Article Text

Abstract
Objective In light of an emerging epidemic identified in the United States and Canada, to identify trends in fatal drug toxicity involving oxycodone and the demographic characteristics and indicators of socioeconomic disadvantage of the deceased.
Study design Population-based observational study in Victoria, Australia.
Population Decedents whose death was reported to the Victorian Coroner between 2000 and 2009 and where oxycodone was detected.
Main outcome measures Association between supply of oxycodone and deaths. Demographic characteristics of decedents. Rate ratios of the rural or metropolitan location and socioeconomic indicators of disadvantage of the deceased.
Results Supply to Victoria has increased nine-fold from 7.5 mg per capita in 2000 to 67.5 mg per capita in 2009. Detection of oxycodone in deaths reported to the Victorian Coroner has increased from 4 (0.08/100 000 population) in 2000 to 97 (1.78/100 000 population) in 2009—a 21-fold increase in deaths. Of the 320 cases described, 53.8% (172) were the result of drug toxicity. Of these, 52.3% were unintentional and 19.8% intentional self-harm; the remaining 27.9% are either still under investigation by the coroner or intent is unknown. Drug toxicity deaths were overrepresented in both rural areas and areas indexed with high levels of disadvantage.
Conclusions The substantial increase in the number of deaths involving oxycodone is strongly and significantly associated with the increase in supply. Most drug toxicity deaths involving oxycodone were unintentional. This newly identified trend in fatalities in Victoria supports concerns that a pattern of increasing deaths involving oxycodone is emerging globally.
- Alcohol/drugs
- poison see ingestion
- public health
- socio economic status
Statistics from Altmetric.com
Introduction
Chronic pain is prevalent in Australia1 and globally, and while treatment can include non-drug and non-opioid drug options, opioid analgesics are frequently prescribed. There has been a substantial global increase in consumption of prescription opioids. The consumption of opiate analgesics such as morphine and oxycodone has increased from 143 million S-DDD (defined daily doses for statistical purposes) in 1997 to 943 million S-DDD in 2008.2 In Australia there has been a notable increase in the supply of oxycodone, from 92 kg in 1997 to 1295 kg in 2008.3 There is concern that non-medical use of prescription opioids is now a major public health problem.4 5
Indicators of misuse: United States
A strong relationship between increased prescription opioid supply and misuse,6 medical emergencies involving non-medical use,7 and drug poisoning deaths8 has been described in the United States. A 2009 survey of drug use found that an estimated 5.3 million adults in the United States had used pain relievers non-medically in the past month, an increase of 20% from the 2002 estimate of 4.4 million. An estimated 1.9 million reported past year dependence on or abuse of pain relievers.9 Between 1997 and 2007, admissions for treatment of ‘abuse’ rose by 456% for opioid analgesics and 5% for heroin10; there was a 111% increase in emergency department attendances for problems involving the non-medical use of opioid analgesics from 2004 to 2008,11 with the greatest increase for oxycodone products (152%). The number of fatal poisonings involving opioid analgesics more than tripled from 1999 to 2006, outnumbering the combined number of deaths involving the illicit drugs cocaine and heroin.12 Many prescription opioid poisoning deaths involve diversion of these drugs from licit to illicit use.13 However, problematic users of pharmaceutical opioids may differ from heroin users,14 and they may be a heterogeneous group including both medical and non-medical users.15
Indicators of misuse: Australia
There has been a substantial increase in the number, formulations, and prescriptions of opioids in Australia since 1992,16 leading to concerns about problematic use and harm.17 Several Australian indicators suggest a developing problem; however, published evidence about these problems is scarce. Illicit use and injection of prescription opioids is widespread among injecting drug users,18–20 and an increasing proportion of individuals seeking treatment for opioid dependence in Queensland nominate prescription opioids as their primary drug of concern.21 Hospital treatment of poisoning due to opioids has changed between 1998/99 and 2006/07, with a 67.6% decrease in the number of separations for poisoning by heroin (ICD-10 code T40.1) and an increase of 170.2% and 1403.7% for poisoning by other opioids (T40.2) and other synthetic narcotics (T40.4), respectively.22
A number of published studies use medical examiner or coroner's data to investigate drug related deaths.13 23–25 Some studies have also examined indicators of socioeconomic disadvantage,13 as well as rural versus urban locations of the deceased to understand where preventive interventions may be best targeted.13 25–27 Morphine injection by injecting drug users is more prevalent in areas where heroin is less available, such as rural areas,28 and US studies suggest that people who live in disadvantaged areas13 or are disadvantaged26 are also likely to have an increased risk of overdose death involving prescription opioids.
This paper examines deaths where oxycodone was detected because of local and international concerns about its misuse. In addition, the sole clinical use for oxycodone is as an analgesic, unlike methadone which is also used as pharmacotherapy for opioid dependence. Morphine may be present in postmortem samples as a metabolite of heroin. There have been fewer deaths involving other opioids. This paper seeks to: (1) describe trends in deaths involving oxycodone reported from 2000 to 2009 and measure the association with Victorian supply; and (2) categorise and describe the epidemiology of these deaths in the period 2003–09.
Method
Oxycodone detection
The Victorian Coroners Act 2008 defines a reportable death as that suspected to be unnatural, the result of injury, of someone in custody, or where a medical practitioner is unable to sign a death certificate. The Victorian Institute of Forensic Medicine (VIFM) serves a population of over 5 million people. All coroners' cases are subjected to routine toxicological screening tests for ethanol and other small volatile compounds in blood by gas chromatography (GC), drugs of abuse in urine and/or blood using immunoassay techniques, and common drugs of abuse and prescription drugs by GC–mass spectrometry. All positive detections were confirmed by subsequent tests. Drugs of abuse included opioids such as morphine, oxycodone, and methadone, as well as cocaine and metabolites, cannabis and metabolites, benzodiazepines, and amphetamines. Oxycodone was quantified by GC–MS using selected ion-monitoring (SIM).
Opioid-related deaths often occur over a prolonged period during which drugs are metabolised, sometimes resulting in low postmortem concentrations. For this reason, any detection of oxycodone in urine, blood, or tissue was considered sufficient for inclusion in this study. Cases where the remains were decomposed were excluded because decomposition compromises the interpretation of toxicology findings. Cases where oxycodone was detected only in hair were also excluded, as this does not indicate use proximal to death.
Trends in oxycodone supply and deaths
Cases were identified using the National Coroners Information System (NCIS) Victorian Drugs Module (VDM) which identifies all coronial deaths from 2003, and the VIFM toxicology database for cases prior to 2003. The Office of Chemical Safety and Environmental Health monitors supply and movement of Schedule 8 drugs including opioids in Australia,29 and this source was used to measure the association between oxycodone supply and trends in deaths reported to the Victorian Coroner from 2000 to 2009 where oxycodone was detected in toxicology.
Population-based observational study
There were 327 cases where oxycodone was detected in toxicology for the period 2003–09. Six decomposed cases and one case where oxycodone was detected only in hair were excluded. In the remaining 320 cases, the autopsy report, brief police description of circumstances, and coroners' findings were examined to categorise the manner of death, and whether deaths involving drug toxicity were intentional or unintentional.
Most cases were categorised by reviewing the coronial documents mentioned above. Specific key points of reference included cause of death statements and descriptive comments in autopsy reports (where available), and/or coroners' determinations. Thirty-two cases were referred to a panel in order to canvas a wider expert opinion on appropriate categorisation. In some cases this may have been where autopsies were not conducted because of a request from the next of kin. In other instances the pathologist did not mention the contribution of drugs to the cause of death, despite the presence of potentially lethal levels reported in toxicology results. Discordance in opinion between forensic toxicologists and pathologists in establishing a cause of death in cases involving poisoning has been reported in the USA.30 The panel therefore included representation from a range of forensic specialisations including a pathologist, toxicologist, epidemiologist, and public health physician. The panel agreed on categorisation into the following categories:
Drug toxicity: Where the cause of death was listed by the forensic pathologist as drug related, ie oxycodone toxicity or multiple drug toxicity, or where drugs were deemed by our panel to have caused death.
Natural disease, where drugs were contributory: While significant natural disease was present at autopsy, toxicology results showed concentrations above therapeutic range, and at level(s) considered potentially lethal. It was difficult to clearly exclude the role of drugs in contribution to death.
Natural disease: Where natural disease was deemed to have caused death. Some natural cases also included cases of substance users whose natural disease may have been significant, however drugs were not clearly linked to the proximate cause of death.
Other external causes: These included other injury cases where oxycodone detection was incidental, such as death caused by hanging, or motor vehicle trauma.
Unknown: Cases where all experts were unable to ascertain cause of death.
Drug toxicity cases involving oxycodone were further categorised by intent:
Unintentional: Cases where toxicity was accidental, as determined by the coroner.
Intentional self-harm: Determination of intent was typically taken from coroners' findings. Where the coroner was silent about intent despite persuasive evidence (such as the presence of a suicide note or extremely excessive consumption of drugs), the death was considered intentional by the panel.
Unknown intent: Where the coroner was unable to determine intent, and there were no other obvious indications of intent.
Still enquiring: Active cases where the coroner has not yet published a finding and there were no other obvious indications of intent.
As an indicator of socioeconomic disadvantage, the residential address of the deceased was matched to the 2006 Australian Bureau of Statistics (ABS) census collection district level rankings of the Victorian index of relative socioeconomic disadvantage (IRSD), a summary measure of a range of indicators of disadvantage. A low score indicates that the area has many people with low levels of education, employed in low skilled jobs, or many households with low income. IRSD deciles were converted into quintiles, from quintile 1 (most disadvantaged) to quintile 5 (least disadvantaged). The usual residential address of this decedent population was allocated to a rural or metropolitan area according to ABS classification and compared to the distribution of the entire Victorian population.
Statistical analysis
A t-test compared mean ages between intentional and unintentional toxicity categories. The proportion of females, and proportion unemployed and on other government benefits, was compared between these same categories with a χ2 test. A Poisson regression model was used to relate number of deaths to the supply of oxycodone. To evaluate whether the drug toxicity cases were uniformly distributed across Victorian IRSD quintiles, a one-sample Pearson χ2 statistic was used. Total drug toxicity incidence rate ratios in each quintile were tested using Poisson regression. A Poisson regression also provided rate ratio CIs for each quintile. A one-sample test of proportions was used to assess whether the residential address of decedents reflected the split by rural and metropolitan location of the Victorian population. Stata V.11 was used to analyse the data.
Ethical approval was granted by the human research ethics committees of the Victorian Department of Justice, VIFM, and Monash University.
Results
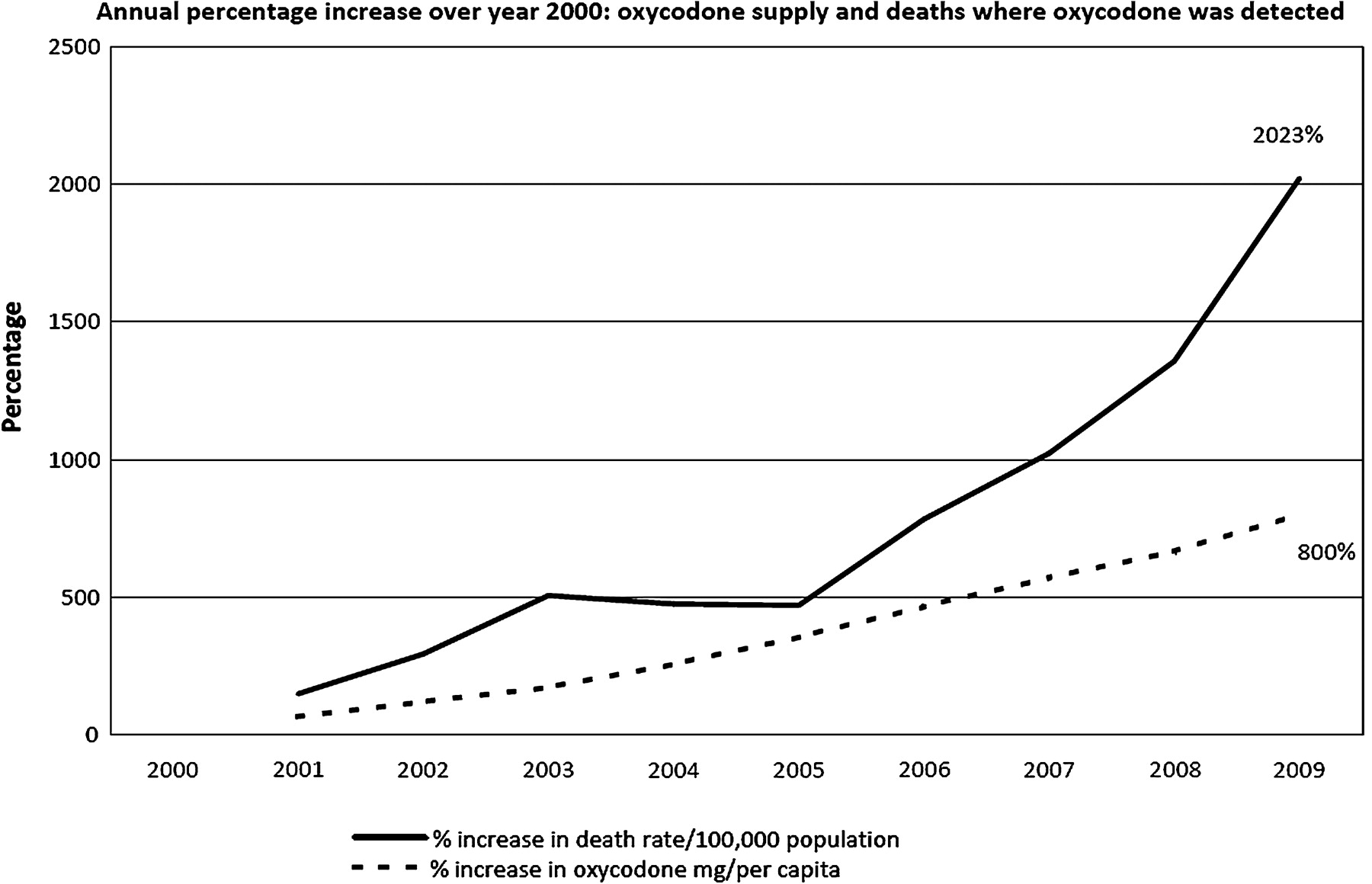
Oxycodone supply to Victoria has increased substantially since the introduction of new formulations, including the sustained release product, OxyContin, in 2000. For the period 2006–08 oxycodone accounted for 19.9% of all consumption of narcotic drugs in Australia as described in defined daily doses for statistical purposes (S-DDD) (2058 S-DDD per million population of oxycodone out of a total of 10 360 S-DDD).2 Supply to Victoria has risen from 35.7 kg (7.5 mg per capita) in 2000 to 367.3 kg (67.5 mg per capita) in 2009, representing a nine-fold increase. Detection of oxycodone in deaths reported to the Victorian Coroner has increased from 4 in 2000 (0.19/100 000 population) to 97 in 2009 (1.78/100 000 population); a 21-fold increase. Figure 1 shows the annual percentage increase above the year 2000 levels. The number of deaths almost doubled (incidence rate ratio 1.95) for every 100 kg increase in supply (p<0.001, CI 1.76 to 2.15).
{kind=link}
Coronial deaths involving oxycodone and oxycodone supply, Victoria, 2000–09.
Table 1 shows the categories of deaths involving oxycodone for the 320 decedents during the seven year period 2003–09. Of these, the cause of death for 172 decedents was attributed to drug toxicity alone, although in a further 19 cases drug toxicity was considered contributory to deaths from natural disease. These 19 cases were not included in further analysis. Drug poisoning cases in this study almost always involved combined drug toxicity; only one case involved oxycodone alone (range 1 to 14). A description of the combinations of drugs detected in toxicology of unintentional cases will be the subject of a future paper.
Cause of death involving oxycodone, Victoria 2003–09
Table 2 presents a summary of demographic characteristics of the 172 fatal drug toxicity cases. Fifty-eight per cent of cases were male, and males were overrepresented in the unintentional drug toxicity category (60%). Females accounted for 47% of the intentional cases, but differences in sex between unintentional and intentional cases were not statistically significant (p=0.48). Mean age of unintentional cases was 39.2 years, 7.8 years less than intentional self-harm cases whose mean age was 47 years (CI 3.1 to 12.6 years, p<0.001).
Demographic characteristics of fatal drug toxicity cases involving oxycodone, Victoria 2003–09
A higher proportion of cases in the unintentional drug toxicity category were either unemployed or receiving other government benefits (53.3%, p=0.13) than in the intentional drug toxicity category (38.3%), and a lower proportion of the unintentional drug toxicity category (5.6%) were retired than in the intentional drug toxicity category (17.7%). Most decedents (90.3%) died in their homes (91.1% of unintentional cases and 85.3% of intentional cases).
Table 3 shows the socioeconomic status indicators and rural/metropolitan location of residence of the deceased. Results show that drug toxicity deaths do not occur uniformly across the five quintiles of socioeconomic disadvantage (p=0.007). A majority (55.2%) of unintentional drug toxicity deaths occurred in quintiles 1 and 2, the most disadvantaged areas, while only 39.5% of the Victorian population live in these areas. Similarly, while 27.1% of the Victorian population live in rural areas, a disproportionately high percentage of unintentional drug toxicity deaths (41.4%) occurred in these areas (p<0.001).
Socioeconomic status and rural/metropolitan distribution of drug toxicity deaths involving oxycodone, 2003–09, Victoria
There were insufficient data available to meaningfully describe marital status; information was not known or not recorded for 111 cases. In 26 cases intent could not be ascertained and in a further 22 cases the coroner was still enquiring.
Discussion
The results of this study show a substantial increase in the number of deaths involving oxycodone reported to the Victorian Coroner that is strongly and significantly associated with increase in supply. This indicates that Victoria may be developing problems similar to those established in the USA and Canada,13 25 31 and reinforces the emerging global concern about the misuse of prescription drugs.32 Other factors contributing to the upward trend in deaths involving oxycodone in this study may include increased prescribing and availability of this drug, increased illicit access, increased media reporting,33 increased promotion and marketing,34 and the widespread availability of high dose controlled release single tablet formulations (OxyContin) where the controlled release mechanism can be easily compromised.35 However, this study was unable to ascertain how these factors may have contributed to the increase in deaths in Victoria.
Increases in the illicit use of prescription opioids in high income countries such as the USA, Canada, and Australia have been described as a paradigm shift from heroin to prescription opioids as the preferred street opioid for misuse.36 Women and older people are more likely to experience chronic pain,1 and are more likely to use opioids,37 suggesting that the higher proportion of men, and higher proportion of decedents in the 25–54 age group may reflect drug misuse among the population studied here. This study describes higher death rates of unintentional drug toxicity in the most disadvantaged quintiles, similar to findings from a study of unintentional pharmaceutical overdose deaths in the United States,13 and research from Washington that found Medicaid enrolees were six times more likely to die of prescription opioid poisoning than the non-Medicaid population (age adjusted RR of 5.7).26 The high death rate for unintentional drug toxicity in rural locations is also consistent with findings from the USA which report high death rates in predominantly rural states and regions.13 25 27 It is possible that use in rural areas is linked to lower availability of illicit drugs such as heroin,28 however further research is required to properly understand this imbalance in Victoria.
In Victoria, cases are reported to the coroner where a doctor is unable or unwilling to sign a death certificate or where death was unexpected, such as injury deaths. It is possible that not all cases of drug toxicity are referred to coroners. However, this potential bias is likely to remain similar throughout the years of our study.
All but one case of drug toxicity involved more than one drug, and the combinations of these drugs in unintentional cases will be described in a future paper. Opioids such as oxycodone are powerful central nervous system (CNS) depressants with a high risk of lethal toxicity if recommended doses are exceeded, and the presence of other CNS depressants, such as benzodiazepines and/or alcohol, potentiates this effect.38 There are inherent limitations in any postmortem study involving drug use. Interpretation of postmortem toxicology depends on individual variability in tolerance to the sedating effects of opioids, the site of the sampling, postmortem redistribution, and the interval between death and sample collection.39
Determining a cause of death, particularly in cases of drug toxicity, is sometimes difficult.30 The 19 cases where drugs were considered to have been contributory to deaths attributed to natural disease were not included in further analysis, meaning that our results may underestimate this problem of drug deaths involving oxycodone. Determination of intent in cases where the coroner is still enquiring will affect the proportions of intentional and unintentional deaths presented here.
Conclusions
The number of deaths reported to the Victorian Coroner where oxycodone is detected has increased substantially since 2000. The association between increasing deaths and the escalation of supply of oxycodone in Victoria highlights the need to better describe this phenomenon and identify opportunities for prevention across Australia and internationally.
The death investigation process could be developed to provide more detailed information that may assist in the development of preventive countermeasures, such as routinely recording the type and formulation of drugs consumed and/or found at the scene of the incident. There are opportunities for data linkage with Medicare Australia, the Australian universal medical insurance scheme. This may include prescriptions dispensed under the Medicare Australia Pharmaceutical Benefits Scheme (PBS), benefits processed under the Medical Benefits Scheme as well as the PBS Prescription Shopping programme database that may assist in determining whether prescriptions were supplied licitly to the deceased and whether problematic use had been identified, as other studies have done.13 23 24 26 These measures would enhance our understanding of the source of prescription drugs and the deceased's contact with healthcare providers prior to death. Licit drugs obtained illicitly may require a different preventive response to cases where escalating use or dependence has resulted from a genuine medical need.
This study highlights the need for a strategic response, including a system to enable coordinated management of opioid prescribing and dispensing in Australia. Regulatory authorities in Australia could contribute to preventing deaths by identifying people at risk because of misuse, or identifying drug-seeking individuals and preventing diversion.23 24 The USA has now introduced prescription drug monitoring programmes across most states,40 British Columbia has introduced the PharmaNet monitoring system,41 and legislation is under consideration in Ontario to improve the safety of prescriptions for narcotics, including oxycodone.42 These monitoring systems have the potential to provide prescribers with critical real time information about a patient's medication supply history. Health professionals need to be aware of the risk of drug toxicity and death. There was evidence of non-medical use in a large number of cases which resulted in unintentional overdose, and this will be the subject of a future paper.
What is already known on the subject
Global consumption of prescription opioids has increased substantially in the last decade. The increase in consumption in several high-income countries is associated with increased misuse, medical emergencies, and drug toxicity deaths.
In the United States and Canada, misuse of prescription opioids has been authoritatively described as a public health crisis.
There has been a substantial increase in supply of prescription opioids in Australia, and misuse is prevalent among people who inject drugs, but there is limited evidence about the nature and extent of misuse and resultant harm in the general population.
What this study adds
This study reports a strong and significant association between oxycodone supply and coronial deaths involving oxycodone in the state of Victoria, Australia.
Most deaths involving oxycodone were the result of drug toxicity, and most of these deaths were unintentional. Decedents from rural and disadvantaged areas were overrepresented.
There is an urgent need in Australia to develop a comprehensive strategic response, and improve monitoring of prescription opioids such as oxycodone in order to prevent increasing prescription opioid-related deaths.
This study adds to the mounting concern that increasing oxycodone related deaths may be a global trend.
Acknowledgments
Dr Rory Wolfe and Pamela Simpson at the Department of Epidemiology & Preventative Medicine, Monash University, provided statistical advice and supervision. Dr Dimitri Gerostromoulos & Prof Stephen Cordner, VIFM, respectively, provided forensic toxicology and pathology advice during the panel review. The Planning & Analysis Unit at the Victorian Department of Health geocoded deceased addresses. The authors are grateful to the reviewers of this paper who provided valuable comments.
References
Footnotes
Funding This work was completed during ACR's participation in the Victorian Public Health Training Scheme, funded by the State of Victoria through the Department of Health. The views and conclusions are those of the authors and do not necessarily represent those of the Department of Health.
Competing interests None.
Ethics approval This study was conducted with the approval of the human research ethics committees of the Victorian Department of Justice, Victorian Institute of Forensic Medicine, and Monash University.
Provenance and peer review Not commissioned; externally peer reviewed.