterial meningitis. However, C reactive protein did distinguish bacterial meningitis from localised bacterial and viral infection (p < 0.05 and 0.01, respectively).
The leucocyte count did not differ significantly across the five categories of infection (p = 0.39; Kruskal-Wallis).
ROC CURVES
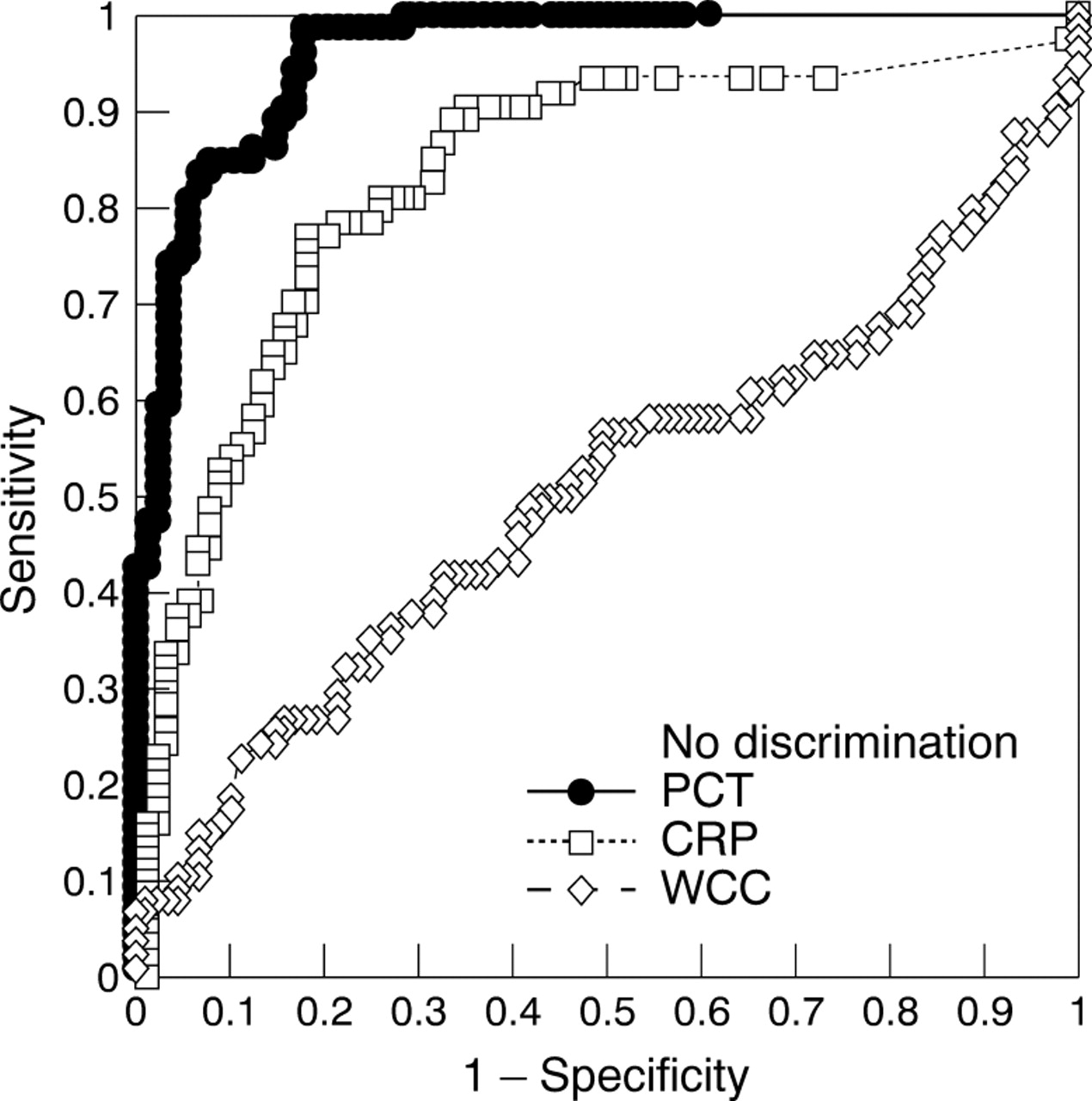
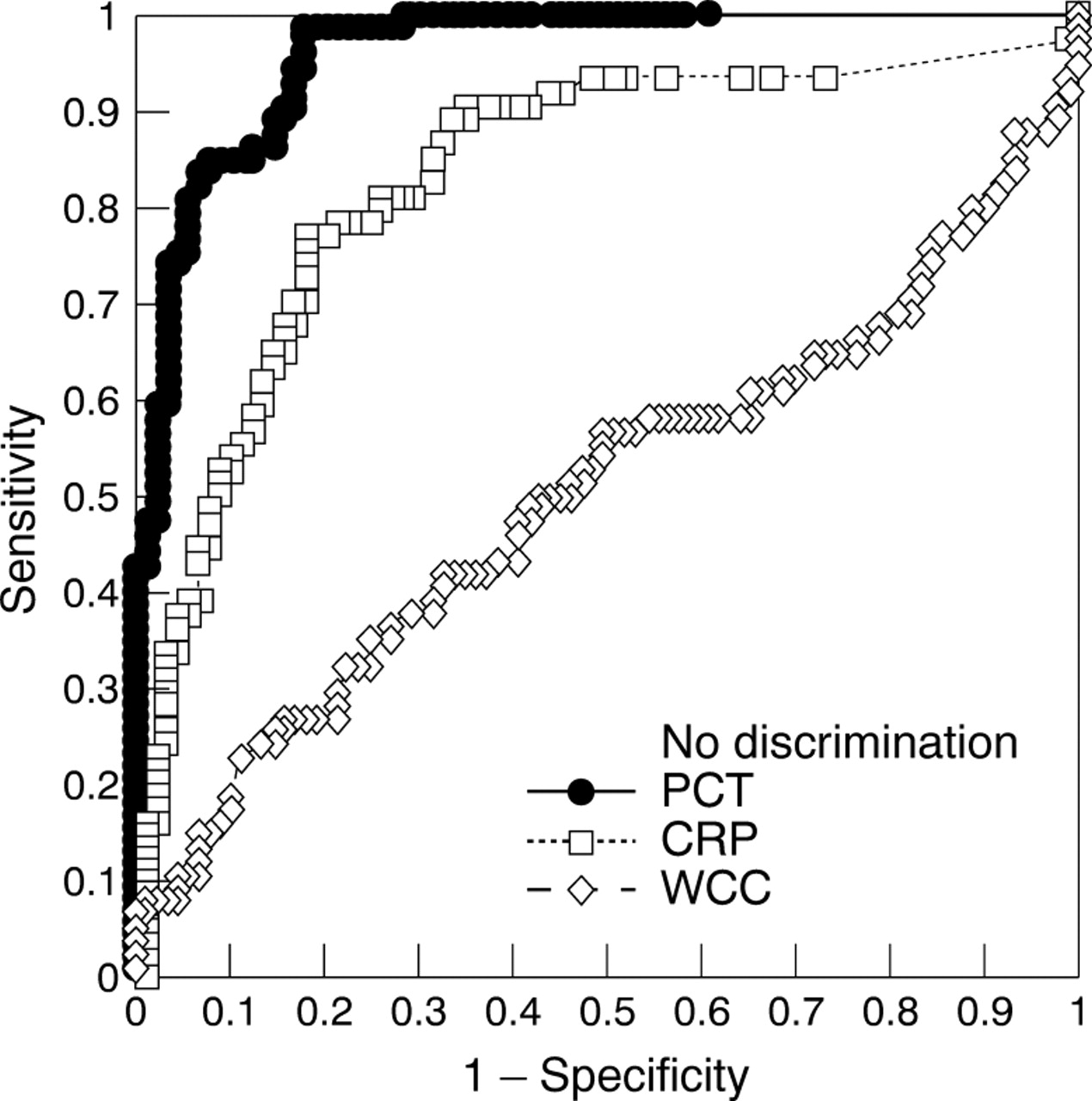
Figure 1 shows ROC curves illustrating the sensitivity and specificity of procalcitonin, C reactive protein, and the leucocyte count for septic shock. The area under the ROC curve was 0.96 for procalcitonin (95% confidence interval (CI), 0.93 to 0.99), compared with 0.83 for C reactive protein (95% CI, 0.76 to 0.90; p < 0.0001), and 0.51 for the leucocyte count (95% CI, 0.41 to 0.60; p < 0.0001). The ROC curve for the leucocyte count did not differ significantly from the line of non-discrimination (p = 0.45).
{kind=link}
Receiver operating characteristic (ROC) curves comparing admission procalcitonin (PCT), C reactive protein (CRP), and leucocyte count (WCC) for prediction of septic shock (all patients). The area under the curve was 0.96 for procalcitonin, 0.83 for CRP, and 0.51 for WCC.
AGE GROUPS
Table 3 shows the area under the ROC curve for procalcitonin in all patients, infants aged less than 3 months, children aged 3–36 months, and children older than 36 months, respectively.
Area under the ROC curve for procalcitonin in septic shock according to age
PREDICTIVE VALUES
Table 4 shows the sensitivity, specificity, and positive and negative predictive values of procalcitonin and C reactive protein for septic shock. Diagnostic cut off levels with the optimum sensitivity and specificity derived from the ROC curve were found to be procalcitonin > 20 ng/ml and C reactive protein > 50 mg/litre. A concentration of procalcitonin > 2 ng/ml had 100% sensitivity and negative predictive value for septic shock, but with specificity and positive predictive value of only 62% and 69%, respectively.
Sensitivity, specificity, positive and negative predictive values (%) of admission PCT and CRP values for septic shock
SEVERE BACTERIAL INFECTION
The range of procalcitonin concentrations in children with bacterial meningitis (range, 7.2–118.4 ng/ml) overlapped that of septic shock (range, 3.3–759.8 ng/ml). Because it is clinically important to differentiate these patients from those with less serious bacterial disease, we then combined both bacterial meningitis and septic shock to form an additional category termed “severe bacterial infection”. Further analysis was performed for sensitivity and specificity in identifying children with severe bacterial infection, yielding an area under the ROC curve of 0.98 (95% CI, 0.96 to 1.0) for procalcitonin. Note that procalcitonin > 2 ng/ml also had 100% sensitivity and a negative predictive value for severe bacterial infection, but with a specificity and positive predictive value of 70% and 78%, respectively.
Discussion
The issue of differentiating patients with severe bacterial sepsis from infants and children with similar non-specific symptoms and signs has generated interest in identifying useful laboratory markers of infection.11-15 Other authors have described “unconventional” inflammatory markers such as fibronectin, interleukin 6, tumour necrosis factor, and β integrins, which have been used as research tools but not gained widespread acceptance in routine practice.25-27
Since Assicot and colleagues first proposed procalcitonin as an early marker of bacteraemia, descriptive reports of procalcitonin measurements in children have been reported.16 18 20More recently, several authors have reported the quantitative evaluation of procalcitonin as a diagnostic marker of bacteraemia and fungaemia, quoting sensitivity and specificity ranging from 57% to 100%, and from 50% to 100%, respectively.19 22 23-30For example, Chiesa et al reported that an abnormal procalcitonin concentration identified early neonatal sepsis with a sensitivity of 92.6% and a specificity of 97.5%.23
Interpretation of the literature dealing with procalcitonin is complicated by variation in the choice of the “abnormal” cut off value, and by the diverse age range and nature of the study populations. Previous studies have suffered from apparent heterogeneity not only within the study group, but also within categories defined as “sepsis”, “distress”, “infected”, “respiratory distress”, or even “haemodynamic failure”.18 20 22Because our own tertiary referral patient population has a low yield from pre-admission blood cultures, possibly as a result of technical factors, it would be impractical to define septic patients only by a gold standard of positive blood culture.31 Despite this limitation, we stress the importance of rigidly defined categories of infection. In our study we have attempted to “capture” children with bacteraemia under the classification of septic shock, and excluded six patients without documented evidence of infection from further analysis.
Objective assessment of any diagnostic marker ideally requires a study population with a high prevalence of disease, and although critically ill children might not be directly comparable with the general paediatric population, the prevalence of bacterial sepsis is high. Thus, we are able to compare a range of procalcitonin cut off values using optimum sensitivity and specificity derived from the ROC curve.
We have shown that procalcitonin rises to very high concentrations early in septic shock, and that an admission procalcitonin value of 20 ng/ml might be used to distinguish children with this condition with high sensitivity and specificity. Because children with bacterial meningitis appear to have procalcitonin concentrations similar to those in septic shock, we may usefully identify these patients on the basis of their admission procalcitonin. The ROC curve illustrates the superior sensitivity and specificity of procalcitonin compared with C reactive protein, as a consequence of the wide range of C reactive protein concentrations in all categories of infection. Our data support the view of some authors that the leucocyte count has little value in differentiating the type of infection in critically ill children.9 10 These findings are based on a single admission measurement, and we acknowledge that sequential testing might improve the diagnostic value of one, or all, of these parameters.
We have shown that procalcitonin has both greater specificity and positive predictive value for septic shock than other commonly used markers, both in the study population as a whole, and for the subgroups of children aged less than 3 months, 3–36 months, and older than 36 months respectively. Critics might argue that knowledge of the procalcitonin value is unlikely to change clinical practice, because these children are likely to receive antibiotic treatment on the basis of clinical suspicion alone. However, we suggest that the value of this investigation lies not in confirming the suspicion of disease, but in helping to exclude severe bacterial disease from the differential diagnosis.
Although a diagnostic value derived from the apex of the ROC curve indicates the optimum combination of sensitivity and specificity, this value might not be the most useful, because a clinician might wish to identify all patients with serious disease at the expense of a high false positive rate. We point out that a procalcitonin concentration > 2 ng/ml has 100% sensitivity and negative predictive value, although only 62% specificity and 69% positive predictive value, respectively, for both septic shock and bacterial meningitis in our study population. It follows that a procalcitonin value of 2 ng/ml might help distinguish severe life threatening bacterial infection from localised and viral disease in febrile children.
This raises the question of whether routine procalcitonin measurement might be useful in the paediatric emergency department. We suggest that procalcitonin measurement has the potential to shorten the duration of both antibiotic treatment and hospital stay for febrile children. However, it remains to be seen whether data derived from our group of critically ill children can be applied to an acute general paediatric population, who might differ in aetiology, severity of disease, and timing of presentation. Indeed, we acknowledge the need for further evaluation of procalcitonin in the emergency department setting, but point out that the low prevalence of severe disease in these children would require a large multicentre study population.
Procalcitonin measurement might provide the clinician with a useful addition to currently available investigations, although given the poor performance of the leucocyte count, and to a lesser extent C reactive protein, it might even be argued that the routine use of these tests is motivated more by low cost, easy availability, and historical practice rather than diagnostic value.
CONCLUSION
The admission procalcitonin concentration has better sensitivity, specificity, and predictive value for septic shock than either C reactive protein or the leucocyte count. The admission leucocyte count has no value in differentiating the type of infection in critically ill children. Procalcitonin measurement might be a useful additional tool for the diagnosis of severe bacterial disease in infants and children.