Article Text

Abstract
Background While it is now clear that paracetamol is ineffective for spinal pain, there is not consensus on the efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for this condition. We performed a systematic review with meta-analysis to determine the efficacy and safety of NSAIDs for spinal pain.
Methods We searched MEDLINE, EMBASE, CINAHL, CENTRAL and LILACS for randomised controlled trials comparing the efficacy and safety of NSAIDs with placebo for spinal pain. Reviewers extracted data, assessed risk of bias and evaluated the quality of evidence using the Grade of Recommendations Assessment, Development and Evaluation approach. A between-group difference of 10 points (on a 0–100 scale) was used for pain and disability as the smallest worthwhile effect, as well as to calculate numbers needed to treat. Random-effects models were used to calculate mean differences or risk ratios with 95% CIs.
Results We included 35 randomised placebo-controlled trials. NSAIDs reduced pain and disability, but provided clinically unimportant effects over placebo. Six participants (95% CI 4 to 10) needed to be treated with NSAIDs, rather than placebo, for one additional participant to achieve clinically important pain reduction. When looking at different types of spinal pain, outcomes or time points, in only 3 of the 14 analyses were the pooled treatment effects marginally above our threshold for clinical importance. NSAIDs increased the risk of gastrointestinal reactions by 2.5 times (95% CI 1.2 to 5.2), although the median duration of included trials was 7 days.
Conclusions NSAIDs are effective for spinal pain, but the magnitude of the difference in outcomes between the intervention and placebo groups is not clinically important. At present, there are no simple analgesics that provide clinically important effects for spinal pain over placebo. There is an urgent need to develop new drug therapies for this condition.
- Low Back Pain
- NSAIDs
- Analgesics
Statistics from Altmetric.com
Introduction
Spinal pain (neck or low back pain) is the leading cause of disability worldwide,1 ,2 and commonly managed in general practice by prescription of medicines.3 ,4 Clinical guidelines recommend non-steroidal anti-inflammatory drugs (NSAIDs) as a second-line analgesic after paracetamol, with third choice being opioids.5 However, recent meta-analyses have shown that paracetamol is ineffective,6 ,7 and opioids appear only to offer small benefits for this condition.8 Thus, although the use of NSAIDs has fallen in the past decade,9 their use could rapidly rise, given the lack of efficacy of paracetamol and increased awareness of risks associated with opioid use.10 ,11
There is still not consensus on the efficacy of NSAIDs for spinal pain. The most recent meta-analysis excluded participants with acute low back pain or neck pain,12 and to date no reviews have investigated NSAID injections or topical formulations in this population. Furthermore, previous meta-analyses have reported standardised mean differences (MD) as effect sizes, which are non-intuitive and difficult to interpret;13 thus better measures of treatment effects, such as numbers needed to treat (NNT), are likely to enhance interpretability for the clinician. There is also concern about the cardiovascular safety of cyclo-oxygenase-2 (COX-2) inhibitors, while serious gastrointestinal adverse reactions are more closely linked to non-selective NSAIDs,14 although all NSAIDs have been associated with cardiovascular and gastrointestinal risks.15 Thus, there is far greater need to understand the efficacy and safety of this medicine for spinal pain.
Therefore, the aim of this systematic review was to investigate the efficacy and safety of NSAIDs compared with placebo in patients with spinal pain, with or without radicular pain. We also aimed to evaluate whether trial characteristics or methods are associated with estimates of treatment effect.
Methods
Literature search
We followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) statement,16 and prospectively registered the review protocol on the International Prospective Register of Systematic Reviews (CRD42015023746). We searched MEDLINE, EMBASE, CINAHL, CENTRAL and LILACS from their inception to February 2016. The search strategy was constructed based on a combination of the following keywords and their variations: neck pain, back pain, lumbago, sciatica, anti-inflammatory, placebo and randomised controlled trial. There were no restrictions of language or publication period. Translations were obtained for non-English studies (two trials). The complete search strategy is shown in online supplementary table S1. One author (GCM) performed the first selection of studies based on titles and abstracts, and two authors (GCM and MBP) independently screened full texts. We also searched for potentially eligible trials in the reference lists of included studies and relevant systematic reviews. We used consensus to resolve any disagreement.
supplementary tables
Study selection
Only randomised placebo-controlled trials published in peer-reviewed journals and investigating the effects and safety of NSAIDs for spinal pain were included in this review. Trials had to include participants with neck or low back pain, with or without radicular pain. Trials that included mixed populations were included if they reported separate data for participants with spinal pain. We included trials investigating acute or chronic spinal pain of any intensity and eligible trials had to compare any class, formulation or route of administration (topical, oral or injection) of NSAIDs with a matching placebo. Only trials that reported patient-relevant outcomes, such as pain intensity, disability status, quality-of-life or adverse events were included. The dose and frequency of NSAIDs intake were not restricted, and we investigated the effects of both non-selective NSAIDs (eg, acetic acids, enolic acids, propionic acids, salicylates) and COX-2 inhibitors. We excluded trials of participants with serious spinal pathology (cancer, infectious diseases or cauda equina syndrome). Trials evaluating postoperative analgesia using NSAIDs in participants with spinal pain were excluded, as were non-randomised controlled trials, review articles, guidelines and observational studies.
Data extraction and quality assessment
We used a standardised data extraction form to record the characteristics of included participants, NSAID class and dose, route of administration, outcomes and duration of follow-up. Two reviewers (GCM and MBP) independently recorded the sample size, means and SDs for pain, disability and quality-of-life measures. We extracted these data following a hierarchical order: mean difference (MD), change scores and post-treatment scores. When medians, IQRs, ranges or SEs were reported, we used previously reported formulae to estimate means and SDs.17 According to recommendations in the Cochrane Handbook,18 we extracted data from the first period of crossover randomised trials, and in multi-arm trials we extracted data from all groups and divided the number of participants in the control group by the number of comparisons.
For the safety outcomes, we extracted the number of participants reporting any adverse event, any serious adverse event (as defined by each trial or events including myocardial infarction and/or stroke), the number of dropouts due to adverse events and the number of participants reporting gastrointestinal adverse reactions. We also extracted the number of participants taking additional analgesics and the number of tablets consumed per day. We contacted authors of included trials to clarify any relevant information or to request additional data in case of incomplete reporting. Consensus or a third reviewer (MLF) was used to resolve any disagreement.
The Cochrane Collaboration's tool was used to assess the risk of bias of included studies by two independent reviewers (GCM and MBP).19 The quality of the evidence from each pooled analysis was evaluated using the Grade of Recommendations Assessment, Development and Evaluation (GRADE) approach.20 The quality of evidence was downgraded by one level according to the following criteria: limitation of study design (more than a quarter of studies considered at serious risk of bias), inconsistency of results (substantial heterogeneity, I2>50%), imprecision (pooled sample size <300), indirectness (dissimilar population, intervention, outcomes and time points) and publication bias (funnel plot assessment and Egger's test two-tailed p<0.1). Consensus was used to resolve any disagreement. The quality of evidence was then judged as high, moderate, low or very low.
Data synthesis and analysis
Trials were pooled for common outcomes and time points. As our primary analysis we present overall pooled estimates including all available trials, and as a secondary analysis we present separate pooled effects for neck pain, acute/chronic low back pain and sciatica. We defined a follow-up period <2 weeks as immediate-term, and a follow-up between 2 weeks and 3 months as short-term. When more than one time point was available for the same definition, we extracted data at 1 week for immediate-term, or at 8 weeks for short-term. Although we attempted to extract data for medium (>3 months but <12 months) and long-term (≥12 months) follow-ups, no trials reported data for these time points.
Pain outcome measures reported in included trials were visual analogue scales (range, 0–100), or numerical rating scales (range, 0–10). These two pain measures are highly correlated and can be used interchangeably when transformed.21 The disability scale used in trials was the Roland-Morris Disability Questionnaire (range, 0–24). Pain and disability scores were converted to a common 0-point (no pain or disability) to 100-point (worst possible pain or disability) scale to facilitate the interpretation of our results, and because smallest worthwhile effects for pain and disability in this population are often reported in a 0–100 scale.22–24 Quality-of-life measures included the 12-item or the 36-item Short Form (SF) Health Survey (range, 0–100); no score conversion was needed for this outcome.
A between-group difference of 10 points (on a 0–100 scale) for pain, disability and quality-of-life was considered as the smallest worthwhile effect;22 the mean effect sizes below this threshold were considered clinically unimportant. The smallest worthwhile effect describes the smallest effect of intervention (compared with placebo) that patients perceive as important, and is critical for clinical decision-making.25 We used random-effects models to calculate MD or risk ratios (RR) and 95% CIs. We also present the results for the pain intensity analyses as numbers needed to treat (NNT), using the method proposed by Norman.26 This expresses the number of patients who need to be treated with an NSAID rather than placebo, for one additional person to benefit (based on a clinically important change of 10 points on a 0–100 pain scale; and allowing for the proportion of patients who were improved, the same and deteriorated in NSAID and placebo groups). All analyses were conducted using Comprehensive Meta-Analysis V.2 (Biostat, Englewood, New Jersey, USA).
Secondary exploratory analysis
We conducted subgroup analyses to explore the influence of different factors on our estimates of treatment effects. We used meta-regression to generate the difference in effect sizes (with 95% CI) and p values between subgroups for pain at immediate-term. Subgroups were defined in terms of risk of bias judgements (low, unclear or high), form of drug administration (topical, oral or injection) and type of NSAID (COX-2 inhibitors or non-selective NSAIDs). We also investigated the difference of effect sizes of discontinued drugs (eg, rofecoxib and valdecoxib) and currently marketed NSAIDs, given the aim of this review in informing current best practice.
Results
Initial search and results
Our search resulted in a total of 5208 individual records. After the screening of titles and abstracts, two independent reviewers assessed 302 full-text articles. We included 35 randomised trials after full-text examination with data for 6065 participants with spinal pain (figure 1).27–61 Twenty-two trials investigated the effects of NSAIDs for low back pain, of which 11 included participants with acute back pain and 11 (10 published reports) included participants with chronic low back pain. Eleven trials investigated participants with sciatica and two included neck pain only. The median treatment duration in included trials was 7 (IQR, 5–7) days. NSAIDs were mostly administered orally, but five trials used intravenous or intramuscular injection,35 ,37–39 ,59 and three used a topical formulation, such as a gel, patch or cream.51 ,53 ,56 Nine trials had a three-arm parallel design and two were randomised crossover trials. These trials compared two different drugs, or two different dosages of the same drug with a matching placebo. Online supplementary table S2 provides more detail on the characteristics of included trials and the medications evaluated.

Study selection. CENTRAL, Cochrane Central Register of Controlled Trials. *Number of citations listed for each database includes duplicates.
The risk of bias assessment (see online supplementary figure S1) shows that overall, studies had no serious risk of bias. However, about half of the trials had at least one bias domain judged as high risk. A third of included trials reported an appropriate method of randomisation, and only four reported suitable allocation concealment. Nearly all trials were therapist and assessor-blinded, but 20% of trials had high dropout rates (>15%). Seven trials did not report relevant outcomes or failed to report results previously described in their methods and were judged at high risk of reporting bias. Eleven trials were judged at high risk for the ‘other’ bias domain as they reported that pharmaceutical companies that funded the trial were involved in running the study, analysing the data or writing the manuscript. The risk of bias assessment for each individual trial is shown in online supplementary figure S2. The inspection of the funnel plot including all trials reporting data for immediate pain reduction and the non-significant Egger's test (p=0.86) revealed no publication bias (see online supplementary figure S3). Therefore, none of our meta-analyses was downgraded for publication bias according to the GRADE approach. Data extracted from individual trials and calculations of effect sizes are shown in online supplementary tables S3 and S4.
supplementary figures
Efficacy of NSAIDs for spinal pain
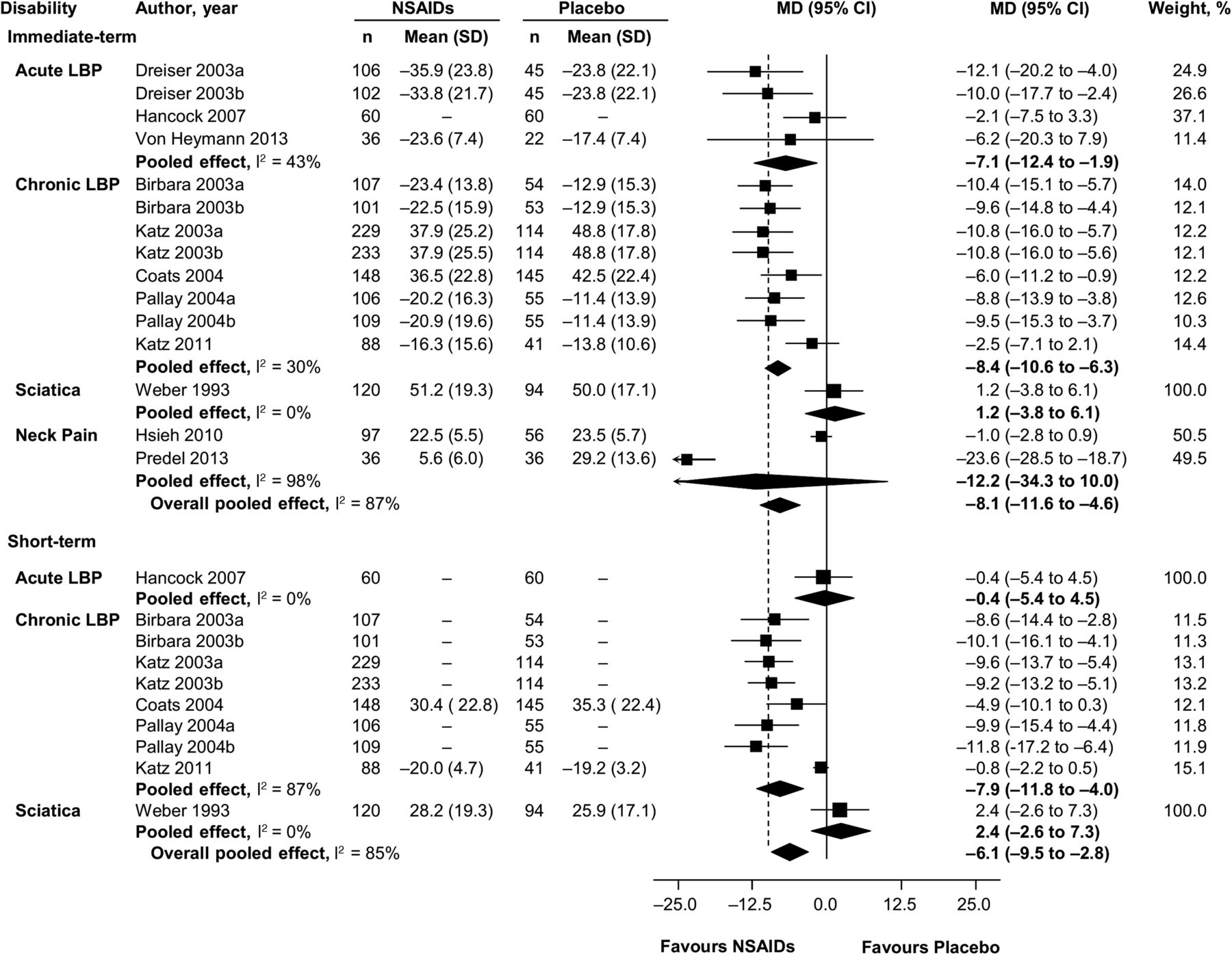
Pooling of all included trials revealed moderate-quality evidence that NSAIDs reduced pain in the immediate (MD −9.2, 95% CI −11.1 to −7.3) and short-term (MD −7.7, 95% CI −11.4 to −4.1) compared with placebo (figure 2). The NNT to achieve a clinically significant effect of NSAIDs over placebo on pain reduction in the immediate-term was 5 (95% CI 4 to 6) and 6 (95% CI 4 to 10) in the short-term. The effects of NSAIDs on disability were slightly smaller than for pain, with effect at immediate-term follow-up being −8.1 (95% CI −11.6 to −4.6), and at short-term −6.1 (95% CI −9.5 to −2.8) (figure 3). The magnitude of the difference in outcomes between the intervention and placebo groups, however, was less than the 10-point threshold for clinical importance.

Mean differences for pain in placebo-controlled trials on efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for spinal pain. Pain is expressed on scale of 0–100. Immediate-term=follow-up ≤2 weeks; short-term=follow-up >2 weeks but ≤3 months; LBP, low back pain. Studies ordered chronologically within subgroups.

Mean differences for disability in placebo-controlled trials on efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) for spinal pain. Disability is expressed on scale of 0–100. Immediate-term=follow-up ≤2 weeks; short-term=follow-up >2 weeks but ≤3 months; LBP, low back pain. Studies ordered chronologically within subgroups.
There was high-quality evidence of clinically unimportant effects of NSAIDs compared with placebo for the physical component of the SF-12 (MD −2.9, 95% CI −3.7 to −2.1), and no effects over placebo were found for the mental component (MD −0.3, 95% CI −1.2 to 0.6). None of the included studies used the SF-36 to measure quality-of-life. Table 1 provides more detailed information on the summary of findings and the GRADE assessment. None of the included trials reported medium-term or long-term effects of NSAIDs.
Summary of findings and quality of evidence assessment
Safety of NSAIDs for spinal pain
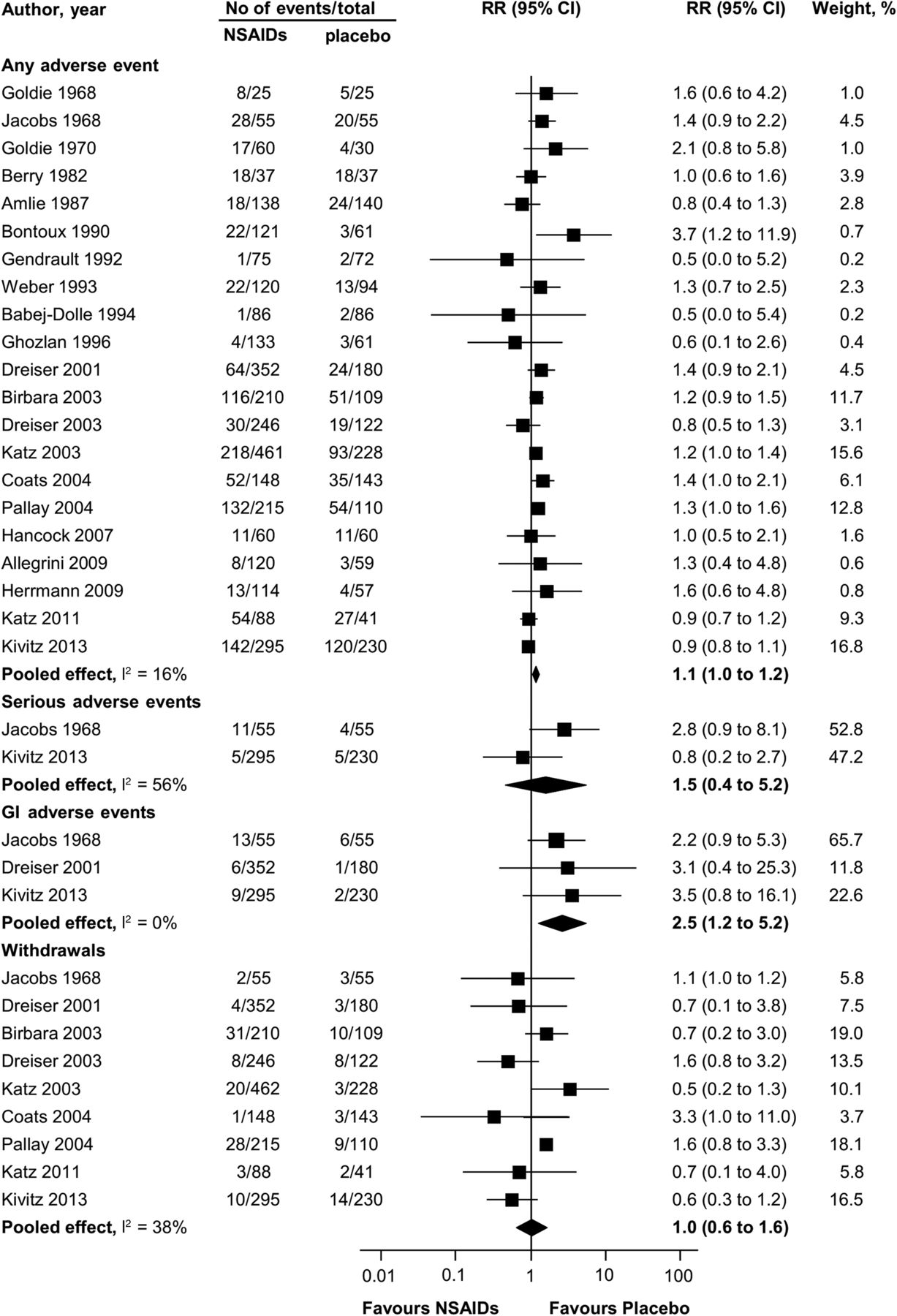
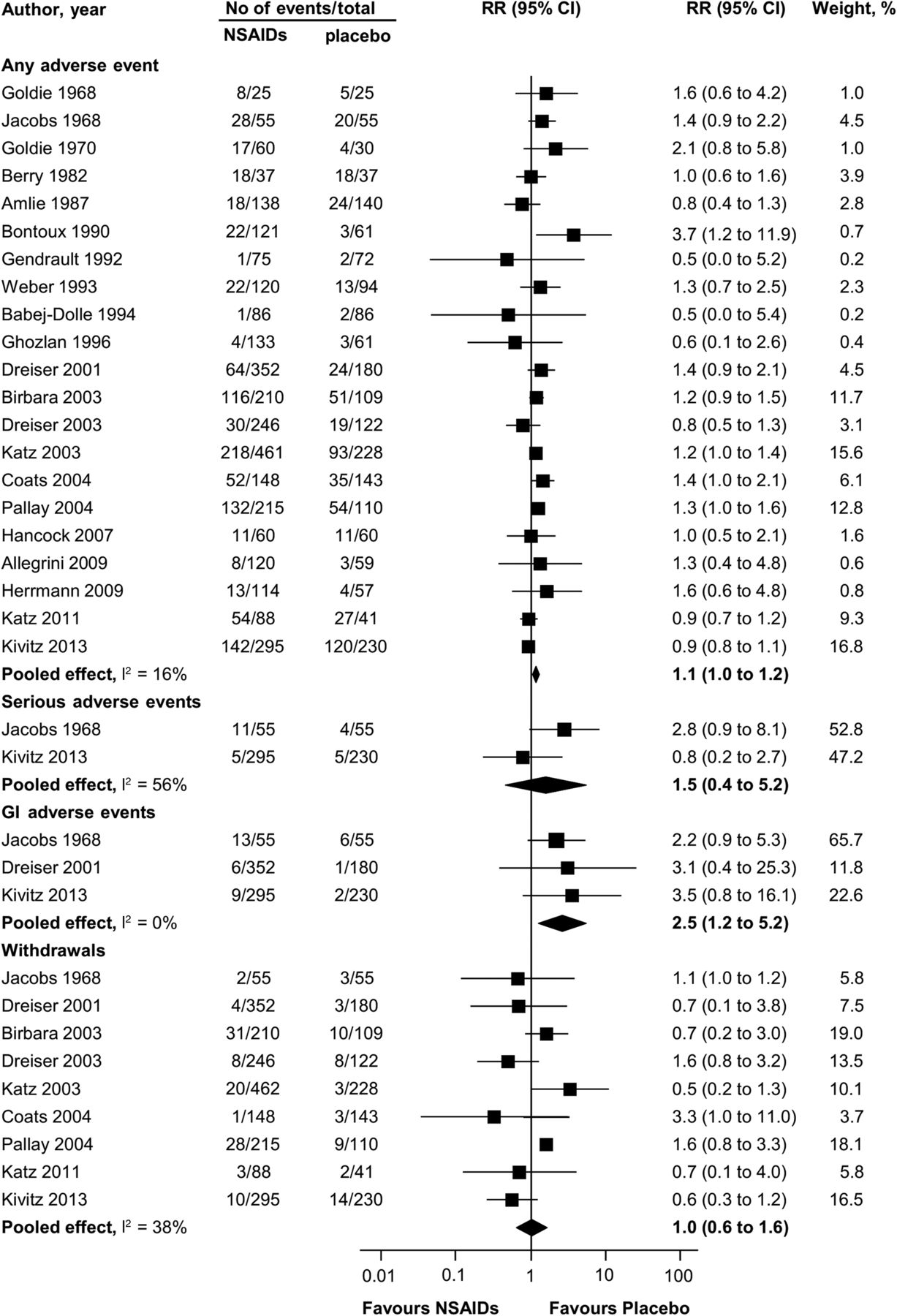
For the safety analyses, we included up to 21 trials (5153 participants) with median treatment duration of 7 (IQR, 5–7) days (figure 4). No difference in any event rate between NSAIDs and placebo was found (RR 1.1, 95% CI 1.0 to 1.2). Only two trials including 635 participants reported serious adverse event data and again there was no difference between groups (RR 1.5, 95% CI 0.4 to 5.2). Similarly, nine trials with 3283 participants revealed no difference in the number of dropouts due to adverse events (RR 1.0, 95% CI 0.6 to 1.6). However, we found a significantly higher number of participants in the NSAIDs group reporting gastrointestinal adverse events compared with placebo (RR 2.5, 95% CI 1.2 to 5.2); 28/702 participants taking NSAIDs had gastrointestinal adverse reactions compared with 9/465 in the placebo groups. Overall, these results were based on high-quality evidence according to the GRADE evaluation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk ratio for safety outcome measures in placebo-controlled trials on efficacy of non-steroidal anti-inflammatory drugs (NSAIDs) compared with placebo. Any adverse event=no. of patients reporting any adverse event; serious adverse events=no. of patients reporting any serious adverse event (as defined by each study); GI adverse events=no. of patients reporting gastrointestinal adverse events; withdrawals=no. of patients withdrawn from study because of adverse events. Studies are ordered chronologically within subgroups.
Use of rescue medication
The use of rescue medication was measured in a variety of ways in eight trials, such as the number of participants taking additional analgesics and the number of tablets taken per day. Four trials revealed moderate-quality evidence of no difference in the number of participants taking an additional analgesic (RR 1.0, 95% CI 0.6 to 1.4). However, pooling of four trials showed high-quality evidence that participants taking NSAIDs required less tablets/day of a rescue medication (MD –0.4, 95% CI −0.5 to −0.3), a difference that is arguably not clinically important.
Secondary exploratory analysis
Results from our meta-regression analyses showed that trials with low risk of selection bias had larger effects (MD −11.2, 95% CI −13.9 to −8.5) than trials judged at unclear risk (MD −6.7, 95% CI −8.6 to −4.9). The difference between these subgroups (MD −4.2, 95% CI −7.7 to −0.8) was statistically significant (p=0.02). COX-2 inhibitors had larger effects (MD −13.4, 95% CI −15.7 to −11.1) compared with non-selective NSAIDs (MD −7.7, 95% CI −9.8 to −5.6). This difference was also statistically significant (MD −5.7, 95% CI −9.4 to −1.9; p=0.003), but of questionable clinical relevance. There was no difference between the effect sizes of discontinued drugs compared with currently marketed NSAIDs (MD 0.3, 95% CI −3.7 to 4.3; p=0.88), although no trials investigating celecoxib were found (table 2). Different delivery routes resulted in similar effects compared with a matching placebo: topical (MD −13.2, 95% CI −18.5 to −7.9), oral (MD −8.5, 95% CI −10.4 to −6.6) and injection (MD −9.5, 95% CI −14.7 to −4.4).
Secondary exploratory analyses for pain at immediate-term
Discussion
Our review of 35 randomised placebo-controlled trials demonstrates that NSAIDs are effective in reducing pain and disability in patients with spinal pain, although treatment effects above those of placebo are small and arguably not clinically important. For every six patients treated with NSAIDs, rather than placebo, only one additional patient would benefit considering a between-group difference of 10 points for clinical importance in the short-term. Furthermore, when looking at different spinal pain, outcomes or time points in only 3 of the 14 analyses were the pooled effects only marginally above our 10-point threshold for clinical relevance. NSAIDs were associated with higher number of patients reporting gastrointestinal adverse effects in the short-term follow-up (ie, <14 days). No data on safety at medium-term or long-term follow-ups were provided by included trials.
The strengths of our review include that it was prospectively registered and followed the PRISMA recommendations, including the use of GRADE to appraise the quality of the evidence. We were able to identify a significantly larger number of trials than past reviews,12 ,62–70 which have often limited their inclusion criteria to a specific language, population or type of NSAID. Including more studies (35 randomised placebo-controlled trials) enabled us to conduct a more thorough evaluation of the effects of NSAIDs for various forms of spinal pain, and to include a range of forms of drug administration. We have also provided valuable information on pooled treatment effects for specific populations, including neck pain, acute/chronic low back pain and sciatica. Furthermore, we have provided clinically interpretable estimates on a 0–100 scale, and compared our effect sizes with a predetermined smallest worthwhile effect of 10 points, which reflects the smallest effect of the intervention on outcomes compared with placebo that patients would consider meaningful or important.22 Given physicians often find the interpretation of effect sizes reported in meta-analysis challenging,71 we have also presented our results on pain reduction as the NNT for a clinically significant effect of NSAIDs over placebo. Moreover, potential factors that could have influenced our treatment effects, such as risk of bias judegments, class of NSAIDs and route of administration, were investigated through meta-regression analyses. Although COX-2 inhibitors showed larger effects than non-selective NSAIDs on pain reduction, the size of the difference is of arguable clinical relevance. COX-2 inhibitors trials included in our review were fairly recent (all were conducted after 2003) and substantially larger (mean sample size of 280). They were also more likely to report safety outcomes than older trials.
Our review has some limitations. First, we did not find any trials investigating the efficacy and safety of celecoxib versus placebo, a commonly used COX-2 selective drug. Second, some of the trials included in our meta-analysis used drugs that are discontinued or are no longer commercialised in major markets (eg, rofecoxib and valdecoxib), but our meta-regression revealed that this was not a factor that influenced our estimates; discontinued drugs (MD −8.9, 95% CI −10.8 to −7.0) had similar effects as currently marketed NSAIDs (MD −9.3, 95% CI −12.1 to −6.5). Third, there is no evidence on the long-term effects and safety of NSAIDs, as the median follow-up time was 1 week in included trials, with some treatment schedules lasting <1 day. Fourth, our overall pooled estimates resulted in substantial between-trial heterogeneity (I2 ranged from 59% to 87%), which, however, was found considerably reduced in the stratified meta-analyses according to the type of spinal pain (ie, neck pain, acute/chronic low back pain, or sciatica). Finally, another limitation of our study is that there were very few trials on neck pain, and none on whiplash.
We provide sound evidence that NSAIDs are effective, but do not offer clinically important benefits for spinal pain above those attributable to placebo, given overall pooled estimated differences were <10 points. This is crucially important because we now know paracetamol is ineffective,6 ,7 and opioids only offer small benefits for spinal pain.8 Thus, given our results and evidence from these recent high-quality meta-analyses, it seems that there are no analgesics with clinically important effects over placebo for spinal pain. This is a problem, as current guidelines for spinal pain endorse these three medicines.5 For instance, the National Institute for Health and Care Excellence (NICE) guidance on low back pain and sciatica now recommends NSAIDs as first analgesic option and suggests the use of opioids with paracetamol to treat spinal pain. In our review, even when the effects of NSAIDs were analysed for different spinal pain strata (ie, neck pain, acute/chronic low back pain or sciatica), only 3 of the 14 analyses revealed effects that were marginally above our threshold for clinical relevance. The effects observed in trials including participants with neck pain were unexpected, particularly because these trials investigated topical NSAIDs only. Our safety analysis revealed that NSAIDs increased the risk of gastrointestinal adverse effects by 2.5 times compared with placebo, although safety data were limited to trials that used non-selective NSAIDs. However, it is established that all NSAIDs, including COX-2 inhibitors, have been linked to gastrointestinal harms.15 ,72 Our safety results should be interpreted with caution given the short duration of exposure to NSAIDs in included trials.
In summary, compared with placebo, NSAIDs do not provide a clinically important effect on spinal pain, and six patients must be treated with NSAIDs for one patient to achieve a clinically important benefit in the short-term. When this result is taken together with those from recent reviews on paracetamol and opioids, it is now clear that the three most widely used, and guideline-recommended medicines for spinal pain do not provide clinically important effects over placebo. There is an urgent need to develop new analgesics for spinal pain.
References
Footnotes
Handling editor Tore K Kvien
Twitter Follow Gustavo Machado @gustavocmachado
Contributors All authors made substantial contributions to the study conception and design or analysis and interpretation of data and were involved in drafting the manuscript and approved the final version.
Funding GCM and MBP are supported by an Australian Postgraduate Award from the Department of Education and Training of Australia. CGM is supported by a Principal Research Fellowship from the National Health and Medical Research Council. MLF holds a Sydney Medical Foundation Fellowship, Sydney Medical School.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.