
Abstract
Consistent with its highest abundance in humans, cytochrome P450 (CYP) 3A is responsible for the metabolism of about 60% of currently known drugs. However, this unusual low substrate specificity also makes CYP3A4 susceptible to reversible or irreversible inhibition by a variety of drugs. Mechanism-based inhibition of CYP3A4 is characterised by nicotinamide adenine dinucleotide phosphate hydrogen (NADPH)-, time- and concentration-dependent enzyme inactivation, occurring when some drugs are converted by CYP isoenzymes to reactive metabolites capable of irreversibly binding covalently to CYP3A4. Approaches using in vitro, in silico and in vivo models can be used to study CYP3A4 inactivation by drugs. Human liver microsomes are always used to estimate inactivation kinetic parameters including the concentration required for half-maximal inactivation (K I) and the maximal rate of inactivation at saturation (k inact).
Clinically important mechanism-based CYP3A4 inhibitors include antibacterials (e.g. clarithromycin, erythromycin and isoniazid), anticancer agents (e.g. tamoxifen and irinotecan), anti-HIV agents (e.g. ritonavir and delavirdine), anti-hypertensives (e.g. dihydralazine, verapamil and diltiazem), sex steroids and their receptor modulators (e.g. gestodene and raloxifene), and several herbal constituents (e.g. bergamottin and glabridin). Drugs inactivating CYP3A4 often possess several common moieties such as a tertiary amine function, furan ring, and acetylene function. It appears that the chemical properties of a drug critical to CYP3A4 inactivation include formation of reactive metabolites by CYP isoenzymes, preponderance of CYP inducers and P-glycoprotein (P-gp) substrate, and occurrence of clinically significant pharmacokinetic interactions with coadministered drugs.
Compared with reversible inhibition of CYP3A4, mechanism-based inhibition of CYP3A4 more frequently cause pharmacokinetic-pharmacodynamic drug-drug interactions, as the inactivated CYP3A4 has to be replaced by newly synthesised CYP3A4 protein. The resultant drug interactions may lead to adverse drug effects, including some fatal events. For example, when aforementioned CYP3A4 inhibitors are coadministered with terfenadine, cisapride or astemizole (all CYP3A4 substrates), torsades de pointes (a life-threatening ventricular arrhythmia associated with QT prolongation) may occur.
However, predicting drug-drug interactions involving CYP3A4 inactivation is difficult, since the clinical outcomes depend on a number of factors that are associated with drugs and patients. The apparent pharmacokinetic effect of a mechanism-based inhibitor of CYP3A4 would be a function of its K I, k inact and partition ratio and the zero-order synthesis rate of new or replacement enzyme. The inactivators for CYP3A4 can be inducers and P-gp substrates/inhibitors, confounding in vitro-in vivo extrapolation. The clinical significance of CYP3A inhibition for drug safety and efficacy warrants closer understanding of the mechanisms for each inhibitor. Furthermore, such inactivation may be exploited for therapeutic gain in certain circumstances.
Similar content being viewed by others


The cytochrome P450 (CYP) [EC 1.14.14.1] superfamily, containing 57 genes,[1] contributes to the metabolism of a variety of xenobiotics including therapeutic drugs, carcinogens, steroids and eicosanoids.[2–6] The catalytic mechanism appears to be common to all CYP isoenzymes and involves a two-electron reduction of molecular oxygen to form a reactive oxygen species and water.[2,7] Among CYP isoenzymes, the subfamily CYP3A is responsible for the metabolism of about 60% of currently known therapeutic drugs.[2–4,8,9] The CYP3A subfamily in humans includes CYP3A4, CYP3A5, CYP3A7[4] and CYP3A43.[10] CYP3A4 is the most abundant among the isoenzymes of CYP3A subfamily in the human liver (~40%) and metabolises more than 50% of clinically used drugs,[3,11] whereas polymorphic CYP3A5 accounts for 5–50% of total CYP3A abundance[12,13] and is present in appreciable amounts in about 25% of the adult population.[14] CYP3A7 is the primary fetal isoform and is rarely detected in adults.[15,16] CYP3A43 gene is expressed significantly in the prostate and testis, whereas the hepatic messenger RNA (mRNA) level is only 0.2–5% of that of CYP3A4.[10] Thus, the two latter enzymes play a minor role in drug metabolism in adults.
The low substrate specificity makes CYP3A4 susceptible to reversible or irreversible inhibition by a variety of drugs.[17] The irreversible mechanism-based inhibition of CYP3A4 refers to the inactivation of the enzyme via the formation of metabolic intermediates (MIs) that bind tightly and irreversibly to the enzyme.[18,19] A mechanism-based inhibition of CYP3A4 should have the following features:[20,21]
-
preincubation time-dependent inhibition of CYP3A4
-
nicotinamide adenine dinucleotide phosphate hydrogen (NADPH)-dependent inhibition (i.e. no inhibition without NADPH in preincubation)
-
inhibitor concentration-dependent inhibition with saturation kinetics (pseudo first-order kinetics)
-
substrate protection (i.e. slower inactivation rate of the enzyme in the presence of substrate)
-
inhibitor protection (i.e. reduced inactivation of CYP3A4 when coincubated with CYP3A4 inhibitor or inhibitory antibody)
-
uncertain prevention by exogenous nucleophiles (e.g. glutathione semicarbazide, and N-acetylcysteine)
-
irreversible inhibition (i.e. CYP3A4 activity not recovered after gel filtration or dialysis)
-
stoichiometry of inactivation (i.e. 1: 1 stoichiometry of the inhibitor and the active site of CYP3A4).
1. Approaches to Investigating Mechanism-Based Inhibition of Cytochrome P450 (CYP) 3A4
1.1 In Vitro Models
Human liver microsomes, hepatocytes and complementary DNA (cDNA)-expressed enzymes are the commonly used in vitro systems for the investigation of mechanism-based inhibition of CYP3A4.[21] By using these in vitro models, the qualitative features of mechanism-based inhibition of CYP3A4, such as time-, NADPH- and concentration-dependent inhibition, can be easily determined. Experimentally, mechanisms of inhibition of inhibitors could be assessed initially by comparing their inhibitory effects obtained in the presence and absence of NADPH during a preincubation period. Important kinetic parameters for mechanism-based inhibition such as the concentration required for half-maximal inactivation (K I), the rate constant of maximal inactivation at saturation, analogous to maximum rate of metabolism by an enzyme-mediated reaction (k inact), and partition ratio (Rmax, ratio of moles of substrate activation per mole of enzyme inactivation) can also be determined.[21]
In vitro systems (particularly microsomal systems) can be used to isolate and identify the resultant covalent metabolic intermediate-CYP3A4 complex by using gel electrophoretic and mass spectrometric techniques. The addition of glutathione and N-acetylcysteine facilitates the identification of reactive metabolites and characterisation of adduct formation with CYP3A4.[22] An apparent attenuation of the degree of CYP3A4 inactivation in preincubation mixtures fortified with glutathione and the identification of glutathione adducts in human liver microsomal incubations would provide further evidence implicating reactive metabolites in the inactivation of CYP3A4. Each in vitro model has its advantages and disadvantages, and a combination use will often provide convincing data. Liver microsomes can be studied long term and are easily manipulated and optimised, but cofactor (NADPH) is necessary for CYP3A4-catalysed reactions to replace those lost as a result of the destruction of cell integrity. Hepatocytes provide cellular integrity with respect to enzyme architecture and are useful for determining the cytotoxicity of formed CYP3A4 adducts in vitro. However, the enzyme activity results obtained from hepatocytes should also be interpreted with caution, especially for quantitative comparisons, as many enzyme activities decline spontaneously during hepatocyte isolation or culture.[23] Cloned cDNA-expressed human CYP3A4 is available, and in theory supplies are unlimited.[24,25] It is worth noting that levels of enzyme expression are variable across expression systems, and (especially with regard to CYP3A) reductase and cytochrome b5 to CYP ratios are often nonphysiological.[24,26]
A number of well characterised model substrates for CYP3A4[27–29] can be used for the study of mechanism-based inhibition of CYP3A4 in vitro (table I). Among these CYP3A4 substrates, benzodiazepine (midazolam and triazolam), testosterone and ciclosporin are most commonly used. These probe drugs have been used to investigate the mechanism-based inhibition of CYP3A4 in vitro by a variety of drugs. These compounds are readily available and suitable for experiments in microsomes. However, only some of them may be used in assays with intact cells (e.g. hepatocytes), as these substrates should be noncytotoxic and readily move across cell membranes. Because the in vitro findings obtained with one probe substrate for CYP3A4 are often extrapolated to the potential of test compounds to influence all CYP3A substrates and the inhibition of CYP3A4 by drugs is often substrate-dependent,[30] it is important to use the right probe substrate and to conduct the experiment under optimal conditions.[28]

Some model substrates of cytochrome P450 (CYP) 3A4 used for the study of mechanism-based inhibition of CYP3A4
Selective inhibitors (chemicals[124] and inhibitory antibody[125] ) for CYP3A4 are also useful tools for the study of mechanism-based inhibition of CYP3A4. These chemical probes and antibody are validated and readily commercially available (see http://www.gentest.com;http://www.biotrend.com). Reversible CYP3A4 inhibitors such as ketoconazole,[22,117,119,126,127] itraconazole,[128] quinidine at high concentration (≥50 µmol/L),[22] testosterone,[129] terfenadine,[130] astemizole,[130] ciclosporin[128] and inhibitory antibody against CYP3A4[22,119,128] are useful for the demonstration of reduced covalent binding by drugs to CYP3A4 and CYP3A4 adduct formation in vitro. Mechanism-based inhibitors for CYP3A4 such as troleandomycin,[90,131–133] clarithromycin[90,91] and erythromycin[121,133] can be particularly useful, as they are often insensitive to the concentration of the test compound and can be used as reference CYP3A4 inactivators. Some of them such as ritonavir[119,120] have been used for the investigation of mechanism-based inhibition of CYP3A4 by drugs.
Model inducers (e.g. rifampicin [rifampin],[27,134] phenobarbital[27,135] and dexamethasone[27,134] ) of CYP3A4 can be used as a valuable tool in the study of mechanism-based CYP3A4 inhibition. The nuclear pregnane X receptor, also called steroid and xenobiotic receptor or pregnane-activated receptor, was found to mediate the drug-induced expression of CYP3A4.[136–140] In in vitro assays for CYP3A4 induction using hepatocytes,[141–146] the catalytic activity, protein or mRNA level of CYP3A4 are enhanced and thus the formation of CYP3A4 adducts can be increased, leading to increased CYP3A4 inactivation. It should be noted that this in vitro approach has several limitations, such as, the remarkable interindividual donor variation in response to the CYP3A4 inducers; and cell culture conditions are also an important factor contributing to the considerable variability of CYP3A4 induction.[146] In addition, the enzyme activity of CYP3A4 obtained from hepatocytes should also be interpreted with caution, especially for quantitative comparisons, as many enzyme activities decline spontaneously during hepatocyte isolation or culture.[23]
1.2 In Silico Models
There is increasing use of in silico methods to study mechanism-based inhibition of CYP isoenzymes by therapeutic drugs. The major in silico methods for this purpose include simple rule-based modelling, structure-activity relationships, three-dimensional quantitative structure-activity relationships, pharmacophores and homology modelling.[147–152] All of these represent useful tools for understanding inactivation reactions (formation of metabolic intermediate-CYP3A4 complex), structural requirements for inactivators, providing insight into the active site of CYP3A4, optimising the design of drugs and selective inhibitors of CYP3A4, and predicting possible metabolic drug-drug interactions involving mechanism-based inactivation of CYP3A4.[19,150,153,154] The resulting data based on in silico approaches may be of clinical significance. For example, knowledge of the substrate specificity and regulation of the CYP is essential, as this will provide information on the possible drug-drug interaction.
An example of application of an in silico model to understanding CYP3A4 inactivation is the structure-activity relationship analysis of the 17α-acetylenic steroids, which indicates that the delta 15 double bond is critical, but is not in itself sufficient for the inactivation process, possibly owing to attack of CYP on the substituted acetylenic carbon leading to porphyrin N-alkylation.[76] In fact, a variety of different mechanism-based CYP inactivators have proven to be useful in identifying active site amino acid residues involved in substrate binding and catalysis.[19] Labelled peptides isolated from the inactivated proteins can be analysed by N-terminal amino acid sequencing in conjunction with mass spectrometric techniques to determine the active sites of covalent modification and amino acids involved.[19]
1.3 In Vivo Models
Although in vitro and in silico models may provide a quick screening tool for mechanism-based CYP inhibition, the relative simplicity of in vitro and in silico approaches provide limited information without considering many important physiological factors. Animal models (mouse and rat) have been extensively used to study mechanism-based CYP3A inhibition, providing important information on CYP inactivation. However, interspecies variations in the substrate specificity, catalytic features and amino acid sequences of CYP isoenzymes may cause difficulty in extrapolating animal data to humans.[155–157] Therefore, in vivo human studies are usually necessary to provide evidence of their clinical importance.
Most substrates listed in table I can be used in vivo in humans to evaluate inhibition and induction of CYP3A.[25,158] Midazolam is considered as one of the best in vivo probe drugs for the study of CYP3A4 activity,[17] for several reasons: it can be administrated both orally and intravenously, which can provide a measure of CYP3A4 activity relative to intestinal and hepatic metabolism, respectively; midazolam is not a substrate of P-glycoprotein (P-gp);[159] and midazolam metabolism at lower concentrations exhibits a regioselective difference which can be used to discriminate among individuals with or without CYP3A5, as CYP3A5 has a much higher 1′-OH: 4-OH ratio of midazolam metabolism than CYP3A4.[12,87] Several classical inducers such as rifampicin,[160–162] ritonavir[77,163] and phenobarbital can be used to study induction of hepatic and intestinal expression of CYP3A4 in vivo in humans.
2. Biochemical Mechanism for Drug-Induced Inactivation of CYP3A4
2.1 Formation of Reactive Metabolic Intermediates of Drugs
The first step of inactivating CYP3A4 by drugs is the bioactivation of drugs to reactive MIs, which is often via various CYP isoenzymes. The diversity of CYP isoforms means that a wide range of drugs can be bioactivated by either a single CYP or multiple CYPs. It is well known that drugs which contain several common moieties such as a tertiary amine function,[164–167] furan ring[114,168] and acetylene function[76,113] are metabolised by CYP isoenzymes and bind to the same enzyme covalently to form a CYP-metabolite complex and thereby inactivate the enzyme. Investigations of mechanism-based inactivation can lead to detailed information on the interaction of the compound and the enzyme, i.e. the nature of the reactive intermediate formed, the efficiency of the inactivation process, and amino acid residues located within the enzyme active site.[19]
For some CYP3A4 inactivators, the reactive MIs have been largely identified. Diltiazem, nicardipine and verapamil (all calcium channel antagonists) contain an amine functional group and undergo N-dealkylation, resulting in MIs.[169,170] Macrolides such as erythromycin, clarithromycin, troleandomycin and oleandomycin with 14-membered rings can be metabolised by CYP3A4 to form reactive nitrosoalkanes via N-demethylation which interact with CYP to result in MI complex.[90,131,132,164,171–176] Ethinylestradiol, the major constituent of many oral contraceptives, is metabolised by CYP3A4 to one major metabolite, 2-hydroxyethinylestradiol, and at least three additional catechol metabolites,[129,177] which are believed to inactivate CYP3A4.[129] However, for most known CYP3A4 inactivators, their reactive MIs and bioactivation pathways are largely unknown. The CYP3A4-mediated metabolism of several protease inhibitors (amprenavir,[120] L 754394,[147,178,179] nelfinavir[180] and ritonavir[119,120] ) results in unknown reactive metabolites which then inactivate CYP3A4. Midazolam is a potent CYP3A4 inactivator and such enzyme inactivation is suggested to be related to the 1′-hydroxylation metabolic pathway.[181] Several antiprogestogens (e.g. mifepristone, lilopristone and onapristone) are suggested to be oxidised by CYP3A4 to reactive nitroso species that complex the haem of the enzyme,[182] thereby inactivating it.
2.2 Multiple Active Sites of CYP3A4
CYP3A4 is known to metabolise a large variety of compounds varying in molecular weight (MW) from lidocaine (MW = 234d) to ciclosporin (MW = 1203d).[2,183] It is believed that CYP3A4 has a spacious hydrophobic active site capable of accommodating a diverse range of compounds. As a result, CYP3A4 binding interactions are dominated by the lipophilicity of the drug molecule involved, as indicated by a significant correlation between the octanol partition coefficient (log D7.4) and apparent Michaelis-Menten constant (K m) for CYP3A4.[184,185] Modelling and amino acid alignment studies have proposed that these amino acids occupy positions in the F-helix, remote from the haem iron of the CYP3A4 active site.[186] Mutagenesis studies have demonstrated that replacement of leucine 210 or leucine 211 with alanine reduced, but did not abolish, the activation effect of α-naphthoflavone on progesterone and testosterone hydroxylase activities.[187]
In deference to the large CYP3A4 active site, substrate-dependent drug-drug interactions and the atypical pharmacokinetics associated with certain CYP3A4-mediated oxidations, there is strong evidence in support of the hypothesis that there are multiple substrate binding sites in CYP3A4.[188–191] The evidence is mainly from studies using methods such as site-directed mutagenesis, homology modelling and functional analysis using substrates such as progesterone, testosterone and midazolam.[30,181,192] The most distant amino acids from the catalytic centre of CYP3A4 that have a role in substrate binding are leucine 210, leucine 211 and aspartic acid 214.[187,193]
CYP3A4 exhibits unusual substrate kinetics, including activation, autoactivation, partial inhibition and substrate inhibition often observed.[30,188–190,194] Several hypotheses involving two-site or three-site models as well as the existence of functionally distinct conformers have been proposed to explain the atypical CYP3A4 pharmacokinetics.[188–190] There is a 6-fold difference in the K m values between triazolam α-hydroxylation and 4-hydroxylation[195] and two very distinct K m values for the two hydroxylation pathways of midazolam,[181,196,197] suggesting the existence of two binding sites in CYP3A4. The differential stimulation/inhibition by α-naphthoflavone and testosterone[30,196] and observation of two distinct apparent inhibition constant (K i) values for inhibition of 1′-OH and 4-OH midazolam formation by the peptide YPFP-NH2 have provided additional evidence to support two binding sites of CYP3A4.[197] However, the possibility of the substrate binding at a single site but in two different orientations cannot be ruled out. Furthermore, molecular modelling[193] and mechanistic studies[190,197] suggest that the complex effects observed with select CYP3A4 substrates may be attributable to the binding of multiple substrates within the active site of the enzyme.
2.3 Mechanisms for the Inactivation of CYP3A4
Mechanisms of CYP inhibition by a drug can be divided into three categories: reversible, quasi-irreversible and irreversible.[198] Quasi-irreversible and irreversible inhibitors require at least one cycle of the CYP catalytic process and are thus signified by both NADPH- and time-dependent inhibition. These catalytic processes result in reactive metabolites that lead to chemical modification of the haem, the protein, or both as a result of covalent binding of modified haem to the protein.[21,199,200] The detailed mechanism of inactivation may be elucidated by a number of analytical and proteomic techniques, such as mass spectrometry and homology modelling. For example, mifepristone was shown to be covalently bound to the apoCYP3A4 by gel electrophoresis,[113,114] while both haem adduction and fragmentation are ruled out, as the Soret absorption of the inactivated CYP3A4 did not decrease when compared with the controls.[201] A similar result has been observed with bergamottin.[114,202,203]
Covalent labelling of the apoCYP isoforms has been shown to be the mechanism for inactivation of CYPs by terminal acetylenes such as 1-ethinylpyrene, 2-ethinylnaphthalene, and some other polycyclic arylacetylenes,[204–206] furan-containing compounds such as methoxsalen, coriandrin and bergamottin,[114,202,207] and sulphur-containing and halogenated compounds such as parathion and chloramphenicol.[208,209] CYP3A4 inactivators such as delavirdine,[126] L 754394,[147] ethinylestradiol[129] and midazolam[181,190] possibly bind covalently to the CYP apoprotein and inactivate it. Certain CYP3A4 inactivators such as macrolides (e.g. erythromycin[210] ), glabridin[211] and nelfinavir[180] bind the haem and inactivate the enzyme.
The reactive intermediates of acetylenic compounds formed by several CYP isoenzymes have been known to alkylate the prosthetic haem group as well as to bind covalently to the protein.[200] Studies with CYP2B1 demonstrated that 2-ethinylnaphthalene predominantly inactivates CYP2B1 through modification of the apoprotein, whereas phenylacetylene inactivates CYP2B1 via N-alkylation of haem.[205,212] In the case of ethinylestradiol, the enzyme inactivation led to the destruction of approximately half the haem with the concomitant generation of modified haem and ethinylestradiol-labelled haem fragments and produced covalently radiolabelled CYP3A4 apoprotein.[114,129,199,213–215] The chemical structure(s) and the nature of adduction of these modified species remain to be established. Ethinylestradiol can modify both the haem and the apoprotein of CYP3A4, whereas it modified only the apoprotein in CYP2B1 and CYP2B6.[216] These results suggest that the metabolic activation of a single ethinyl compound can result in different reactivities towards haem versus apoprotein with different CYP isoenzymes.
3. Estimation of Inhibitory Potencies of CYP3A4 Inactivators
3.1 Estimation of Apparent KI and kinact
To get K I and k inact, the logarithm of the remaining enzymatic activity is plotted against the preincubation time. The apparent inactivation rate constant (k obs) is determined from the slope of the initial linear phase. The value of k obs is then plotted against the inhibitor concentration, and the parameters (k inact and K I) are obtained by the nonlinear least-squares method using the following equation (equation 1):[21,217]
where k obs, k inact, K I represent the apparent inactivation rate constant of the enzyme at the initial concentration of inhibitor [I], the maximum inactivation rate constant, and the apparent inactivation constant between the enzyme and inhibitor, respectively. Furthermore, the inactivation efficiency (Einact) can be calculated by equation 2:
The inactivation half-life (t ½ inact) can be calculated by equation 3:
In addition, R max can be estimated by equation 4:
where r and R max represent the nanomoles of reactive product formed per nanomole CYP at a particular time (t) and at infinity, respectively. It should be noted that partition ratio (R max) is also an important potency parameter for CYP3A4 inactivation. The partition ratio of the most powerful mechanism-based inhibitor is zero (i.e. every turnover produces inactivated enzyme). CYP3A4 inactivators with a low partition ratio (e.g. 1.4 for L 754394[147,178] ) are often potent mechanism-based inhibitors, while those with a high partition ratio (e.g. 50 for ethinylestradiol[129] and 41 for delavirdine[126] ) have low inhibition of CYP3A4.
3.2 Reported Apparent KI and kinact
A number of drugs with different efficacy and structure have been reported to be mechanism-based inhibitors of CYP3A4 (table II). Most of these drugs are reported to be CYP substrates and reversible inhibitors of CYP3A4. These drugs can be classified into four groups based on their K I values, reflecting their inhibitory potency: drugs with K I ≤1.0 µmol/L (e.g. ritonavir,[119,120] troleandomycin[90,131–133] and tamoxifen[110] ); drugs with K I 1.1–5.0 µmol/L (e.g. amprenavir,[120] verapamil,[95,218] diltiazem[91,92,95,218] and mibefradil[219] ); drugs with K I 5.1–10.0 µmol/L (e.g. fluoxetine,[91] midazolam[181] and clarithromycin[90,91] ); and drugs with K I >10 µmol/L (e.g. irinotecan,[109] gestodene,[76] isoniazid[89] and erythromycin[220–222] ). In addition, the metabolites of some drugs are also mechanism-based inhibitors of CYP3A4 (e.g. N-desmethyl diltiazem,[91] N-desmethyltamoxifen,[110] SN 38[109] and 6′, 7′-dihydroxybergamottin[223] ). Among these drugs, both K 11777[128] and ritonavir[119,120] are the most potent CYP3A4 inactivators, with K I of 0.06 and 0.07 µmol/L, respectively; whereas isoniazid[89] is a weak CYP3A4 inactivator with a K I of 228 µmol/L.

Drugs reported to be mechanism-based cytochrome P450 (CYP) 3A4 inhibitors and their corresponding apparent K m, K i and K I values
Drugs in table II can also be classified in four groups based on their k inact values: drugs with k inact ≤0.06 min– 1 (i.e. t ½ inact ≥11.6 min) [e.g. fluoxetine,[91] dihydralazine,[111] tamoxifen[110] and irinotecan[109] ]; drugs with k inact 0.061–0.10 min– 1 (i.e. t ½ inact 6.93–11.5 min) [e.g. clarithromycin,[90,91] amprenavir[120] and ritonavir[119,120] ]; drugs with k inact 0.11–0.29 min– 1 (i.e. t ½ inact 2.39–6.30 min) [e.g. diltiazem,[91,92,95,218] glabridin,[211] troleandomycin[90,131–133] and raloxifene[22] ]; and drugs with k inact ≥0.30 min– 1 (i.e. t ½ inact ≥6.30 min) [e.g. gestodene,[76] mibefradil[219] and delavirdine[126] ]. Both nicardipine[95] and L 754394[147,178] are the most potent inactivators of CYP3A4, with a k inact of 2.0 and 1.62 min– 1, respectively, while fluoxetine[91] and K 11002[128] inhibited CYP3A4 to the least extent, with k inact values of 0.017–0.026 min– 1.
3.3 Relationship between KI and kinact, Km and Ki
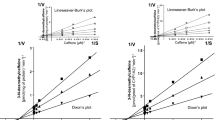
There is no significant relationship between K I and k inact (r 2 = –0.31, p = 0.598) [figure 1 a], indicating that both inhibitor concentration and time of exposure are independent determinants for CYP3A4 inactivation. Similarly, there is no correlation between apparent K i and K I (r 2 = 0.047, p = 0.3454) [figure 1 b]. This may be because the apparent K i is mainly determined by a reversible process where the parent drug molecules play a major role; whereas K I is a dissociation constant reflecting an irreversible process where covalent binding occurs.[19] In particular, the K i values for CYP3A4 inhibition may be substrate-dependent and less selective compared with K I. As shown in table II, the apparent K i values of drugs for the inhibition of CYP3A4-mediated reaction are often greater than the corresponding K I values, exceptions being gestodene (5.6[47] vs 46 µmol/L[76] ) and isoniazid (63.9[231] vs 228 µmol/L[89] ).

Relationship between K I and k inact (a), K i (b) and K m (c). K I = concentration required for half-maximal inactivation; K i = apparent inhibition constant; k inact = maximal rate of inactivation at saturation; K m = Michaelis-Menten constant.
Because of the highly possible relevance of drug bioactivation by CYP isoenzymes to metabolites that subsequently inactivate the enzymes, the apparent K m values for bioactivation are often comparable to the K I values. For example, the apparent K m value[234] for the hydroxylation of the 17α-propynyl group of mifepristone (9.9 µmol/L) in human liver microsomes is comparable to its K I (4.7 µmol/L).[113] Another example is delavirdine, which undergoes oxidation (desalkylation and 6′-hydroxylation) by pooled human liver microsomes or recombinant CYP3A4 with an apparent K m of 5.4–6.8 µmol/L,[126] which is close to its K I (9.5 ± 1.7 µmol/L) for CYP3A4 inactivation.[117] The similar binding affinities for these two independent processes imply that the orientation of the mifepristone molecule in the active site of CYP3A4 may be similar for both the oxidative bioactivation and enzyme inactivation. A relationship study of CYP3A4 inactivators indicates that there is a significant relationship between apparent K m and K I (r 2 = 0.668, p = 0.004) [figure 1 c]. However, this positive correlation disappears if amprenavir,[120] clarithromycin,[90,91] diltiazem[228] and tamoxifen[110] are included. For these drugs, a large difference (9.8- to 250-fold) between apparent K m and K I are observed, which may be due to the involvement of multiple CYP isoenzymes in their metabolism and bioactivation, multiple binding sites of CYP3A4, nonspecific binding to microsomal proteins and different assay systems.
4. Clinical Considerations of Drug-Induced CYP3A4 Inactivation
4.1 Altered Drug Pharmacokinetics and/or Pharmacodynamics due to CYP3A4 Inactivation
Because of the pivotal role of CYP isoenzymes in drug metabolism, significant inactivation of these isoforms and particularly the major human hepatic and intestinal CYP3A4 could result in drug-drug interactions and adverse drug reactions. Compared with reversible inhibition of CYP3A4, mechanism-based inhibitors of CYP3A4 more frequently cause pharmacokinetic/pharmacodynamic drug-drug interactions, as the inactivated CYP3A4 has to be replaced by newly synthesised CYP3A4 protein. Pharmacokinetic interactions often occur as a result of a change in drug metabolism. For example, the 14-membered-ring macrolides increased the plasma concentrations of a number of therapeutic agents that are substrates of CYP3A4 (table III). Diltiazem has been shown to potently inhibit the metabolism of a variety of coadministered drugs including carbamazepine,[240] ciclosporin,[241,242] quinidine,[243] midazolam,[244] alfentanil,[36] nifedipine[245] and lovastatin[246] (table IV). Inhibition of CYP3A by ritonavir explains, at least in part, the remarkable elevation of blood concentrations and area under the plasma concentration-time curve (AUC) of other concomitantly administered drugs that are extensively metabolised by CYP3A4 and have intermediate (10–80 L/h) to high (>80 L/h) intrinsic clearance and significant first-pass metabolism. These drugs include rifabutin (400%),[247] clarithromycin (77%),[248] ketoconazole (350%),[163] saquinavir (5000%),[249] amprenavir (210%),[250,251] nelfinavir (152%),[163,252] lopinavir (7700%)[253] and indinavir (380%).[254]

Examples of macrolide-drug interactions potentially involving mechanism-based cytochrome P450 3A4 inhibition

Examples of diltiazem-drug interactions potentially involving mechanism-based cytochrome P450 3A4 inhibition
Mechanism-based inactivation of CYP3A4 may cause severe drug toxicity due to metabolic inhibition of coadministered drugs.[269] When irreversible CYP3A4 inhibitors such as erythromycin and clarithromycin are coadministered with other drugs such as terfenadine, astemizole or pimozide, patients may experience torsades de pointes.[269–271] Terfenadine is a CYP3A4 substrate that undergoes extensive first-pass metabolism following oral administration.[54,272] In the absence of a drug interaction, the carboxylate metabolite is the principal circulating entity in plasma, whereas unchanged terfenadine, a drug known to cause torsades de pointes, is normally not present at measurable concentrations.[272,273] Rhabdomyolysis has occurred when simvastatin was combined with erythromycin or ritonavir.[274] Symptomatic hypotension may occur when mechanism-based CYP3A4 inhibitors are combined with some dihydropyridine calcium channel antagonists,[275] as well as with the phosphodiesterase inhibitor sildenafil.[276] In addition, ataxia can occur when carbamazepine is coadministered with mechanism-based CYP3A4 inhibitors such as macrolide antibacterials, isoniazid, verapamil and diltiazem.[277,278] On the other hand, beneficial drug interactions may occur as a result of CYP3A4 inactivation. Coadministration of a mechanism-based CYP3A4 inhibitor with ciclosporin may allow reduction of the dosage and cost of the immunosuppressant.[269] Certain HIV protease inhibitors (e.g. saquinavir) have low oral bioavailability that can be significantly (>50-fold) increased by the addition of ritonavir.[279,280]
In addition to toxic drug-drug interactions, the formation of drug reactive metabolite-CYP3A can also play a role in toxicity initiation. The formed adduct can induce potential immune responses, leading to production of autoantibodies against CYP3A. The formation of drug-CYP3A adducts may be nontoxic or fatal, depending on the drugs, pharmacokinetics of adduct formation and degradation, other affected target proteins and organs, and pathological conditions of the patients.[281] The reactivity of drug intermediates and subcellular localisation of major protein targets are important determining factors in the toxicity.[282,283] Selective protein covalent binding by a drug or its metabolite(s) has been associated with target organ/tissue toxicity of drugs.[284] For example, reactive metabolites of tamoxifen are believed to bind covalently to DNA and proteins in the endometrial tissue, causing endometrial carcinoma.
4.2 In Vitro-In Vivo Extrapolation Involving CYP3A4 Inactivation
One of the main objectives of in vitro metabolic inhibition studies is the qualitative and quantitative prediction of in vivo drug-drug interactions, and quantitative in vitro metabolic data may be extrapolated reasonably well to in vivo situations with the application of appropriate pharmacokinetic principles.[20,285–288] It can be anticipated that the inactivation of CYP3A4 by various drugs would increase the bioavailability of coadministered drugs metabolised mainly by CYP3A4, because of intestinal and hepatic inhibition of CYP3A4. It is believed that, in vivo, the inhibitory effect of a mechanistic inactivator is more prominent after multiple-dose administration and lasts longer than that of a reversible inhibitor.[198] The activated species irreversibly alters the enzyme to remove it permanently from the pool of active enzyme. Thus, the time-dependent inactivation of CYP3A isoenzymes results in nonlinear pharmacokinetics, as indicated by 50–100% prolongation of the diltiazem half-life in humans after long-term administration compared with the single-dose data.[289]
The extent of a drug interaction due to CYP3A inactivation is time dependent in both onset and offset. For example, erythromycin did not significantly inhibit the clearance of alfentanil on the first day of coadministration but produced a 25% decrease after 7 days.[37] As the half-life for onset of inactivation is inversely proportional to the efficiency [k inact/(K I + [I])] of inactivation, the delayed onset of inhibition by erythromycin is a predictable property of a relatively weak inactivator. The delayed offset of CYP3A inhibition is expected to be independent of the inactivating drug and the extent of inhibition. This time-dependent offset may explain the serious adverse events associated with discontinuation of the irreversible inactivator, mibefradil, and immediate initiation of alternative calcium channel antagonist treatment.[219,290] A mibefradil washout period of 7–14 days was thus recommended.
Determination of in vitro pharmacokinetic parameters is essential for the prediction of drug metabolism by a particular CYP isoenzyme in vivo. The apparent K I values for competitive inhibition determined in vitro, together with its relationship to unbound plasma concentrations of the inhibitor achieved with therapeutic doses in vivo, can be used as a rough guide to predict the possibility of a significant in vivo drug interaction.[20,291] Relating the in vitro results to in vivo pharmacokinetics is not straightforward. Generally, to predict the degree of interaction observed in clinical cases quantitatively, it is necessary to investigate the correlation between in vitro inhibitory potency of the inhibitor and in vivo inhibition, taking into account the distribution of the inhibitor into the liver, and extrapolation of data from animal studies.[229]
Several approaches for modelling mechanism-based enzyme inactivation have been described in the literature.[21,91,217,292–294] In a well described model of mechanism-based enzyme,[293] an inactivator can be released from the enzyme through reversible binding, converted to a product through a productive catalytic cycle, or can inactivate the enzyme by forming a complex. The active enzyme concentration at time t ([E]t) can be defined by equation 5:
where [E]0 is the initial enzyme concentration, [I] is inactivator concentration, and k inact and K I are parameters estimable by nonlinear regression. This model assumes that:[91]
-
the conditions of the well stirred model are met;
-
hepatic elimination is the only pathway;
-
there is complete absorption of drugs from the gastrointestinal tract;
-
hepatic first-pass metabolism is influenced by an inactivator.
By using this model, it was predicted that diltiazem, clarithromycin and fluoxetine at unbound plasma concentrations of 0.1 µmol/L will increase the AUC of a coadministered CYP3A substrate by 1.4-, 2.6- and 4.7-fold, respectively.[91] These predicted results are in good qualitative agreement with reported clinical data, especially when one considers that simple competitive models completely fail to predict any interactions where a K i of 60, 10 and 50 µmol/L for diltiazem, clarithromycin and fluoxetine, respectively,[54,220,295] and steady-state plasma concentrations of 0.3, 0.9 and 1.0 µmol/L, respectively, were used.[94,246,295]
However, the in vitro inhibitory potencies of mechanism-based CYP3A4 inhibitors do not necessarily translate directly into relative extents of inhibition in vivo. In vivo clinical consequences depend upon additional factors that are not easily accounted for in vitro and they could confound in vitro - in vivo extrapolation for drug-drug interactions. Such factors include:
-
concentration-time course
-
plasma protein binding
-
atypical substrate pharmacokinetics for CYP3A4
-
existence of inhibitory metabolites
-
partitioning from plasma to liver
-
rate-limiting transport of drug and inhibitor into the hepatocytes
-
intestinal active efflux of drug and inhibitor
-
extrahepatic metabolism of drugs and inhibitors.
4.3 Factors Affecting the Clinical Consequence of Mechanism-Based Inhibition of CYP3A4
4.3.1 Drug-Related Factors
The clinical importance of any drug-drug interaction due to CYP3A4 inactivation depends on factors that are associated with the administered drugs and patients, and the pharmacodynamic consequences may or may not closely follow pharmacokinetic alterations. Since many mechanism-based CYP3A4 inhibitors are also inducers of CYP isoenzymes, and enzyme inactivation is significantly affected by drug exposure time, the clearance of coadministered drugs may be increased or decreased in vivo, depending on the interplay between substrate, inhibitor, inducer and CYP3A4. There appear to be no common structural factors that determine whether a compound is a CYP3A4 inactivator. However, it is well known that drugs which have several common moieties such as a tertiary amine function,[164,165] furan ring[114,168] and acetylene function[76,113] are metabolised by CYP isoenzymes and bind to the same enzyme covalently to form a CYP-metabolite complex and thereby inactivate the enzyme. It appears that the chemical properties of a drug critical to CYP3A4 inactivation include formation of reactive metabolites, metabolism by CYP isoenzymes, preponderance of CYP inducers and P-gp substrate, and occurrence of clinically significant pharmacokinetic interactions with coadministered drugs.
Many CYP3A4 inactivators such as irinotecan,[296–299] some protease inhibitors[300] and mifepristone[301] are also known substrates and/or inhibitors of P-gp. P-gp encoded by the human MDR1 is constitutively expressed in the brush border membrane of intestinal enterocytes and the canalicular membrane of hepatocytes, and it transports structurally and functionally diverse compounds.[302,303] Thus, the potential for effects of these CYP3A4 inhibitors on the bioavailability of certain drugs may be enhanced, given that P-gp is the other major determinant of the oral bioavailability of many drugs.[301,304] However, P-gp can also alter the intracellular concentration of CYP3A inhibitors and inducers and hence the magnitude of the inhibitory and inductive response. Furthermore, P-gp is present on many barrier sites throughout the body, such as the blood-brain and blood-testis interfaces, and could decrease the concentration of its substrates such as protease inhibitors in these sanctuary sites.[302] P-gp, like CYP3A, can also be induced by many drugs.[305] This would complicate the interactions between drugs, CYP3A and P-gp. It has been postulated that P-gp and CYP3A are functionally linked components of a drug detoxification cascade that limits the bioavailability of several drugs.[306] There is substantial overlap in substrate specificity between CYP3A and P-gp, and several modulators/substrates of P-gp and CYP3A have been shown to coordinately upregulate the expression of these proteins in vitro.[307]
4.3.2 Patient-Related Factors
The age, sex, comedications, diseases and genetic factors are all potentially important factors affecting the clinical outcomes of mechanism-based inactivation of CYP3A4. In most cases, there are remarkable interindividual variations in the mechanism-based inactivation of CYP3A4 and subsequent drug-drug interactions. This is mainly due to the significant difference of CYP3A4 content. There is a significant variation in the hepatic expression of CYP3A4 based on in vitro (35- to 100-fold) studies using human liver bank[11] and in vivo (20- to 50-fold) using probe drugs such as erythromycin[308] midazolam[93] and alfentanil.[34] Such a substantial variation is considered to be the result of a number of environmental, physiological and genetic factors.[137] Treatment of patients with rifampicin results in a 4- to 8-fold variation in induction of CYP3A4 in the enterocyte as assessed by CYP3A4 probe,[309] indicating additional interindividual variation in the CYP3A4 inductive response.
It appears that there are no marked age and sex differences in CYP3A4 expression,[310–312] although 24–36% higher activity in females than in males has been reported.[70] CYP3A4 catalytic activity is also not affected by smoking status, alcohol (ethanol) consumption or percentage ideal bodyweight.[310] Thus, it can be predicted that age and sex are not important factors determining the clinical outcome of drug interactions involving CYP3A4 inactivation. However, changes in liver blood flow, liver size, renal function, drug protein binding and distribution with aging may be significant, and thus affect drug metabolism and elimination. Further studies are required to substantiate whether there is a clinically significant sex- and age-dependent difference in CYP3A inactivation.
Inflammation and relevant cytokines are known to affect drug metabolism by downregulating or upregulating expression of several CYP isoenzymes, including the CYP3A subfamily. Cytokines such as interleukin-6 rapidly and extensively decreased the expression of both human pregnane X receptor and constitutively activated receptor mRNAs in human hepatocytes, leading to reduced expression of CYP3A4, CYP2B and CYP2C.[309] This receptor downregulation phenomenon is accompanied by reduced responsiveness of CYP3A4 to induction by both rifampicin and phenobarbital. In addition, cytokines are potent regulating factors of drug transporters,[313] indicating a complex effect on drug metabolism and transport of inflammation and cytokines.
5. Conclusion and Future Perspectives
The low substrate specificity also makes CYP3A4 susceptible to reversible or irreversible inhibition by a variety of drugs. Irreversible inhibition of CYP3A4 due to enzyme inactivation or complexation occurs when some therapeutic drugs are converted by CYP isoenzymes to reactive metabolites capable of binding covalently to CYP3A4. Clinically important mechanism-based CYP3A4 inhibitors include antibacterials (e.g. clarithromycin, erythromycin and isoniazid), anticancer agents (e.g. irinotecan and tamoxifen), anti-HIV agents (e.g. ritonavir and delavirdine), antihypertensives (e.g. verapamil and diltiazem), and sex steroids and their modulators (e.g. gestodene and mifepristone). Most of these CYP3A4 inactivators are also substrates and inducers of CYP isoenzymes (particularly CYP3A4). The drugs that inactivate CYP3A4 often possess several common moieties such as a tertiary amine function, furan ring and acetylene function.
The functional effects of CYP3A4 inactivation on drug pharmacokinetics are indistinguishable, depending on factors that are associated with drugs and patients. The pharmacodynamic consequences (efficacy and toxicity) may or may not closely follow pharmacokinetic alterations due to CYP3A4 inactivation that causes long-term effects on drug pharmacokinetics, as the inactivated CYP3A4 has to be replaced by newly synthesised CYP3A4 protein. Severe drug toxicity has been observed as a result of the inactivation of CYP3A4 by coadministered drugs. For example, when aforementioned CYP3A4 inactivators are coadministered with terfenadine, cisapride or astemizole (all CYP3A4 substrates), torsades de pointes (a life-threatening ventricular arrhythmia associated with QT prolongation) may occur.
The study of mechanism-based CYP3A4 inhibition may play an important role in drug development.[314] During drug development, early discovery of problematic drugs that inactivate CYP3A4 can save time and money. Late recognition of significant drug interactions due to CYP3A4 modulation would put patients at risk of clinical toxicity. An example of early detection of potentially toxic drug-drug interactions involving CYP3A inactivation is mibefradil, which has been withdrawn from the market. Currently, it is impossible to accurately predict which new drugs will be associated with the formation of reactive metabolites and CYP3A inactivation, leading to potentially toxic drug-drug interactions. However, by screening drug candidates for the formation of reactive metabolites and CYP3A4 inhibition nature and establishing structure-activity relationships it is possible to halt the development of problematic drugs. The application of genomic and proteomic, coupled with in silico methods, approaches to the study of drug-CYP interactions has the potential to lead to a more effective screen because of their high throughput capacity.
References
Nelson D. Cytochrome P450 homepage [online]. Available from URL: http://drnelson.utmem.edu/CytochromeP450.html [Accessed 2005 Feb 3]
Rendic S. Summary of information on human CYP enzymes: human P450 metabolism data. Drug Metab Rev 2002; 34(1–2): 83–448
Rendic S, Di Carlo FJ. Human cytochrome P450 enzyme: a status report summarizing their reactions, substrates, induction, and inhibitors. Drug Metab Rev 1997; 29(1–2): 413–580
Nelson DR, Koymans L, Kamataki T, et al. P450 superfamily: update on new sequences, gene mapping, accession numbers and nomenclature. Pharmacogenetics 1996; 6(1): 1–42
Gonzalez FJ. Evolution of the P450 gene superfamily: animal-plant ‘warfare’, molecular drive and human genetic differences in drug oxidation. Trends Genet 1990; 6(6): 182–6
Nebert DW, Russell DW. Clinical importance of the cytochromes P450. Lancet 2002; 360(9340): 1155–62
Porter TD, Coon MJ. Cytochrome P450: multiplicity of isoforms, substrates, and catalytic and regulatory mechanisms. J Biol Chem 1991; 266: 13469–72
Wormhoudt LW, Commandeur JNM, Vermeulen NPE. Genetic polymorphisms of human N-acetyltransferase, cytochrome P450, glutathione-S-transferase, and epoxide hydrolase enzymes: relevance to xenobiotic metabolism and toxicity. Crit Rev Toxicol 1999; 29(1): 59–124
Rodrigues AD, Rushmore TH. Cytochrome P450 pharmacogenetics in drug development: in vitro studies and clinical consequences. Curr Drug Metab 2002; 3(3): 289–309
Domanski TL, Finta C, Halpert JR, et al. cDNA cloning and initial characterization of CYP3A43, a novel human cytochrome P450. Mol Pharmacol 2001; 59: 386–92
Shimada T, Yamazaki H, Mimura M, et al. Interindividual variations in human liver cytochrome P450 enzymes involved in the oxidation of drugs, carcinogens and toxic chemicals. J Pharmacol Exp Ther 1994; 270(1): 414–23
Kuehl P, Zhang J, Lin Y, et al. Sequence diversity in CYP3A promoters and characterization of the genetic basis of polymorphic CYP3A5 expression. Nat Genet 2001; 27(4): 383–91
Westlind-Johnsson A, Malmebo S, Johansson A, et al. Comparative analysis of CYP3A expression in human liver suggests only a minor role for cyp3a5 in drug metabolism. Drug Metab Dispos 2003; 31(6): 755–61
Wrighton SA, Brian WR, Sari MA, et al. Studies on the expression and metabolic capabilities of human liver cytochrome P450IIIA5 (HLp3). Mol Pharmacol 1990; 38(2): 207–13
Schuetz JD, Beach DL, Guzelian PS. Selective expression of cytochrome P450 CYP3A mRNAs in embryonic and adult human liver. Pharmacogenetics 1994; 4: 11–20
Komori M, Nishio K, Kitada M, et al. Fetus-specific expression of a form of cytochrome P-450 in human livers. Biochemistry 1990; 29(18): 4430–3
Thummel KE, Wilkinson GR. In vitro and in vivo drug interactions involving human CYP3A. Annu Rev Pharmacol Toxicol 1998; 38: 389–430
Silverman RB. Mechanism-based enzyme inactivation: chemistry and enzymology. Boca Raton (FL): CRC Press, 1988
Kent UM, Juschyshyn MI, Hollenberg PF. Mechanism-based inactivators as probes of cytochrome P450 structure and function. Curr Drug Metab 2001; 2(3): 215–43
Ito K, Iwatsubo T, Kanamitsu S, et al. Prediction of pharmacokinetic alterations caused by drug-drug interactions: metabolic interaction in the liver. Pharmacol Rev 1998; 50: 387–411
Silverman RB. Mechanism-based enzyme inactivation: chemistry and enzymology. Boca Raton (FL): CRC Press, 1998
Chen Q, Ngui JS, Doss GA, et al. Cytochrome P450 3A4-mediated bioactivation of raloxifene: irreversible enzyme inhibition and thiol adduct formation. Chem Res Toxicol 2002; 15(7): 907–14
Hengstler JG, Utesch D, Steinberg P, et al. Cryopreserved primary hepatocytes as a constantly available in vitro model for the evaluation of human and animal drug metabolism and enzyme induction. Drug Metab Rev 2000; 32: 81–118
Crespi CL, Miller VP. The use of heterologously expressed drug metabolizing enzymes: state of the art and prospects for the future. Pharmacol Ther 1999; 84: 121–31
Streetman DS, Bertino JS, Nafziger AN. Phenotyping of drug-metabolizing enzymes in adults: a review of in-vivo cytochrome P450 phenotyping probes. Pharmacogenetics 2000; 10: 187–216
Crespi CL, Penman BW. Use of cDNA-expressed human cytochrome P450 enzymes to study potential drug-drug interactions. Adv Pharmacol 1997; 43: 171–88
Hollenberg PF. Characteristics and common properties of inhibitors, inducers, and activators of CYP enzymes. Drug Metab Rev 2002; 34(1–2): 17–35
Yuan R, Madani S, Wei XX, et al. Evaluation of cytochrome p450 probe substrates commonly used by the pharmaceutical industry to study in vitro drug interactions. Drug Metab Dispos 2002; 30(12): 1311–9
Kenworthy KE, Bloomer JC, Clarke SE, et al. CYP3A4 drug interactions: correlation of 10 in vitro probe substrates. Br J Clin Pharmacol 1999; 48(5): 716–27
Wang RW, Newton DJ, Liu N, et al. Human cytochrome P-450 3A4: in vitro drug-drug interaction patterns are substrate-dependent. Drug Metab Dispos 2000; 28(3): 360–6
Labroo RB, Thummel KE, Kunze KL, et al. Catalytic role of cytochrome P4503A4 in multiple pathways of alfentanil metabolism. Drug Metab Dispos 1995; 23(4): 490–6
Kharasch ED, Thummel KE. Human alfentanil metabolism by cytochrome P450 3A3/4: an explanation for the interindividual variability in alfentanil clearance? Anesth Analg 1993; 76(5): 1033–9
Yun CH, Wood M, Wood AJ, et al. Identification of the pharmacogenetic determinants of alfentanil metabolism: cytochrome P-450 3A4: an explanation of the variable elimination clearance. Anesthesiology 1992; 77(3): 467–74
Kharasch ED, Hoffer C, Walker A, et al. Disposition and miotic effects of oral alfentanil: a potential noninvasive probe for first-pass cytochrome P4503A activity. Clin Pharmacol Ther 2003; 73(3): 199–208
Labroo R, Kharasch ED. Gas chromatographic-mass spectrometric analysis of alfentanil metabolites: application to human liver microsomal alfentanil biotransformation. J Chromatogr B Biomed Appl 1994; 660(1): 85–94
Ahonen J, Olkkola KT, Salmenperä M, et al. Effect of diltiazem on midazolam and alfentanil disposition in patients undergoing coronary artery bypass grafting. Anesthesiology 1996; 85(6): 1246–51
Bartkowski RR, Goldberg ME, Larijani GE, et al. Inhibition of alfentanil metabolism by erythromycin. Clin Pharmacol Ther 1989; 46(1): 99–102
Gorski JC, Jones DR, Hamman MA, et al. Biotransformation of alprazolam by members of the human cytochrome P4503A subfamily. Xenobiotica 1999; 29(9): 931–44
Schmith VD, Cox SR, Zemaitis MA, et al. New high-performance liquid chromatographic method for the determination of alprazolam and its metabolites in serum: instability of 4-hydroxyalprazolam. J Chromatogr 1991; 568(1): 253–60
Yasui N, Otani K, Kaneko S, et al. A kinetic and dynamic study of oral alprazolam with and without erythromycin in humans: in vivo evidence for the involvement of CYP3A4 in alprazolam metabolism. Clin Pharmacol Ther 1996; 59(5): 514–9
Greenblatt DJ, Preskorn SH, Cotreau MM, et al. Fluoxetine impairs clearance of alprazolam but not of clonazepam. Clin Pharmacol Ther 1992; 52: 479–86
Lasher TA, Fleishaker JC, Steenwyk RC, et al. Pharmacokinetic pharmacodynamic evaluation of the combined administration of alprazolam and fluoxetine. Psychopharmacology (Berl) 1991; 104(3): 323–7
Rodrigues AD, Roberts EM, Mulford DJ, et al. Oxidative metabolism of clarithromycin in the presence of human liver microsomes: major role for the cytochrome P4503A (CYP3A) subfamily. Drug Metab Dispos 1997; 25(5): 623–30
Wang JS, Wang W, Xie HG, et al. Effect of troleandomycin on the pharmacokinetics of imipramine in Chinese: the role of CYP3A. Br J Clin Pharmacol 1997; 44(2): 195–8
Albani F, Riva R, Baruzzi A. Clarithromycin-carbamazepine interaction: a case report. Epilepsia 1993; 34(1): 161–2
Sketris IS, Wright MR, West ML. Possible role of the intestinal P-450 enzyme system in a cyclosporine-clarithromycin interaction. Pharmacotherapy 1996; 16(2): 301–5
Abel SM, Back DJ. Cortisol metabolism in vitro: III. Inhibition of microsomal 6 beta-hydroxylase and cytosolic 4-ene-reductase. J Steroid Biochem Mol Biol 1993; 46(6): 827–32
Hunt CM, Watkins PB, Saenger P, et al. Heterogeneity of CYP3A isoforms metabolizing erythromycin and cortisol. Clin Pharmacol Ther 1992; 51(1): 18–23
Joellenbeck Z, Qian L, Zarba A, et al. Urinary 6 beta-hydroxy-cortisol/cortisol ratios measured by high-performance liquid chromatography for use as a biomarker for the human cytochrome P-450 3A4. Cancer Epidemiol Biomarkers Prev 1992; 1: 567–72
Seidegard J, Dahlstrom K, Kullberg A. Effect of grapefruit juice on urinary 6 beta-hydroxycortisol/cortisol excretion. Clin Exp Pharmacol Physiol 1998; 25(5): 379–81
Koup JR, Anderson GD, Loi CM. Effect of troglitazone on urinary excretion of 6beta-hydroxycortisol. J Clin Pharmacol 1998; 38(9): 815–8
Micuda S, Hodac M, Sispera L, et al. Influence of amiodarone on urinary excretion of 6beta-hydroxycortisol in humans. Physiol Res 2001; 50(2): 191–6
Hammerstein J, Daume E, Simon A, et al. Influence of gestodene and desogestrel as components of low-dose oral contraceptives on the pharmacokinetics of ethinyl estradiol (EE2), on serum CBG and on urinary cortisol and 6 beta-hydroxycortisol. Contraception 1993; 47(3): 263–81
Jurima-Romet M, Crawford K, Cyr T, et al. Terfenadine metabolism in human liver: in vitro inhibition by macrolide antibiotics and azole antifungals. Drug Metab Dispos 1994; 22(6): 849–57
Christians U, Strohmeyer S, Kownatzki R, et al. Investigations on the metabolic pathways of cyclosporine: II. Elucidation of the metabolic pathways in vitro by human liver microsomes. Xenobiotica 1991; 21(9): 1199–210
Kronbach T, Fischer V, Meyer UA. Cyclosporine metabolism in human liver: identification of a cytochrome P-450III gene family as the major cyclosporine-metabolizing enzyme explains interactions of cyclosporine with other drugs. Clin Pharmacol Ther 1988; 43(6): 630–5
Combalbert J, Fabre I, Fabre G, et al. Metabolism of cyclosporin A: IV. Purification and identification of the rifampicin-inducible human liver cytochrome P-450 (cyclosporin A oxidase) as a product of P450IIIA gene subfamily. Drug Metab Dispos 1989; 17(2): 197–207
Tjia JF, Back DJ, Breckenridge AM. Calcium channel antagonists and cyclosporine metabolism: in vitro studies with human liver microsomes. Br J Clin Pharmacol 1989; 28(3): 362–5
Cakaloglu Y, Tredger JM, Devlin J, et al. Importance of cytochrome P-450IIIA activity in determining dosage and blood levels of FK 506 and cyclosporine in liver transplant recipients. Hepatology 1994; 20(2): 309–16
Spicer ST, Liddle C, Chapman JR, et al. The mechanism of cyclosporine toxicity induced by clarithromycin. Br J Clin Pharmacol 1997; 43(2): 194–6
Vereerstraeten P, Thiry P, Kinnaert P, et al. Influence of erythromycin on cyclosporine pharmacokinetics. Transplantation 1987; 44(1): 155–6
Fleming CM, Branch RA, Wilkinson GR, et al. Human liver microsomal N-hydroxylation of dapsone by cytochrome P-4503A4. Mol Pharmacol 1992; 41(5): 975–80
Gill HJ, Tingle MD, Park BK. N-hydroxylation of dapsone by multiple enzymes of cytochrome P450: implications for inhibition of haemotoxicity. Br J Clin Pharmacol 1995; 40(6): 531–8
Kinirons MT, O’shea D, Downing TE, et al. Absence of correlations among three putative in vivo probes of human cytochrome P4503A activity in young healthy men. Clin Pharmacol Ther 1993; 54(6): 621–9
Frye RF, Matzke GR, Adedoyin A, et al. Validation of the five-drug Pittsburgh cocktail approach for assessment of selective regulation of drug-metabolizing enzymes. Clin Pharmacol Ther 1997; 62(4): 365–76
Joshi JV, Maitra A, Sankolli G, et al. Norethisterone and ethinyl estradiol kinetics during dapsone therapy. J Assoc Physicians India 1984; 32(2): 191–3
Wang RW, Newton DJ, Scheri TD, et al. Human cytochrome P450 3A4-catalyzed testosterone 6 beta-hydroxylation and erythromycin N-demethylation: competition during catalysis. Drug Metab Dispos 1997; 25(4): 502–7
Rivory LP, Slaviero KA, Hoskins JM, et al. The erythromycin breath test for the prediction of drug clearance. Clin Pharmacokinet 2001; 40(3): 151–8
Watkins PB, Wrighton SA, Maurel P, et al. Identification of an inducible form of cytochrome P-450 in human liver. Proc Natl Acad Sci U S A 1985; 82(18): 6310–4
Watkins PB, Murray SA, Winkelman LG, et al. Erythromycin breath test as an assay of glucocorticoid-inducible liver cytochromes P-450: studies in rats and patients. J Clin Invest 1989; 83(2): 688–97
Lown K, Kolars J, Turgeon K, et al. The erythromycin breath test selectively measures P450IIIA in patients with severe liver disease. Clin Pharmacol Ther 1992; 51(3): 229–38
Schmidt LE, Olsen AK, Stentoft K, et al. Early postoperative erythromycin breath test correlates with hepatic cytochrome P4503A activity in liver transplant recipients. Clin Pharmacol Ther 2001; 70(5): 446–54
Cheng CL, Smith DE, Carver PL, et al. Steady-state pharmacokinetics of delavirdine in HIV-positive patients: effect on erythromycin breath test. Clin Pharmacol Ther 1997; 61(5): 531–43
Schmid SE, Au WY, Hill DE, et al. Cytochrome P-450-dependent oxidation of the 17 alpha-ethynyl group of synthetic steroids: D-homoannulation or enzyme inactivation. Drug Metab Dispos 1983; 11(6): 531–6
Guengerich FP. Oxidation of 17-ethynylestradiol by human liver cytochrome P450. Mol Pharmacol 1988; 33(5): 500–8
Guengerich FP. Mechanism-based inactivation of human liver microsomal cytochrome P-450 IIIA4 by gestodene. Chem Res Toxicol 1990; 3(4): 363–71
Ouellet D, Hsu A, Qian J, et al. Effect of ritonavir on the pharmacokinetics of ethinyl oestradiol in healthy female volunteers. Br J Clin Pharmacol 1998; 46(2): 111–6
Wang JS, Backman JT, Taavitsainen P, et al. Involvement of CYP1A2 and CYP3A4 in lidocaine N-deethylation and 3-hydroxylation in humans. Drug Metab Dispos 2000; 28(8): 959–65
Bargetzi MJ, Aoyama T, Gonzalez FJ, et al. Lidocaine metabolism in human liver microsomes by cytochrome P450IIIA4. Clin Pharmacol Ther 1989; 46(5): 521–7
Imaoka S, Enomoto K, Oda Y, et al. Lidocaine metabolism by human cytochrome P-450s purified from hepatic microsomes: comparison of those with rat hepatic cytochrome P-450s. J Pharmacol Exp Ther 1990; 255: 1385–91
O’Neal CL, Poklis A. Sensitive HPLC for simultaneous quantification of lidocaine and its metabolites monoethylglycinexylidide and glycinexylidide in serum. Clin Chem 1996; 42(2): 330–1
Testa R, Caglieris S, Risso D, et al. Monoethylglycinexylidide formation measurement as a hepatic function test to assess severity of chronic liver disease. Am J Gastroenterol 1997; 92(12): 2268–73
Swart EL, van der Hoven B, Groeneveld AB, et al. Correlation between midazolam and lignocaine pharmacokinetics and MEGX formation in healthy volunteers. Br J Clin Pharmacol 2002; 53(2): 133–9
Orszulak-Michalak D, Owczarek J, Wiktorowska-Owczarek AK. The influence of midazolam on plasma concentrations and pharmacokinetic parameters of lidocaine in rabbits. Pharmacol Res 2002; 45(1): 11–4
Tanaka E, Breimer DD. In vivo function tests of hepatic drug-oxidizing capacity in patients with liver disease. J Clin Pharm Ther 1997; 22(4): 237–49
Isohanni MH, Neuvonen P, Olkkola KT. Effect of erythromycin and itraconazole on the pharmacokinetics of oral lignocaine. Pharmacol Toxicol 1999; 84(3): 143–6
Gorski JC, Hall SD, Jones DR, et al. Regioselective biotransformation of midazolam by members of the human cytochrome P450 3A (CYP3A) subfamily. Biochem Pharmacol 1994; 47(9): 1643–53
Carrillo JA, Ramos SI, Agundez JA, et al. Analysis of midazolam and metabolites in plasma by high-performance liquid chromatography: probe of CYP3A. Ther Drug Monit 1998; 20(3): 319–24
Wen X, Wang JS, Neuvonen PJ, et al. Isoniazid is a mechanism-based inhibitor of cytochrome P450 1A2, 2A6, 2C19 and 3A4 isoforms in human liver microsomes. Eur J Clin Pharmacol 2002; 57(11): 799–804
Tinel M, Descatoire V, Larrey D, et al. Effects of clarithromycin on cytochrome P-450. Comparison with other macrolides. J Pharmacol Exp Ther 1989; 250(2): 746–51
Mayhew BS, Jones DR, Hall SD. An in vitro model for predicting in vivo inhibition of cytochrome P450 3A4 by metabolic intermediate complex formation. Drug Metab Dispos 2000; 28(9): 1031–7
Jones DR, Gorski JC, Hamman MA, et al. Diltiazem inhibition of cytochrome P-450 3A activity is due to metabolite intermediate complex formation. J Pharmacol Exp Ther 1999; 290(3): 1116–25
Thummel KE, Shen DD, Podoll TD, et al. Use of midazolam as a human cytochrome P450 3A probe: I. In vitro-in vivo correlations in liver transplant patients. J Pharmacol Exp Ther 1994; 271(1): 549–56
Gorski JC, Jones DR, Haehnerdaniels BD, et al. The contribution of intestinal and hepatic CYP3A to the interaction between midazolam and clarithromycin. Clin Pharmacol Ther 1998; 64(2): 133–43
Ma B, Prueksaritanont T, Lin JH. Drug interactions with calcium channel blockers: possible involvement of metabolite-intermediate complexation with CYP3A. Drug Metab Dispos 2000; 28(2): 125–30
Gonzalez FJ, Schmid BJ, Umeno M, et al. Human P450PCN1: sequence, chromosome localization, and direct evidence through cDNA expression that P450PCN1 is nifedipine oxidase. DNA 1988; 7(2): 79–86
Breimer DD, Schellens JH, Soons PA. Nifedipine: variability in its kinetics and metabolism in man. Pharmacol Ther 1989; 44(3): 445–54
Balogh A, Gessinger S, Svarovsky U, et al. Can oral contraceptive steroids influence the elimination of nifedipine and its primary pryidine metabolite in humans? Eur J Clin Pharmacol 1998; 54(9-10): 729–34
Greenblatt DJ, von Moltke LL, Harmatz JS, et al. Differential impairment of triazolam and zolpidem clearance by ritonavir. J Acquir Immune Defic Syndr 2000; 24(2): 129–36
Ling KH, Leeson GA, Burmaster SD, et al. Metabolism of terfenadine associated with CYP3A (4) activity in human hepatic microsomes. Drug Metab Dispos 1995; 23(6): 631–6
Rodrigues AD, Mulford DJ, Lee RD, et al. In vitro metabolism of terfenadine by a purified recombinant fusion protein containing cytochrome P4503A4 and NADPH-P450 reductase: comparison to human liver microsomes and precision-cut liver tissue slices. Drug Metab Dispos 1995; 23(7): 765–75
Yun CH, Okerholm RA, Guengerich FP. Oxidation of the antihistaminic drug terfenadine in human liver microsomes: role of cytochrome P-450 3A (4) in N-dealkylation and C-hydroxylation. Drug Metab Dispos 1993; 21(3): 403–9
Terhechte A, Blaschke G. Investigation of the stereoselective metabolism of the chiral H1-antihistaminic drug terfenadine by high-performance liquid chromatography. J Chromatogr A 1995; 694(1): 219–25
Kumar GN, Rodrigues A, Buko AM, et al. Cytochrome P450-mediated metabolism of the HIV-1 protease inhibitor ritonavir (ABT-538) in human liver microsomes. J Pharmacol Exp Ther 1996; 277(1): 423–31
Jurima-Romet M, Wright M, Neigh S. Terfenadine-antidepressant interactions: an in vitro inhibition study using human liver microsomes. Br J Clin Pharmacol 1998; 45(3): 318–21
Waxman DJ, Lapenson DP, Aoyama T, et al. Steroid hormone hydroxylase specificities of eleven cDNA-expressed human cytochrome P450s. Arch Biochem Biophys 1991; 290(1): 160–6
Draper AJ, Madan A, Smith K, et al. Development of a non-high pressure liquid chromatography assay to determine testosterone hydroxylase (CYP3A) activity in human liver microsomes. Drug Metab Dispos 1998; 26(4): 299–304
Testino Jr SA, Ozarowski J, Thurston AW, et al. Determination of testosterone and 6beta-hydroxytestosterone by gas chromatography-selected ion monitoring-mass spectrometry for the characterization of cytochrome p450 3A activity. J Chromatogr B Biomed Sci Appl 1999; 734(1): 73–81
Hanioka N, Ozawa S, Jinno H, et al. Interaction of irinotecan (CPT-11) and its active metabolite 7-ethyl-10-hydroxy-camptothecin (SN-38) with human cytochrome P450 enzymes. Drug Metab Dispos 2002; 30(4): 391–6
Zhao XJ, Jones DR, Wang YH, et al. Reversible and irreversible inhibition of CYP3A enzymes by tamoxifen and metabolites. Xenobiotica 2002; 32(10): 863–78
Masubuchi Y, Horie T. Mechanism-based inactivation of cytochrome P450s 1A2 and 3A4 by dihydralazine in human liver microsomes. Chem Res Toxicol 1999; 12(10): 1028–32
Masubuchi Y, Horie T. Dihydralazine-induced inactivation of cytochrome P450 enzymes in rat liver microsomes. Drug Metab Dispos 1998; 26(4): 338–42
He K, Woolf TF, Hollenberg PF. Mechanism-based inactivation of cytochrome P-450-3A4 by mifepristone (RU486). J Pharmacol Exp Ther 1999; 288(2): 791–7
He K, Iyer KR, Hayes RN, et al. Inactivation of cytochrome P450 3A4 by bergamottin, a component of grapefruit juice. Chem Res Toxicol 1998; 11(4): 252–9
von Moltke LL, Greenblatt DJ, Harmatz JS, et al. Triazolam biotransformation by human liver microsomes in vitro: effects of metabolic inhibitors and clinical confirmation of a predicted interaction with ketoconazole. J Pharmacol Exp Ther 1996; 276(2): 370–9
Perloff MD, von Moltke LL, Court MH, et al. Midazolam and triazolam biotransformation in mouse and human liver microsomes: relative contribution of CYP3A and CYP2C isoforms. J Pharmacol Exp Ther 2000; 292(2): 618–28
Voorman RL, Maio SM, Payne NA, et al. Microsomal metabolism of delavirdine: evidence for mechanism-based inactivation of human cytochrome P450 3A. J Pharmacol Exp Ther 1998; 287(1): 381–8
von Moltke LL, Greenblatt DJ, Grassi JM, et al. Protease inhibitors as inhibitors of human cytochromes P450: high risk associated with ritonavir. J Clin Pharmacol 1998; 38(2): 106–11
Koudriakova T, Iatsimirskaia E, Utkin I, et al. Metabolism of the human immunodeficiency virus protease inhibitors indinavir and ritonavir by human intestinal microsomes and expressed cytochrome P4503A4/3A5: mechanism-based inactivation of cytochrome P4503A by ritonavir. Drug Metab Dispos 1998; 26(6): 552–61
von Moltke LL, Durol AL, Duan SX, et al. Potent mechanism-based inhibition of human CYP3A in vitro by amprenavir and ritonavir: comparison with ketoconazole. Eur J Clin Pharmacol 2000; 56(3): 259–61
Kanamitsu S, Ito K, Green CE, et al. Prediction of in vivo interaction between triazolam and erythromycin based on in vitro studies using human liver microsomes and recombinant human CYP3A4. Pharm Res 2000; 17(4): 419–26
Greenblatt DJ, von Moltke LL, Harmatz JS, et al. Inhibition of triazolam clearance by macrolide antimicrobial agents: in vitro correlates and dynamic consequences. Clin Pharmacol Ther 1998; 64(3): 278–85
Kosuge K, Nishimoto M, Kimura M, et al. Enhanced effect of triazolam with diltiazem. Br J Clin Pharmacol 1997; 43(4): 367–72
Halpert JR, Guengerich FP, Bend JR, et al. Selective inhibitors of cytochromes P450. Toxicol Appl Pharmacol 1994; 125: 163–75
Gelboin HV, Krausz KW, Gonzalez FJ, et al. Inhibitory monoclonal antibodies to human cytochrome P450 enzymes: a new avenue for drug discovery. Trends Pharmacol Sci 1999; 20(11): 432–8
Voorman RL, Maio SM, Hauer MJ, et al. Metabolism of delavirdine, a human immunodeficiency virus type-1 reverse transcriptase inhibitor, by microsomal cytochrome P450 in humans, rats, and other species: probable involvement of CYP2D6 and CYP3A. Drug Metab Dispos 1998; 26(7): 631–9
Treluyer JM, Bowers G, Cazali N, et al. Oxidative metabolism of amprenavir in the human liver. Effect of the CYP3A maturation. Drug Metab Dispos 2003; 31(3): 275–81
Jacobsen W, Christians U, Benet LZ. In vitro evaluation of the disposition of A novel cysteine protease inhibitor. Drug Metab Dispos 2000; 28(11): 1343–51
Lin HL, Kent UM, Hollenberg PF. Mechanism-based inactivation of cytochrome P450 3A4 by 17 alpha-ethynylestradiol: evidence for heme destruction and covalent binding to protein. J Pharmacol Exp Ther 2002; 301(1): 160–7
Decker CJ, Laitinen LM, Bridson GW, et al. Metabolism of amprenavir in liver microsomes: role of CYP3A4 inhibition for drug interactions. J Pharm Sci 1998; 87(7): 803–7
Pessayre D, Tinel M, Larrey D, et al. Inactivation of cytochrome P-450 by a troleandomycin metabolite: protective role of glutathione. J Pharmacol Exp Ther 1983; 224(3): 685–91
Miura T, Iwasaki M, Komori M, et al. Decrease in a constitutive form of cytochrome P-450 by macrolide antibiotics. J Antimicrob Chemother 1989; 24(4): 551–9
Chan WK, Delucchi AB. Resveratrol, a red wine constituent, is a mechanism-based inactivator of cytochrome P450 3A4. Life Sci 2000; 67(25): 3103–12
Waxman DJ. P450 gene induction by structurally diverse xenochemicals: central role of nuclear receptors CAR, PXR, and PPAR. Arch Biochem Biophys 1999; 369(1): 11–23
Sueyoshi T, Negishi M. Phenobarbital response elements of cytochrome P450 genes and nuclear receptors. Annu Rev Pharmacol Toxicol 2001; 41: 123–43
Lehmann JM, McKee DD, Watson MA, et al. The human orphan nuclear receptor PXR is activated by compounds that regulate CYP3A4 gene expression and cause drug interactions. J Clin Invest 1998; 102: 1016–23
Gibson GG, Plant NJ, Swales KE, et al. Receptor-dependent transcriptional activation of cytochrome P4503A genes: induction mechanisms, species differences and interindividual variation in man. Xenobiotica 2002; 32(3): 165–206
Quattrochi LC, Guzelian PS. CYP3A regulation: from pharmacology to nuclear receptors. Drug Metab Dispos 2001; 29(5): 615–22
Xie W, Evans RM. Orphan nuclear receptors: the exotics of xenobiotics. J Biol Chem 2001; 276(41): 37739–42
Goodwin B, Redinbo MR, Kliewer SA. Regulation of CYP3A gene transcription by the pregnane X receptor. Annu Rev Pharmacol Toxicol 2002; 42: 1–23
Kocarek TA, Schuetz EG, Strom SC, et al. Comparative analysis of cytochrome P4503A induction in primary cultures of rat, rabbit, and human hepatocytes. Drug Metab Dispos 1995; 23(3): 415–21
Madan A, Graham RA, Carroll KM, et al. Effects of prototypical microsomal enzyme inducers on cytochrome P450 expression in cultured human hepatocytes. Drug Metab Dispos 2003; 31(4): 421–31
Luo G, Cunningham M, Kim S, et al. CYP3A4 induction by drugs: correlation between a pregnane X receptor reporter gene assay and CYP3A4 expression in human hepatocytes. Drug Metab Dispos 2002; 30(7): 795–804
El-Sankary W, Gibson GG, Ayrton A, et al. Use of a reporter gene assay to predict and rank the potency and efficacy of CYP3A4 inducers. Drug Metab Dispos 2001; 29(11): 1499–504
Ledirac N, de Sousa G, Fontaine F, et al. Effects of macrolide antibiotics on CYP3A expression in human and rat hepatocytes: interspecies differences in response to troleandomycin. Drug Metab Dispos 2000; 28(12): 1391–3
LeCluyse EL. Human hepatocyte culture systems for the in vitro evaluation of cytochrome P450 expression and regulation. Eur J Pharm Sci 2001; 13(4): 343–68
Lightning LK, Jones JP, Friedberg T, et al. Mechanism-based inactivation of cytochrome P450 3A4 by L-754,394. Biochemistry 2000; 39(15): 4276–87
Ekins S, Waller CL, Swaan PW, et al. Progress in predicting human ADME parameters in silico. J Pharmacol Toxicol Methods 2000; 44(1): 251–72
Ekins S, Bravi G, Binkley S, et al. Three- and four-dimensional quantitative structure activity relationship analyses of cytochrome P-450 3A4 inhibitors. J Pharmacol Exp Ther 1999; 290(1): 429–38
Ekins S, Bravi G, Wikel JH, et al. Three-dimensional-quantitative structure activity relationship analysis of cytochrome P-450 3A4 substrates. J Pharmacol Exp Ther 1999; 291(1): 424–33
Ekins S, Ring BJ, Grace J, et al. Present and future in vitro approaches for drug metabolism. J Pharmacol Toxicol Method 2000; 44(1): 313–24
Lewis DFV. Molecular modeling of human cytochrome P450-substrate interactions. Drug Metab Rev 2002; 34(1–2): 55–67
Ekins S, Wrighton SA. Application of in silico approaches to predicting drug-drug interactions. J Pharmacol Toxicol Method 2001; 45(1): 65–9
Ekins S, de Groot MJ, Jones JP. Pharmacophore and three-dimensional quantitative structure activity relationship methods for modeling cytochrome P450 active sites. Drug Metab Dispos 2001; 29(7): 936–44
Boobis AR, Sesardic D, Murray BP, et al. Species variation in the response of the cytochrome P450-dependent monooxygenase system to inducers and inhibitors. Xenobiotica 1990; 20: 1139–61
Lin JH. Species similarities and differences in pharmacokinetics. Drug Metab Dispos 1995; 23(10): 1008–21
Lewis DF, Ionnides C, Parke DV. Cytochrome P450 and species differences in xenobiotic metabolism and activation of carcinogen. Environ Health Perspect 1998; 106: 633–41
Brockmoller J, Roots I. Assessment of liver metabolic function: clinical implications. Clin Pharmacokinet 1994; 27(3): 216–48
Kim RB, Wandel C, Leake B, et al. Interrelationship between substrates and inhibitors of human CYP3A and P-glycoprotein. Pharm Res 1999; 16(3): 408–14
Villikka K, Kivisto KT, Neuvonen PJ. The effect of rifampin on the pharmacokinetics of oral and intravenous ondansetron. Clin Pharmacol Ther 1999; 65(4): 377–81
Villikka K, Kivisto KT, Lamberg TS, et al. Concentrations and effects of zopiclone are greatly reduced by rifampicin. Br J Clin Pharmacol 1997; 43(5): 471–4
Villikka K, Kivisto KT, Backman JT, et al. Triazolam is ineffective in patients taking rifampin. Clin Pharmacol Ther 1997; 61(1): 8–14
Hsu A, Granneman GR, Bertz RJ. Ritonavir: clinical pharmacokinetics and interactions with other anti-HIV agents. Clin Pharmacokinet 1998; 35(4): 275–91
Larry D, Funk-Brentano C, Breil P, et al. Effect of erythromycin on hepatic drug-metabolizing enzymes in humans. Biochem Pharmacol 1983; 32(6): 1063–8
Ohmori S, Ishii I, Kuriya S, et al. Effects of clarithromycin and its metabolites on the mixed function oxidase system in hepatic microsomes of rat. Drug Metab Dispos 1993; 21(2): 358–63
Hlavica P, Golly I, Lehnerer M, et al. Primary aromatic amines: their N-oxidative bioactivation. Hum Exp Toxicol 1997; 16(8): 441–8
Hlavica P. N-oxidative transformation of free and n-substituted amine functions by cytochrome P450 as means of bioactivation and detoxication. Drug Metab Rev 2002; 34(3): 451–77
Khojasteh-Bakht SC, Koenigs LL, Peter RM, et al. (R)- (+)-menthofuran is a potent, mechanism-based inactivator of human liver cytochrome P450 2A6. Drug Metab Dispos 1998; 26(7): 701–4
Bensoussan C, Delaforge M, Mansuy D. Particular ability of cytochromes P450 3A to form inhibitory P450-iron-metabolite complexes upon metabolic oxidation of aminodrugs. Biochem Pharmacol 1995; 49(5): 591–602
Pershing LK, Franklin MR. Cytochrome P-450 metabolic-intermediate complex formation and induction by macrolide antibiotics: a new class of agents. Xenobiotica 1982; 12: 687–99
Periti P, Mazzei T, Mini E, et al. Pharmacokinetic drug interactions of macrolides. Clin Pharmacokinet 1992; 23(2): 106–31
Ludden TM. Pharmacokinetic interactions of the macrolide antibiotics. Clin Pharmacokinet 1985; 10(1): 63–79
von Rosensteil NA, Adam D. Macrolide antibacterials: drug interactions of clinical significance. Drug Saf 1995; 13(2): 105–22
Amacher DE, Schomaker SJ, Retsema JA. Comparison of the effects of the new azalide antibiotic, azithromycin, and erythromycin estolate on rat liver cytochrome P-450. Antimicrob Agents Chemother 1991; 35(6): 1186–90
Delaforge M, Jaouen M, Mansuy D. Dual effects of macrolide antibiotics on rat liver cytochrome P-450: induction and formation of metabolite-complexes: a structure-activity relationship. Biochem Pharmacol 1983; 32(15): 2309–18
Larrey D, Tinel M, Pessayre D. Formation of inactive cytochrome P-450 Fe (II)-metabolite complexes with several erythromycin derivatives but not with josamycin and midecamycin in rats. Biochem Pharmacol 1983; 32(9): 1487–93
Guengerich FP. Metabolism of 17 alpha-ethynylestradiol in humans. Life Sci 1990; 47(22): 1981–8
Chiba M, Nishime JA, Lin JH. Potent and selective inactivation of human liver microsomal cytochrome P-450 isoforms by L-754,394, an investigational human immune deficiency virus protease inhibitor. J Pharmacol Exp Ther 1995; 275(3): 1527–34
Lin JH, Chiba M, Chen IW, et al. Time- and dose-dependent pharmacokinetics of L-754,394, an HIV protease inhibitor, in rats, dogs and monkeys. J Pharmacol Exp Ther 1995; 274(1): 264–9
Lillibridge JH, Liang BH, Kerr BM, et al. Characterization of the selectivity and mechanism of human cytochrome P450 inhibition by the human immunodeficiency virus-protease inhibitor nelfinavir mesylate. Drug Metab Dispos 1998; 26(7): 609–16
Khan KK, He YQ, Domanski TL, et al. Midazolam oxidation by cytochrome P450 3A4 and active-site mutants: an evaluation of multiple binding sites and of the metabolic pathway that leads to enzyme inactivation. Mol Pharmacol 2002; 61(3): 495–506
Jang GR, Benet LZ. Antiprogestin-mediated inactivation of cytochrome P450 3A4. Pharmacology 1998; 56(3): 150–7
Guengerich FP. Cytochrome P-450 3A4: regulation and role in drug metabolism. Annu Rev Pharmacol Toxicol 1999; 39: 1–17
Ishigami M, Honda T, Takasaki W, et al. A comparison of the effects of 3-hydroxy-3-methylglutaryl-coenzyme a (HMG-CoA) reductase inhibitors on the CYP3A4-dependent oxidation of mexazolam in vitro. Drug Metab Dispos 2001; 29: 282–8
Riley RJ, Parker AJ, Trigg S, et al. Development of a generalized, quantitative physicochemical model of CYP3A4 inhibition for use in early drug discovery. Pharm Res 2001; 18: 652–5
Szklarz GD, Halpert JR. Molecular modeling of cytochrome P450 3A4. J Comput-Aided Mol Des 1997; 11: 265–72
Harlow GR, Halpert JR. Alanine-scanning mutagenesis of a putative substrate recognition site in human cytochrome P450 3A4: role of residues 210 and 211 in flavonoid activation and substrate specificity. J Biol Chem 1997; 272: 5396–402
Shou M, Grogan J, Mancewicz JA, et al. Activation of CYP3A4: evidence for the simultaneous binding of two substrates in a cytochrome P450 active site. Biochemistry 1994; 33(21): 6450–5
Korzekwa KR, Krishnamachary N, Shou M, et al. Evaluation of atypical cytochrome P450 kinetics with two-substrate models: evidence that multiple substrates can simultaneously bind to cytochrome P450 active sites. Biochemistry 1998; 37: 4137–47
Schrag ML, Wienkers LC. Covalent alteration of the CYP3A4 active site: evidence for multiple substrate binding domains. Arch Biochem Biophys 2001; 391(1): 49–55
Ekins S, Stresser DM, Williams JA. In vitro and pharmacophore insights into CYP3A enzymes. Trends Pharmacol Sci 2003; 24(4): 161–6
Domanski TL, Halpert JR. Analysis of mammalian cytochrome P450 structure and function using site-directed mutagenesis. Curr Drug Metab 2001; 2(4): 117–37
Harlow GR, Halpert JR. Analysis of human cytochrome P450 3A4 cooperativity: construction and characterization of a site-directed mutant that displays hyperbolic steroid hydroxylation kinetics. Proc Natl Acad Sci U S A 1998; 95: 6636–41
Ueng Y-F, Kuwabara T, Chun Y-J, et al. Cooperativity in oxidations catalyzed by cytochrome P450 3A4. Biochemistry 1997; 36: 370–81
Schrag ML, Wienkers LC. Topological alteration of the CYP3A4 active site by the divalent cation Mg (2+). Drug Metab Dispos 2000; 28(10): 1198–201
Ghosal A, Satoh H, Thomas PE, et al. Inhibition and kinetics of cytochrome P4503A activity in microsomes from rat, human, and cDNA-expressed human cytochrome P450. Drug Metab Dispos 1996; 24(9): 940–7
Hosea NA, Miller GH, Guengerich FP. Elucidation of distinct ligand binding sites for cytochrome P450 3A4. Biochemistry 2000; 39: 5929–39
Lin JH, Lu AYH. Inhibition and induction of cytochrome P450 and the clinical implications. Clin Pharmacokinet 1998; 35: 361–90
Osawa Y, Pohl LR. Covalent bonding of the prosthetic heme to protein: a potential mechanism for suicide inactivation or activation of hemoproteins. Chem Res Toxicol 1989; 2(3): 131–41
Ortiz de Montellano PR, Correia MA. Inhibition of cytochrome P450. In: Ortiz de Montellano PR, editor. Cytochrome P450: structure, mechanism and biochemistry. New York: Plenum Press, 1995: 305–66
He K, He YA, Szklarz GD, et al. Secobarbital-mediated inactivation of cytochrome P450 2B1 and its active site mutants: partitioning between heme and protein alkylation and epoxidation. J Biol Chem 1996; 271(42): 25864–72
Labbe G, Descatoire V, Beaune P, et al. Suicide inactivation of cytochrome P-450 by methoxsalen: evidence for the covalent binding of a reactive intermediate to the protein moiety. J Pharmacol Exp Ther 1989; 250(3): 1034–42
Mays DC, Hilliard JB, Wong DD, et al. Bioactivation of 8-methoxypsoralen and irreversible inactivation of cytochrome P-450 in mouse liver microsomes: modification by monoclonal antibodies, inhibition of drug metabolism and distribution of covalent adducts. J Pharmacol Exp Ther 1990; 254(2): 720–31
Gan LS, Acebo AL, Alworth WL. 1-Ethynylpyrene, a suicide inhibitor of cytochrome P-450 dependent benzo[a]pyrene hydroxylase activity in liver microsomes. Biochemistry 1984; 23: 3827–36
Roberts P, Kitteringham NR, Park BK. Elucidation of the structural requirements for the bioactivation of mianserin in-vitro. J Pharm Pharmacol 1993; 45(7): 663–5
Yun CH, Hammons GJ, Jones G, et al. Modification of cytochrome P450 1A2 enzymes by the mechanism-based inactivator 2-ethynylnaphthalene and the photoaffinity label 4-azidobiphenyl. Biochemistry 1992; 31(43): 10556–63
Cai Y, Baer-Dubowska W, Ashwood-Smith MJ, et al. Mechanism-based inactivation of hepatic ethoxyresorufin O-dealkylation activity by naturally occurring coumarins. Chem Res Toxicol 1996; 9(4): 729–36
Halpert J, Hammond D, Neal RA. Inactivation of purified rat liver cytochrome P-450 during the metabolism of parathion (diethyl p-nitrophenyl phosphorothionate). J Biol Chem 1980; 255: 1080–9
Halpert J. Further studies of the suicide inactivation of purified rat liver cytochrome P450 by chloramphenicol. Mol Pharmacol 1982; 21: 166–72
Franklin MR. Cytochrome P450 metabolic intermediate complexes from macrolide antibiotics and related compounds. Methods Enzymol 1991; 206: 559–73
Kent UM, Aviram M, Rosenblat M, et al. The licorice root derived isoflavan glabridin inhibits the activities of human cytochrome P450S 3A4, 2B6, and 2C9. Drug Metab Dispos 2002; 30(6): 709–15
Ortiz de Montellano PR, Komives EA. Branchpoint for heme alkylation and metabolite formation in the oxidation of arylacetylenes by cytochrome P450. J Biol Chem 1985; 260: 3330–6
Guengerich FP. Covalent binding to apoprotein is a major fate of heme in a variety of reactions in which cytochrome P450 is destroyed. Biochem Biophys Res Commun 1986; 138: 193–8
Correia MA, Decker C, Sugiyama K, et al. Degradation of rat hepatic cytochrome P450 heme by 3,5-dicarbethoxy-2,6-dimethyl-4-ethyl-1,4-dihydropyridine to irreversibly bound protein adducts. Arch Biochem Biophys 1987; 258: 436–45
Yao K, Falick AM, Patel N, et al. Cumene hydroperoxide-mediated inactivation of cytochrome P450 2B1: identification of an active site heme-modified peptide. J Biol Chem 1993; 268: 59–65
Kent UM, Mills DE, Rajnarayanan RV, et al. Effect of 17-alpha-ethynylestradiol on activities of cytochrome P450 2B (P450 2B) enzymes: characterization of inactivation of P450s 2B1 and 2B6 and identification of metabolites. J Pharmacol Exp Ther 2002; 300(2): 549–58
Tudela J, Garcia Canovas F, Varon R, et al. Transient-phase kinetics of enzyme inactivation induced by suicide substrates. Biochim Biophys Acta 1987; 912(3): 408–16
Yeo KR, Yeo WW. Inhibitory effects of verapamil and diltiazem on simvastatin metabolism in human liver microsomes. Br J Clin Pharmacol 2001; 51(5): 461–70
Prueksaritanont T, Ma B, Tang C, et al. Metabolic interactions between mibefradil and HMG-CoA reductase inhibitors: an in vitro investigation with human liver preparations. Br J Clin Pharmacol 1999; 47(3): 291–8
Pichard L, Fabre I, Fabre G, et al. Cyclosporin A drug interactions: screening for inducers and inhibitors of cytochrome P-450 (cyclosporin A oxidase) in primary cultures of human hepatocytes and in liver microsomes. Drug Metab Dispos 1990; 18(5): 595–606
Stresser DM, Blanchard AP, Turner SD, et al. Substrate-dependent modulation of CYP3A4 catalytic activity: analysis of 27 test compounds with four fluorometric substrates. Drug Metab Dispos 2000; 28(12): 1440–8
Wrighton SA, Ring BJ. Inhibition of human CYP3A catalyzed 1′-hydroxy midazolam formation by ketoconazole, nifedipine, erythromycin, cimetidine and nizatidine. Pharm Res 1994; 11: 921–4
Schmiedlin-Ren P, Edwards DJ, Fitzsimmons ME, et al. Mechanisms of enhanced oral availability of CYP3A4 substrates by grapefruit constituents: decreased enterocyte CYP3A4 concentration and mechanism-based inactivation by furanocoumarins. Drug Metab Dispos 1997; 25(11): 1228–33
Le Goff-Klein N, Koffel JC, Jung L, et al. In vitro inhibition of simvastatin metabolism, a HMG-CoA reductase inhibitor in human and rat liver by bergamottin, a component of grapefruit juice. Eur J Pharm Sci 2003; 18(1): 31–5
Guo LQ, Fukuda K, Ohta T, et al. Role of furanocoumarin derivatives on grapefruit juice-mediated inhibition of human CYP3A activity. Drug Metab Dispos 2000; 28(7): 766–71
Voorman RL, Payne NA, Wienkers LC, et al. Interaction of delavirdine with human liver microsomal cytochrome P450: inhibition of CYP2C9, CYP2C19, and CYP2D6. Drug Metab Dispos 2001; 29(1): 41–7
von Moltke LL, Greenblatt DJ, Granda BW, et al. Inhibition of human cytochrome P450 isoforms by nonnucleoside reverse transcriptase inhibitors. J Clin Pharmacol 2001; 41(1): 85–91
Sutton D, Butler AM, Nadin L, et al. Role of CYP3A4 in human hepatic diltiazem N-demethylation: inhibition of CYP3A4 activity by oxidized diltiazem metabolites. J Pharmacol Exp Ther 1997; 282(1): 294–300
Yamano K, Yamamoto K, Katashima M, et al. Prediction of midazolam-CYP3A inhibitors interaction in the human liver from in vivo/in vitro absorption, distribution, and metabolism data. Drug Metab Dispos 2001; 29 (4 Pt 1): 443–52
Haaz MC, Rivory L, Riche C, et al. Metabolism of irinotecan (CPT-11) by human hepatic microsomes: participation of cytochrome P-450 3A and drug interactions. Cancer Res 1998; 58(3): 468–72
Desta Z, Soukhova NV, Flockhart DA. Inhibition of cytochrome P450 (CYP450) isoforms by isoniazid: potent inhibition of CYP2C19 and CYP3A. Antimicrob Agents Chemother 2001; 45(2): 382–92
Sahali-Sahly Y, Balani SK, Lin JH, et al. In vitro studies on the metabolic activation of the furanopyridine L-754,394, a highly potent and selective mechanism-based inhibitor of cytochrome P450 3A4. Chem Res Toxicol 1996; 9(6): 1007–12
Wandel C, Kim RB, Guengerich FP, et al. Mibefradil is a P-glycoprotein substrate and a potent inhibitor of both P-glycoprotein and CYP3A in vitro. Drug Metab Dispos 2000; 28(8): 895–8
Jang GR, Wrighton SA, Benet LZ. Identification of CYP3A4 as the principal enzyme catalyzing mifepristone (RU 486) oxidation in human liver microsomes. Biochem Pharmacol 1996; 52(5): 753–61
Stupans I, Murray M, Kirlich A, et al. Inactivation of cytochrome P450 by the food-derived complex phenol oleuropein. Food Chem Toxicol 2001; 39(11): 1119–24
Tran TH, Von Moltke LL, Venkatakrishnan K, et al. Microsomal protein concentration modifies the apparent inhibitory potency of CYP3A inhibitors. Drug Metab Dispos 2002; 30(12): 1441–5
Zdravkovic M, Olsen AK, Christiansen T, et al. A clinical study investigating the pharmacokinetic interaction between NN703 (tabimorelin), a potential inhibitor of CYP3A4 activity, and midazolam, a CYP3A4 substrate. Eur J Clin Pharmacol 2003; 58(10): 683–8
Williams JA, Ring BJ, Cantrell VE, et al. Comparative metabolic capabilities of CYP3A4, CYP3A5, and CYP3A7. Drug Metab Dispos 2002; 30(8): 883–91
Kroemer HK, Echizen H, Heidemann H, et al. Predictability of the in vivo metabolism of verapamil from in vitro data: contribution of individual metabolic pathways and stereoselective aspects. J Pharmacol Exp Ther 1992; 260(3): 1052–7
Brodie MJ, Macphee GJA. Carbamazepine neurotoxicity precipitated by diltiazem. BMJ (Clin Red Ed) 1986; 292: 1170–1
Sadrieh N, Thomas PE. Characterization of rat cytochrome P450 isozymes involved in the covalent binding of cyclosporin A to microsomal proteins. Toxicol Appl Pharmacol 1994; 127(2): 222–32
Brockmöller J, Neumayer H-H, Wagner K, et al. Pharmacokinetic interaction between cyclosporin and diltiazem. Eur J Clin Pharmacol 1990; 38(3): 237–42
Laganière S, Davies RF, Carignan G, et al. Pharmacokinetic and pharmacodynamic interactions between diltiazem and quinidine. Clin Pharmacol Ther 1996; 60(3): 255–64
Backman JT, Olkkola KT, Aranko K, et al. Dose of midazolam should be reduced during diltiazem and verapamil treatments. Br J Clin Pharmacol 1994; 37(3): 221–5
Toyosaki N, Toyo-Oka T, Natsume T, et al. Combination therapy with diltiazem and nifedipine in patients with effort angina pectoris. Circulation 1988; 77: 1370–5
Azie NE, Brater DC, Becker PA, et al. The interaction of diltiazem with lovastatin and pravastatin. Clin Pharmacol Ther 1998; 64(4): 369–77
Cato III A, Cavanaugh J, Shi H, et al. The effect of multiple doses of ritonavir on the pharmacokinetics of rifabutin. Clin Pharmacol Ther 1998; 63(4): 414–21
Ouellet D, Hsu A, Granneman GR, et al. Pharmacokinetic interaction between ritonavir and clarithromycin. Clin Pharmacol Ther 1998; 64(4): 355–62
Hsu A, Granneman GR, Cao G, et al. Pharmacokinetic interactions between two human immunodeficiency virus protease inhibitors, ritonavir and saquinavir. Clin Pharmacol Ther 1998; 63(4): 453–64
Sadler BM, Piliero PJ, Preston SL, et al. Pharmacokinetics and safety of amprenavir and ritonavir following multiple-dose, co-administration to healthy volunteers. AIDS 2001; 15(8): 1009–18
Goujard C, Vincent I, Meynard JL, et al. Steady-state pharmacokinetics of amprenavir coadministered with ritonavir in human immunodeficiency virus type 1-infected patients. Antimicrob Agents Chemother 2003; 47(1): 118–23
Kurowski M, Kaeser B, Sawyer A, et al. Low-dose ritonavir moderately enhances nelfinavir exposure. Clin Pharmacol Ther 2002; 72(2): 123–32
Sham HL, Kempf DJ, Molla A, et al. ABT-378, a highly potent inhibitor of the human immunodeficiency virus protease. Antimicrob Agents Chemother 1998; 42(12): 3218–24
Hsu A, Granneman GR, Cao G, et al. Pharmacokinetic interaction between ritonavir and indinavir in healthy volunteers. Antimicrob Agents Chemother 1998; 42(11): 2784–91
Yasui N, Otani K, Kaneko S, et al. Carbamazepine toxicity induced by clarithromycin coadministration in psychiatric patients. Int Clin Psychopharmacol 1997; 12(4): 225–9
van Haarst AD, van’t Klooster GA, van Gerven JM, et al. The influence of cisapride and clarithromycin on QT intervals in healthy volunteers. Clin Pharmacol Ther 1998; 64(5): 542–6
Sadaba B, Lopez de Ocariz A, Azanza JR, et al. Concurrent clarithromycin and cyclosporin A treatment. J Antimicrob Chemother 1998; 42(3): 393–5
Boruchoff SE, Sturgill MG, Grasing KW, et al. The steady-state disposition of indinavir is not altered by the concomitant administration of clarithromycin. Clin Pharmacol Ther 2000; 67(4): 351–9
Ushiama H, Echizen H, Nachi S, et al. Dose-dependent inhibition of CYP3A activity by clarithromycin during Helicobacter pylori eradication therapy assessed by changes in plasma lansoprazole levels and partial cortisol clearance to 6beta-hydroxycortisol. Clin Pharmacol Ther 2002; 72(1): 33–43
Fost DA, Leung DY, Martin RJ, et al. Inhibition of methyl-prednisolone elimination in the presence of clarithromycin therapy. J Allergy Clin Immunol 1999; 103(6): 1031–5
Hafner R, Bethel J, Power M, et al. Tolerance and pharmacokinetic interactions of rifabutin and clarithromycin in human immunodeficiency virus-infected volunteers. Antimicrob Agents Chemother 1998; 42(3): 631–9
Luurila H, Olkkola KT, Neuvonen PJ. Interaction between erythromycin and the benzodiazepines diazepam and flunitrazepam. Pharmacol Toxicol 1996; 78(2): 117–22
Kantola T, Kivisto KT, Neuvonen PJ. Erythromycin and verapamil considerably increase serum simvastatin and simvastatin acid concentrations. Clin Pharmacol Ther 1998; 64(2): 177–82
Isohanni MH, Neuvonen PJ, Palkama VJ, et al. Effect of erythromycin and itraconazole on the pharmacokinetics of intravenous lignocaine. Eur J Clin Pharmacol 1998; 54(7): 561–5
Olkkola KT, Aranko K, Luurila H, et al. A potentially hazardous interaction between erythromycin and midazolam. Clin Pharmacol Ther 1993; 53(3): 298–305
Luurila H, Olkkola KT, Neuvonen PJ. Interaction between erythromycin and nitrazepam in healthy volunteers. Pharmacol Toxicol 1995; 76(4): 255–8
Lamberg TS, Kivistö KT, Neuvonen PJ. Effects of verapamil and diltiazem on the pharmacokinetics and pharmacodynamics of buspirone. Clin Pharmacol Ther 1998; 63(6): 640–5
Booker BM, Magee MH, Blum RA, et al. Pharmacokinetic and pharmacodynamic interactions between diltiazem and methyl-prednisolone in healthy volunteers. Clin Pharmacol Ther 2002; 72(4): 370–82
Dresser GK, Spence JD, Bailey DG. Pharmacokinetic-pharmacodynamic consequences and clinical relevance of cytochrome P450 3A4 inhibition. Clin Pharmacokinet 2000; 38(1): 41–57
Spinler SA, Cheng JW, Kindwall KE, et al. Possible inhibition of hepatic metabolism of quinidine by erythromycin. Clin Pharmacol Ther 1995; 57(1): 89–94
Michalets EL, Williams CR. Drug interactions with cisapride: clinical implications. Clin Pharmacokinet 2000; 39(1): 49–75
Honig PK, Woosley RL, Zamani K, et al. Changes in the pharmacokinetics and electrocardiographic pharmacodynamics of terfenadine with concomitant administration of erythromycin. Clin Pharmacol Ther 1992; 52(3): 231–8
Honig PK, Wortham DC, Zamani K, et al. Terfenadine-ketoconazole interaction: pharmacokinetic and electrocardiographic consequences. JAMA 1993; 269: 1513–8
Williams D, Feely J. Pharmacokinetic-pharmacodynamic drug interactions with HMG-CoA reductase inhibitors. Clin Pharmacokinet 2002; 41(5): 343–70
Anderson JR, Nawarskas JJ. Cardiovascular drug-drug interactions. Cardiol Clin 2001; 19(2): 215–34
Simonsen U. Interactions between drugs for erectile dysfunction and drugs for cardiovascular disease. Int J Impot Res 2002; 14(3): 178–88
Patsalos PN, Froscher W, Pisani F, et al. The importance of drug interactions in epilepsy therapy. Epilepsia 2002; 43(4): 365–85
Spina E, Pisani F, Perucca E. Clinically significant pharmacokinetic drug interactions with carbamazepine: an update. Clin Pharmacokinet 1996; 31(3): 198–214
Rathbun RC, Rossi DR. Low-dose ritonavir for protease inhibitor pharmacokinetic enhancement. Ann Pharmacother 2002; 36(4): 702–6
Kempf DJ, Marsh KC, Kumar G, et al. Pharmacokinetic enhancement of inhibitors of the human immunodeficiency virus protease by coadministration with ritonavir. Antimicrob Agents Chemother 1997; 41(3): 654–60
Chitturi S, George J. Hepatotoxicity of commonly used drugs: nonsteroidal anti-inflammatory drugs, antihypertensives, antidiabetic agents, anticonvulsants, lipid-lowering agents, psychotropic drugs. Semin Liver Dis 2002; 22(2): 169–83
Pumford NR, Halmes NC. Protein targets of xenobiotic reactive intermediates. Annu Rev Pharmacol Toxicol 1997; 37: 91–117
Tornqvist M, Fred C, Haglund J, et al. Protein adducts: quantitative and qualitative aspects of their formation, analysis and applications. J Chromatogr B Analyt Technol Biomed Life Sci 2002 Oct 5; 778(1–2): 279–308
Cohen SD, Pumford NR, Khairallah EA, et al. Selective protein covalent binding and target organ toxicity. Toxicol Appl Pharmacol 1997; 143(1): 1–12
Houston JB. Utility of in vitro drug metabolism data in predicting in vivo metabolic clearance. Biochem Pharmacol 1994; 47: 1469–79
Houston JB, Carlile DJ. Incorporation of in vitro drug metabolism data into physiologically-based pharmacokinetic models. Toxicol In Vitro 1997; 11: 473–8
von Moltke LL, Greenblatt DJ, Schmider J, et al. In vitro approaches to predicting drug interactions in vivo. Biochem Pharmacol 1998; 55: 113–22
Lave T, Coassolo P, Reigner B. Prediction of hepatic metabolic clearance based on interspecies allometric scaling techniques and in vitro in vivo correlations. Clin Pharmacokinet 1999; 36(3): 211–31
Tsao S-C, Dickinson TH, Abernethy DR. Metabolite inhibition of parent drug biotransformation: studies of diltiazem. Drug Metab Dispos 1990; 18: 180–2
Mullins ME, Horowitz Z, Linden DHJ, et al. Life-threatening interaction of mibefradil and β-blockers with dihydropyridine calcium channel blockers. JAMA 1998; 280(2): 157–8
Ito K, Iwatsubo T, Kanamitsu S, et al. Quantitative prediction of in vivo drug clearance and drug interactions from in vitro data on metabolism, together with binding and transport. Annu Rev Pharmacol Toxicol 1998; 38: 461–99
Waley SG. Kinetics of suicide substrates. Biochem J 1980; 185: 771–3
Waley SG. Kinetics of suicide substrates. Practical procedures for determining parameters. Biochem J 1985; 227: 843–9
Tatsunami S, Yago N, Hosoe M. Kinetics of suicide substrates: steady-state treatments and computer-aided exact solutions. Biochim Biophys Acta 1981; 662(2): 226–35
Ring BJ, Binkley SN, Roskos L, et al. Effect of fluoxetine, norfluoxetine, sertraline and desmethyl sertraline on human CYP3A catalyzed 1′-hydroxy midazolam formation in vitro. J Pharmacol Exp Ther 1995; 275(3): 1131–5
Sugiyama Y, Kato Y, Chu X. Multiplicity of biliary excretion mechanisms for the camptothecin derivative irinotecan (CPT-11), its metabolite SN-38, and its glucuronide: role of canalicular multispecific organic anion transporter and P-glycoprotein. Cancer Chemother Pharmacol 1998; 42 Suppl.: S44–9
Chu XY, Suzuki H, Ueda K, et al. Active efflux of CPT-11 and its metabolites in human KB-derived cell lines. J Pharmacol Exp Ther 1999; 288(2): 735–41
Chu XY, Kato Y, Ueda K, et al. Biliary excretion mechanism of CPT-11 and its metabolites in humans: involvement of primary active transporters. Cancer Res 1998; 58(22): 5137–43
Chu XY, Kato Y, Niinuma K, et al. Multispecific organic anion transporter is responsible for the biliary excretion of the camptothecin derivative irinotecan and its metabolites in rats. J Pharmacol Exp Ther 1997; 281(1): 304–14
Olson DP, Scadden DT, D’Aquila RT, et al. The protease inhibitor ritonavir inhibits the functional activity of the multidrug resistance related-protein 1 (MRP-1). AIDS 2002; 16(13): 1743–7
Gruol DJ, Zee MC, Trotter J, et al. Reversal of multidrug resistance by RU486. Cancer Res 1994; 54: 3088–91
Ambudkar SV, Dey S, Hrycyna CA, et al. Biochemical, cellular, and pharmacological aspects of the multidrug transporter. Annu Rev Pharmacol Toxicol 1999; 39: 361–98
Lin JH, Yamazaki M. Role of P-glycoprotein in pharmacokinetics: clinical implications. Clin Pharmacokinet 2003; 41(1): 59–98
Lecureur V, Fardel O, Guilouzo A. The antiprogestin drug RU486 potentiates doxorubicin cytotoxicity in multidrug resistant cells through inhibition of P-glycoprotein function. FEBS Lett 1994; 355(2): 187–91
Huang LY, Wring S, Woolley JL, et al. Induction of P-glycoprotein and cytochrome P450 3A by HIV protease inhibitors. Drug Metab Dispos 2001; 29(5): 754–60
Wacher VJ, Wu C-Y, Benet LZ. Overlapping substrate specificities and tissue distribution of cytochrome P450 3A and P-glycoprotein: implications for drug delivery and activity in cancer chemotherapy. Mol Carcinog 1995; 13: 129–34
Schuetz EG, Beck WT, Schuetz JD. Modulators and substrates of P-glycoprotein and cytochrome P4503A coordinately upregulate these proteins in human colon carcinoma cells. Mol Pharmacol 1996; 49: 311–8
Watkins PB. Noninvasive tests of CYP3A enzymes. Pharmacogenetics 1994; 4(4): 171–84
Pascussi JM, Gerbal-Chaloin S, Pichard-Garcia L, et al. Interleukin-6 negatively regulates the expression of pregnane X receptor and constitutively activated receptor in primary human hepatocytes. Biochem Biophys Res Commun 2000; 274(3): 707–13
Hunt CM, Westerkam WR, Stave GM. Effect of age and gender on the activity of human hepatic CYP3A. Biochem Pharmacol 1992; 44(2): 275–83
Schmucker DL. Liver function and phase I drug metabolism in the elderly: a paradox. Drugs Aging 2001; 18(11): 837–51
Meibohm B, Beierle I, Derendorf H. How important are gender differences in pharmacokinetics? Clin Pharmacokinet 2002; 41(5): 329–42
Hartmann G, Cheung AK, Piquette-Miller M. Inflammatory cytokines, but not bile acids, regulate expression of murine hepatic anion transporters in endotoxemia. J Pharmacol Exp Ther 2002; 303(1): 273–81
Chen YZ, Ung CY. Prediction of potential toxicity and side effect protein targets of a small molecule by a ligand-protein inverse docking approach. J Mol Graph Model 2001; 20(3): 199–218
Acknowledgements
The authors appreciate support by the National University of Singapore Academic Research Funds. The authors have no potential conflicts of interest that are directly relevant to the content of this review.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Zhou, S., Chan, S.Y., Goh, B.C. et al. Mechanism-Based Inhibition of Cytochrome P450 3A4 by Therapeutic Drugs. Clin Pharmacokinet 44, 279–304 (2005). https://doi.org/10.2165/00003088-200544030-00005
Published:
Issue Date:
DOI: https://doi.org/10.2165/00003088-200544030-00005