





Abstract
Despite a well-described symptomatology, treatment delay and sequelae are common in patients with Lyme neuroborreliosis (LNB). The aim of this study was to contribute to the knowledge about the symptomatology and epidemiology of LNB.
We conducted a retrospective study of all LNB cases verified by a positive Borrelia intrathecal antibody index test performed at the Department of Microbiology, Odense University Hospital, Denmark, from 1995 through 2014.
The study included 431 patients; 126 were children. The mean incidence was 4.7 per 100 000 inhabitants per year. The median delay from neurological symptom debut to first hospital contact was 20 days and significantly longer for patients with symptom debut in the winter/early spring. The most common clinical symptoms were painful radiculitis (65.9%), cranial nerve palsy (43.4%), and headache (28.3%). A total of 30.6% were seen in >1 hospital department, and 85.6% were admitted during their course of treatment. Serum Borrelia immunoglobulin M and immunoglobulin G at the time of positive Borrelia intrathecal antibody index test were negative in 67 patients (15.5%). We found a median treatment delay of 24 days, with no improvement in our 20-year study period. Residual symptoms following treatment were found in 28.1% of patients, and risk of residual symptoms was significantly associated with delay from symptom debut to initiation of treatment.
The association between treatment delay and residual symptoms and the lack of improvement in treatment delay during the study period highlight the need for standardized diagnostic routines and a better follow-up for LNB patients. Our findings disprove that all patients with LNB develop positive serum Borrelia antibodies within 6 weeks after infection.
Since Garin and Bujadoux first described paralysis after a tick bite in 1922 [1], our understanding of Lyme neuroborreliosis (LNB) has been widened considerably. The culprit, the spirochete Borrelia burgdorferi, was discovered in 1982 [2], and we now know of at least 5 different genospecies that cause disease in humans: Borrelia afzelii, Borrelia garinii, B. burgdorferi sensu stricto, Borrelia spielmanii, and Borrelia bavariensis [3].
LNB is seen in 3%–15% of patients with borreliosis [3–5]. The symptoms generally debut 4–6 weeks after a tick bite. The most common manifestations are meningoradiculitis, lymphocytic meningitis, and cranial nerve palsy [3–8]. The LNB diagnosis is based on the combination of neurological symptoms; cerebrospinal fluid (CSF) findings, typically with lymphocytic pleocytosis and elevated protein levels; and an antibody index (CSF-Borrelia AI) calculation comparing the B. burgdorferi–specific antibodies in the CSF and serum [8–11].
LNB is treated with intravenous penicillin, intravenous ceftriaxone, or oral doxycycline for 14–21 days [8, 12, 13]. Even with the recommended treatment, 12%–59% of LNB patients report residual symptoms months to years after treatment [7, 8, 13–16]. The risk of persisting residual symptoms has been related to the length of time from onset of symptoms to antibiotic treatment [7, 14, 17].
In Europe, the incidence of LNB has been stable in known endemic regions, with some yearly variation [3, 18, 19]. The yearly incidence rates are 0.9–3.2 per 100000 inhabitants in Denmark [6, 14, 20]. The islands of Funen and Langeland are known for their LNB endemicity [6, 20].
The aim of this retrospective study was to characterize the symptomatology and epidemiology of LNB on the Danish islands of Funen and Langeland from 1995 through 2014.
METHODS
Study Population and Design
Our data cover the islands of Funen and Langeland, with a total population of 449551 on 1 January 1995, and 472067 as of 1 January 2015 [21]. The Department of Clinical Microbiology at Odense University Hospital serves all residents. All microbiological results are recorded in an electronic laboratory system from which eligible patients were identified. Patients with a positive CSF-Borrelia AI (immunoglobulin M [IgM] and/or immunoglobulin G [IgG]) in the period 1 January 1995 to 1 January 2015 were candidates for the study. Patient charts were retrieved through electronic or paper records from hospital archives.
Clinical Data
For each patient, the following parameters were extracted from the charts: date of birth, sex, occupation, comorbidities (using Charlson comorbidity index) [22], risk factors for tick bites, history of tick bites, debut of neurological symptoms, first hospital contact after debut of symptoms, clinical symptoms, use of pain medication, temperature at first contact, admission, antibiotic treatment (start, length, and effect), residual symptoms after treatment, treating hospital departments, and first-year mortality.
Definitions
Patient delay was defined as the number of days from onset of neurological symptoms to first hospital contact, hospital delay as the number of days from first hospital contact with LNB symptoms to initiation of antimicrobial therapy, and treatment delay as the summarized patient delay and hospital delay.
Paraclinical Data
From the blood tests we registered hemoglobin, leukocytes, neutrophils, lymphocytes, thrombocytes, C-reactive protein, and Borrelia-specific IgG and IgM antibodies in serum (S-Borrelia IgM/IgG). From CSF, we registered leukocyte count including percentage of mononuclear cells, protein, glucose, and Borrelia IgM/IgG AI.
Cerebrospinal Fluid Borrelia AI
The second-generation IDEIA LNB test (Oxoid, Hampshire, United Kingdom) was used for detection of intrathecal synthesis of Borrelia-specific antibodies throughout the study period [23, 24]. For details about the Borrelia antibody assays used, see the Supplementary Materials.
Borrelia-Specific Antibodies in Serum
For the detection of S-Borrelia IgG/IgM, we used IDEIA B. burgdorferi IgG and IgM (Oxoid) between 1995 and 2010 [25, 26], and Enzygnost Lyme link variable lipoprotein surface-exposed protein (VlsE)/IgG and Enzygnost Borreliosis/IgM (Siemens, Marburg, Germany) from 2011 (Supplementary Materials) [27, 28].
Statistical Analysis
The database was created using FileMakerPro 13.0. Statistical analyses were carried out using Stata version 12.1 software. To test the significance between groups, Pearson χ2, t test, or F-test (for normally distributed data), and Wilcoxon-Mann-Whitney and Kruskal-Wallis test (for nonnormally distributed data) were performed. A P value <.05 was considered statistically significant.
Ethical Considerations
The study was approved by the Danish Data Protection Agency (j.nr.2008-58-0035) and the Danish Health and Medicines Authority (j.nr.3-3013-631/1/).
RESULTS
In total, 442 patients were found to have a positive CSF-Borrelia AI IgM and/or IgG. Eleven patients were excluded due to missing records; therefore, 431 patients were included in the study.
Incidence
There was a large yearly variation in number of patients, ranging from 10 patients in 1996 and 1998 to 40 patients in 2006, a mean of 21.6 patients per year. This gives a mean incidence of 4.7 per 100000 inhabitants.
Patient Characteristics
Patient characteristics are shown in Table 1. The median age was 47 years (interquartile range [IQR], 50[12–62] years), 60.8% were male, and 126 were children <18 years. The majority had no comorbidities, 36.9% had a history of tick bite registered, and 19.5% had a history of erythema migrans.
Characteristics of 431 Patients With Lyme Neuroborreliosis
| Characteristic | No. (%) |
|---|---|
| Age, y, median (IQR) | 47 (12–62) |
| Children <18 y | 126 (29.2) |
| Sex, male | 262 (60.8) |
| Charlson comorbidity score | |
| 0 | 372 (86.3) |
| 1–2 | 53 (12.3) |
| ≥3 | 6 (1.4) |
| Exposition | |
| Hiker | 67 (15.5) |
| Garden next to forest | 41 (9.5) |
| Occupation farmer/forester | 10 (2.3) |
| Hunter | 7 (1.6) |
| No known exposition | 287 (66.6) |
| History of tick bite | 159 (36.9) |
| Tick bite location (n = 67) | |
| Trunk | 25 |
| Lower extremities | 23 |
| Head/neck | 14 |
| Upper extremities | 5 |
| History of EM | 84 (19.5) |
| Location of EM (n = 77) | |
| Trunk | 29 |
| Lower extremities | 27 |
| Head/neck | 14 |
| Upper extremities | 7 |
| Coinciding location of tick bite and EM | 12/15 (80) |
| 1-y mortality | 2 (0.46) |
| Characteristic | No. (%) |
|---|---|
| Age, y, median (IQR) | 47 (12–62) |
| Children <18 y | 126 (29.2) |
| Sex, male | 262 (60.8) |
| Charlson comorbidity score | |
| 0 | 372 (86.3) |
| 1–2 | 53 (12.3) |
| ≥3 | 6 (1.4) |
| Exposition | |
| Hiker | 67 (15.5) |
| Garden next to forest | 41 (9.5) |
| Occupation farmer/forester | 10 (2.3) |
| Hunter | 7 (1.6) |
| No known exposition | 287 (66.6) |
| History of tick bite | 159 (36.9) |
| Tick bite location (n = 67) | |
| Trunk | 25 |
| Lower extremities | 23 |
| Head/neck | 14 |
| Upper extremities | 5 |
| History of EM | 84 (19.5) |
| Location of EM (n = 77) | |
| Trunk | 29 |
| Lower extremities | 27 |
| Head/neck | 14 |
| Upper extremities | 7 |
| Coinciding location of tick bite and EM | 12/15 (80) |
| 1-y mortality | 2 (0.46) |
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: EM, erythema migrans, IQR, interquartile range.
Characteristics of 431 Patients With Lyme Neuroborreliosis
| Characteristic | No. (%) |
|---|---|
| Age, y, median (IQR) | 47 (12–62) |
| Children <18 y | 126 (29.2) |
| Sex, male | 262 (60.8) |
| Charlson comorbidity score | |
| 0 | 372 (86.3) |
| 1–2 | 53 (12.3) |
| ≥3 | 6 (1.4) |
| Exposition | |
| Hiker | 67 (15.5) |
| Garden next to forest | 41 (9.5) |
| Occupation farmer/forester | 10 (2.3) |
| Hunter | 7 (1.6) |
| No known exposition | 287 (66.6) |
| History of tick bite | 159 (36.9) |
| Tick bite location (n = 67) | |
| Trunk | 25 |
| Lower extremities | 23 |
| Head/neck | 14 |
| Upper extremities | 5 |
| History of EM | 84 (19.5) |
| Location of EM (n = 77) | |
| Trunk | 29 |
| Lower extremities | 27 |
| Head/neck | 14 |
| Upper extremities | 7 |
| Coinciding location of tick bite and EM | 12/15 (80) |
| 1-y mortality | 2 (0.46) |
| Characteristic | No. (%) |
|---|---|
| Age, y, median (IQR) | 47 (12–62) |
| Children <18 y | 126 (29.2) |
| Sex, male | 262 (60.8) |
| Charlson comorbidity score | |
| 0 | 372 (86.3) |
| 1–2 | 53 (12.3) |
| ≥3 | 6 (1.4) |
| Exposition | |
| Hiker | 67 (15.5) |
| Garden next to forest | 41 (9.5) |
| Occupation farmer/forester | 10 (2.3) |
| Hunter | 7 (1.6) |
| No known exposition | 287 (66.6) |
| History of tick bite | 159 (36.9) |
| Tick bite location (n = 67) | |
| Trunk | 25 |
| Lower extremities | 23 |
| Head/neck | 14 |
| Upper extremities | 5 |
| History of EM | 84 (19.5) |
| Location of EM (n = 77) | |
| Trunk | 29 |
| Lower extremities | 27 |
| Head/neck | 14 |
| Upper extremities | 7 |
| Coinciding location of tick bite and EM | 12/15 (80) |
| 1-y mortality | 2 (0.46) |
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: EM, erythema migrans, IQR, interquartile range.
Symptoms
Radicular pain and facial nerve palsy were the dominant symptoms, and 74.7% had >1 symptom (Table 2). Compared to adults, children had a significantly higher proportion of cranial nerve palsy (54.7% vs 38.7%; P < .01), headache (40.5% vs 23.3%; P < .001), meningitis (13.5% vs 1.3%; P < .001), and intermittent fever (38.9% vs 18.0%; P < .001), and less radicular pain (38.1% vs 77.4%; P < .001) and peripheral nerve palsy (2.4% vs 10.2%; P < .01).
Symptoms Among 431 Patients With Lyme Neuroborreliosis
| Symptom | No. of Patients (%) |
|---|---|
| Radicular pain | 284 (65.9) |
| Cranial nerve palsy | 187 (43.4) |
| Nervus facialis | 178 |
| Nervus abducens | 8 |
| Nervus oculomotorius | 4 |
| Nervus trochlearis | 2 |
| Nervus trigeminus | 2 |
| Nervus hypoglossus | 2 |
| Nervus olfactorius | 1 |
| Nervus vestibulocochlearis | 1 |
| Headache | 122 (28.3) |
| Intermittent fever | 104 (24.1) |
| Analgesic-resistant pain | 92 (21.3) |
| Morphine-resistant pain | 16 |
| NSAID-resistant pain | 42 |
| Morphine- and NSAID-resistant pain | 34 |
| Fatigue | 65 (15.1) |
| Temperature of ≥38.0°C at first hospital contacta | 34 (13.0) |
| Peripheral nerve palsy | 34 (7.9) |
| Dizziness | 30 (7.0) |
| Weight loss | 23 (5.3) |
| Meningitis | 21 (4.9) |
| Encephalitis | 16 (3.7) |
| Arthritis | 15 (3.5) |
| Memory impairment | 6 (1.4) |
| Lymphadenopathy | 6 (1.4) |
| Acrodermatitis chronicum atrophicans | 4 (0.9) |
| Arthralgias/myalgias | 3 (0.7) |
| Eye symptomsb | 2 (0.5) |
| Concentration difficulties | 2 (0.5) |
| Abdominal pain | 2 (0.5) |
| Bladder paresis | 2 (0.5) |
| Symptom | No. of Patients (%) |
|---|---|
| Radicular pain | 284 (65.9) |
| Cranial nerve palsy | 187 (43.4) |
| Nervus facialis | 178 |
| Nervus abducens | 8 |
| Nervus oculomotorius | 4 |
| Nervus trochlearis | 2 |
| Nervus trigeminus | 2 |
| Nervus hypoglossus | 2 |
| Nervus olfactorius | 1 |
| Nervus vestibulocochlearis | 1 |
| Headache | 122 (28.3) |
| Intermittent fever | 104 (24.1) |
| Analgesic-resistant pain | 92 (21.3) |
| Morphine-resistant pain | 16 |
| NSAID-resistant pain | 42 |
| Morphine- and NSAID-resistant pain | 34 |
| Fatigue | 65 (15.1) |
| Temperature of ≥38.0°C at first hospital contacta | 34 (13.0) |
| Peripheral nerve palsy | 34 (7.9) |
| Dizziness | 30 (7.0) |
| Weight loss | 23 (5.3) |
| Meningitis | 21 (4.9) |
| Encephalitis | 16 (3.7) |
| Arthritis | 15 (3.5) |
| Memory impairment | 6 (1.4) |
| Lymphadenopathy | 6 (1.4) |
| Acrodermatitis chronicum atrophicans | 4 (0.9) |
| Arthralgias/myalgias | 3 (0.7) |
| Eye symptomsb | 2 (0.5) |
| Concentration difficulties | 2 (0.5) |
| Abdominal pain | 2 (0.5) |
| Bladder paresis | 2 (0.5) |
Data are presented as No. (%).
Abbreviation: NSAID, nonsteroidal anti-inflammatory drug.
aOf 262 patients with registered temperature at first hospital contact.
bOne patient with nystagmus, 1 patient with impaired vision.
Symptoms Among 431 Patients With Lyme Neuroborreliosis
| Symptom | No. of Patients (%) |
|---|---|
| Radicular pain | 284 (65.9) |
| Cranial nerve palsy | 187 (43.4) |
| Nervus facialis | 178 |
| Nervus abducens | 8 |
| Nervus oculomotorius | 4 |
| Nervus trochlearis | 2 |
| Nervus trigeminus | 2 |
| Nervus hypoglossus | 2 |
| Nervus olfactorius | 1 |
| Nervus vestibulocochlearis | 1 |
| Headache | 122 (28.3) |
| Intermittent fever | 104 (24.1) |
| Analgesic-resistant pain | 92 (21.3) |
| Morphine-resistant pain | 16 |
| NSAID-resistant pain | 42 |
| Morphine- and NSAID-resistant pain | 34 |
| Fatigue | 65 (15.1) |
| Temperature of ≥38.0°C at first hospital contacta | 34 (13.0) |
| Peripheral nerve palsy | 34 (7.9) |
| Dizziness | 30 (7.0) |
| Weight loss | 23 (5.3) |
| Meningitis | 21 (4.9) |
| Encephalitis | 16 (3.7) |
| Arthritis | 15 (3.5) |
| Memory impairment | 6 (1.4) |
| Lymphadenopathy | 6 (1.4) |
| Acrodermatitis chronicum atrophicans | 4 (0.9) |
| Arthralgias/myalgias | 3 (0.7) |
| Eye symptomsb | 2 (0.5) |
| Concentration difficulties | 2 (0.5) |
| Abdominal pain | 2 (0.5) |
| Bladder paresis | 2 (0.5) |
| Symptom | No. of Patients (%) |
|---|---|
| Radicular pain | 284 (65.9) |
| Cranial nerve palsy | 187 (43.4) |
| Nervus facialis | 178 |
| Nervus abducens | 8 |
| Nervus oculomotorius | 4 |
| Nervus trochlearis | 2 |
| Nervus trigeminus | 2 |
| Nervus hypoglossus | 2 |
| Nervus olfactorius | 1 |
| Nervus vestibulocochlearis | 1 |
| Headache | 122 (28.3) |
| Intermittent fever | 104 (24.1) |
| Analgesic-resistant pain | 92 (21.3) |
| Morphine-resistant pain | 16 |
| NSAID-resistant pain | 42 |
| Morphine- and NSAID-resistant pain | 34 |
| Fatigue | 65 (15.1) |
| Temperature of ≥38.0°C at first hospital contacta | 34 (13.0) |
| Peripheral nerve palsy | 34 (7.9) |
| Dizziness | 30 (7.0) |
| Weight loss | 23 (5.3) |
| Meningitis | 21 (4.9) |
| Encephalitis | 16 (3.7) |
| Arthritis | 15 (3.5) |
| Memory impairment | 6 (1.4) |
| Lymphadenopathy | 6 (1.4) |
| Acrodermatitis chronicum atrophicans | 4 (0.9) |
| Arthralgias/myalgias | 3 (0.7) |
| Eye symptomsb | 2 (0.5) |
| Concentration difficulties | 2 (0.5) |
| Abdominal pain | 2 (0.5) |
| Bladder paresis | 2 (0.5) |
Data are presented as No. (%).
Abbreviation: NSAID, nonsteroidal anti-inflammatory drug.
aOf 262 patients with registered temperature at first hospital contact.
bOne patient with nystagmus, 1 patient with impaired vision.
Paraclinical Findings
The mean CSF leukocyte count was 113 × 106/L, and the mean CSF protein and CSF glucose were 0.9 g/L and 3.0 mmol/L, respectively (Table 3). In 5 patients, the CSF leukocyte count was not available. The majority of patients did not have elevated inflammatory markers in peripheral blood.
Results from Cerebrospinal Fluid and Peripheral Blood Among 431 Patients With Lyme Neuroborreliosis
| Laboratory Result | No. (%) of Patients With Registered Result | Mean | Range | 25th, 75th Percentile | Reference Interval | No. (%) of Patients Above Normal Range |
|---|---|---|---|---|---|---|
| CSF leukocytes, ×106/L | 425 (98.6) | 113 | 0–7850 | 29, 288 | 0–5 | 383 (90.1) |
| CSF mononuclear, % of leukocytes | 294 (68.2) | 98 | 0.00–1.00 | 0.95, 1.00 | … | … |
| CSF protein, g/L | 407 (94.4) | 0.9 | 0.1–9.6 | 0.5, 1.5 | 0.40–0.70 | 234 (57.5) |
| CSF glucose, mmol/L | 408 (94.7) | 3.0 | 0.6–9.3 | 2.7, 3.4 | … | … |
| CRP, mg/L | 389 (90.3) | <10 | 0–161 | <10, <10 | <10 | 37 (9.5) |
| B-leukocytes, ×109/L | 401 (93.0) | 7.4 | 3.1–35.0 | 6.0, 9.0 | 3.50–8.80 | 110 (27.4) |
| Laboratory Result | No. (%) of Patients With Registered Result | Mean | Range | 25th, 75th Percentile | Reference Interval | No. (%) of Patients Above Normal Range |
|---|---|---|---|---|---|---|
| CSF leukocytes, ×106/L | 425 (98.6) | 113 | 0–7850 | 29, 288 | 0–5 | 383 (90.1) |
| CSF mononuclear, % of leukocytes | 294 (68.2) | 98 | 0.00–1.00 | 0.95, 1.00 | … | … |
| CSF protein, g/L | 407 (94.4) | 0.9 | 0.1–9.6 | 0.5, 1.5 | 0.40–0.70 | 234 (57.5) |
| CSF glucose, mmol/L | 408 (94.7) | 3.0 | 0.6–9.3 | 2.7, 3.4 | … | … |
| CRP, mg/L | 389 (90.3) | <10 | 0–161 | <10, <10 | <10 | 37 (9.5) |
| B-leukocytes, ×109/L | 401 (93.0) | 7.4 | 3.1–35.0 | 6.0, 9.0 | 3.50–8.80 | 110 (27.4) |
Abbreviations: CRP, C-reactive protein; CSF, cerebrospinal fluid.
Results from Cerebrospinal Fluid and Peripheral Blood Among 431 Patients With Lyme Neuroborreliosis
| Laboratory Result | No. (%) of Patients With Registered Result | Mean | Range | 25th, 75th Percentile | Reference Interval | No. (%) of Patients Above Normal Range |
|---|---|---|---|---|---|---|
| CSF leukocytes, ×106/L | 425 (98.6) | 113 | 0–7850 | 29, 288 | 0–5 | 383 (90.1) |
| CSF mononuclear, % of leukocytes | 294 (68.2) | 98 | 0.00–1.00 | 0.95, 1.00 | … | … |
| CSF protein, g/L | 407 (94.4) | 0.9 | 0.1–9.6 | 0.5, 1.5 | 0.40–0.70 | 234 (57.5) |
| CSF glucose, mmol/L | 408 (94.7) | 3.0 | 0.6–9.3 | 2.7, 3.4 | … | … |
| CRP, mg/L | 389 (90.3) | <10 | 0–161 | <10, <10 | <10 | 37 (9.5) |
| B-leukocytes, ×109/L | 401 (93.0) | 7.4 | 3.1–35.0 | 6.0, 9.0 | 3.50–8.80 | 110 (27.4) |
| Laboratory Result | No. (%) of Patients With Registered Result | Mean | Range | 25th, 75th Percentile | Reference Interval | No. (%) of Patients Above Normal Range |
|---|---|---|---|---|---|---|
| CSF leukocytes, ×106/L | 425 (98.6) | 113 | 0–7850 | 29, 288 | 0–5 | 383 (90.1) |
| CSF mononuclear, % of leukocytes | 294 (68.2) | 98 | 0.00–1.00 | 0.95, 1.00 | … | … |
| CSF protein, g/L | 407 (94.4) | 0.9 | 0.1–9.6 | 0.5, 1.5 | 0.40–0.70 | 234 (57.5) |
| CSF glucose, mmol/L | 408 (94.7) | 3.0 | 0.6–9.3 | 2.7, 3.4 | … | … |
| CRP, mg/L | 389 (90.3) | <10 | 0–161 | <10, <10 | <10 | 37 (9.5) |
| B-leukocytes, ×109/L | 401 (93.0) | 7.4 | 3.1–35.0 | 6.0, 9.0 | 3.50–8.80 | 110 (27.4) |
Abbreviations: CRP, C-reactive protein; CSF, cerebrospinal fluid.
Among the 431 patients, 48 had a CSF leukocyte count ≤5 x 106/L. Although their symptoms did not differ from patients with CSF pleocytosis, their symptom debut was more equally distributed throughout the year, with 40% presenting with symptoms between November and April. Only 15.2% of the patients with CSF pleocytosis had symptom debut in these months (P < .001).
Borrelia Antibodies
CSF-Borrelia IgM/IgG AI and S-Borrelia IgM/IgG at the time of the first positive CSF-Borrelia AI are shown in Table 4.
Borrelia Antibody Profile in Serum and Cerebrospinal Fluid (CSF) at the Time of the First Positive CSF Borrelia Antibody Index in 431 Patients With Lyme Neuroborreliosis
| CSF Result | Serum | Total No. of Patients | |||
|---|---|---|---|---|---|
| Positive IgM | Positive IgG | Positive IgM + IgG | Negative IgM + IgG | ||
| Positive AI IgM | 21 | 46 | 61 | 23 | 151 |
| Positive AI IgG | 32 | 4 | 15 | 27 | 78 |
| Positive AI IgM + IgG | 62 | 39 | 84 | 17 | 202 |
| Total No. of patients | 115 | 89 | 160 | 67 | 431 |
| CSF Result | Serum | Total No. of Patients | |||
|---|---|---|---|---|---|
| Positive IgM | Positive IgG | Positive IgM + IgG | Negative IgM + IgG | ||
| Positive AI IgM | 21 | 46 | 61 | 23 | 151 |
| Positive AI IgG | 32 | 4 | 15 | 27 | 78 |
| Positive AI IgM + IgG | 62 | 39 | 84 | 17 | 202 |
| Total No. of patients | 115 | 89 | 160 | 67 | 431 |
Abbreviations: AI, antibody index; CSF, cerebrospinal fluid; IgG, immunoglobulin G; IgM, immunoglobulin M.
Borrelia Antibody Profile in Serum and Cerebrospinal Fluid (CSF) at the Time of the First Positive CSF Borrelia Antibody Index in 431 Patients With Lyme Neuroborreliosis
| CSF Result | Serum | Total No. of Patients | |||
|---|---|---|---|---|---|
| Positive IgM | Positive IgG | Positive IgM + IgG | Negative IgM + IgG | ||
| Positive AI IgM | 21 | 46 | 61 | 23 | 151 |
| Positive AI IgG | 32 | 4 | 15 | 27 | 78 |
| Positive AI IgM + IgG | 62 | 39 | 84 | 17 | 202 |
| Total No. of patients | 115 | 89 | 160 | 67 | 431 |
| CSF Result | Serum | Total No. of Patients | |||
|---|---|---|---|---|---|
| Positive IgM | Positive IgG | Positive IgM + IgG | Negative IgM + IgG | ||
| Positive AI IgM | 21 | 46 | 61 | 23 | 151 |
| Positive AI IgG | 32 | 4 | 15 | 27 | 78 |
| Positive AI IgM + IgG | 62 | 39 | 84 | 17 | 202 |
| Total No. of patients | 115 | 89 | 160 | 67 | 431 |
Abbreviations: AI, antibody index; CSF, cerebrospinal fluid; IgG, immunoglobulin G; IgM, immunoglobulin M.
In total, 67 patients (15.5%) were negative by both S-Borrelia IgM and IgG. Of these, 45 had CSF pleocytosis. Of the 105 patients who had displayed symptoms for >6 weeks prior to blood sampling, 22 had negative S-Borrelia IgM and IgG, giving an S-Borrelia sensitivity of 79.0%. Nine of these 22 patients had a subsequent S-Borrelia performed 14 days to 36 months later (mean, 5 months). One patient had converted to a positive S-Borrelia IgM; the others were continuously S-Borrelia IgM and IgG negative.
Of the 67 S-Borrelia negative patients, 62 of 355 were tested with IDEIA, and 5 of 76 with Enzygnost (P < .05).
A quantitative Borrelia AI value was available for 292 patients, a positive Borrelia IgG AI in 185 patients (median value, 4.40), and a positive Borrelia IgM AI in 237 patients (median value, 7.97). Of the 48 patients without CSF pleocytosis, 37 patients had a quantitative Borrelia AI value available. Nine had a positive Borrelia IgG AI with a median value of 1.43 (P = .38 compared to patients with CSF pleocytosis), and 31 had a positive Borrelia IgM AI with a median value of 0.84 (P < .01).
Course of Disease
The median delay from debut of neurological symptoms to first hospital contact was 20 days (IQR, 32[8–40] days). In children, the median delay was 10.5 days (IQR, 17[5–22] days), significantly shorter than for adults (21 days [IQR, 45[13–58] days]; P < .001). There was no difference in patient delay between the sexes. The median hospital delay was 1 day (IQR, 8 days).
The month of symptom debut, first hospital contact, and treatment start is displayed in Figure 1. Patients with symptom debut between November and April had a significantly longer treatment delay (median, 38.5 days [IQR, 145[14–159] days]) compared with patients with symptom debut between May and October (median, 22 days [IQR, 35[14–49] days]; P < .01).
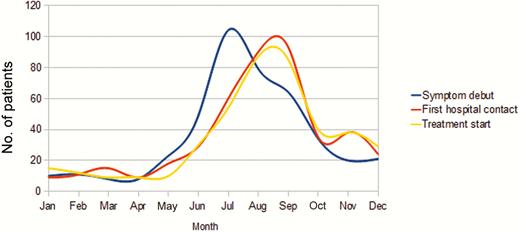
Month of debut of neurological symptoms and first hospital contact for 431 patients with Lyme neuroborreliosis (LNB), and month of start of treatment for 418 patients treated for LNB, 1995–2014.
Three hundred sixty-nine (85.6%) patients were hospitalized at some point during their course of disease; 118 (93.7%) of the 126 children. One hundred thirty-two patients (30.6%) were seen in >1 hospital department, but 82.5% of the children were seen only at the Department of Paediatrics. We found a significant difference in hospital delay among the different departments (P < .001), and an additional hospital delay for patients seen in ≥2 departments (P < .001).
Treatment Delay
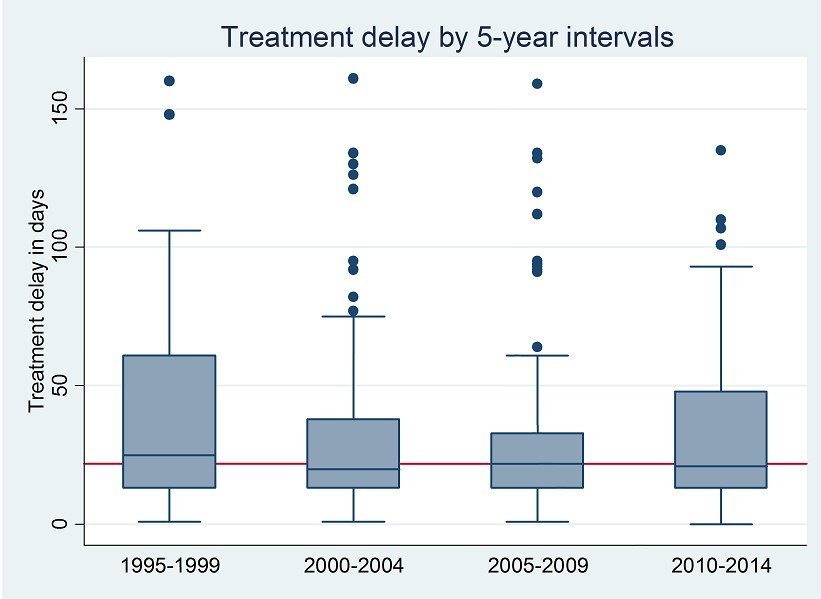
All except 13 patients received antibiotic treatment. The median treatment delay was 24 days (IQR, 44[14–58] days). Children had a significantly shorter median treatment delay compared with adults (15 days [IQR, 24[6–30] days] vs 29.5 days [IQR, 54[16–70] days]; P < .001). The treatment delay was constant during the 20-year study period (Supplementary Figure 2). In 170 patients, the treatment delay was >30 days. This group had a significantly higher proportion of radicular pain (77.1% vs 58.9%; P < .001), but less frequent intermittent fever (18.8% vs 28.2%; P = .03) and cranial nerve palsy (23.5% vs 57.7%; P < .001) compared with patients with treatment delay ≤30 days.
A lack of CSF pleocytosis was also associated with a longer treatment delay (median, 56 days [IQR, 384 days] vs 22 days [IQR, 36 days] in the CSF pleocytosis group; P < .01).
Twenty patients had a treatment delay of >1 year.
Treatment
The patients received antibiotic treatment regimens consisting of penicillin, ceftriaxone, and/or doxycycline; 110 patients received ≥1 type of antibiotic (Table 5).
Antibiotic Treatment Type and Treatment Length Among 431 Patients With Lyme Neuroborreliosis
| Treatment | No. (%) of Patients | Mean Total Length of Treatment, d (Range) | 1995–1999 | 2000–2004 | 2005–2009 | 2010–2014 |
|---|---|---|---|---|---|---|
| Penicillin G IV | 175 (40.6) | 10 (7–21) | 42 (60.0) | 66 (55.5) | 62 (44.6) | 5 (4.9) |
| Penicillin V PO | 1 (0.2) | 10 | 1 (1.4) | |||
| Doxycycline PO | 47 (10.9) | 21 (10–31) | 1 (1.4) | 10 (8.4) | 11 (7.9) | 25 (24.3) |
| Ceftriaxone IV | 85 (19.7) | 14 (10–24) | 15 (21.4) | 15 (12.6) | 24 (17.3) | 31 (30.1) |
| Ceftriaxone IV + doxycycline PO | 39 (9.0) | 21 (14–42) | 3 (4.3) | 8 (5.8) | 28 (27.2) | |
| Penicillin G IV + ceftriaxone IV | 38 (8.8) | 15 (1–30) | 5 (7.1) | 11 (9.2) | 12 (8.6) | 10 (9.7) |
| Ceftriaxone IV + penicillin V PO | 3 (0.7) | 14 (9–21) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + doxycycline | 12 (2.8) | 21 (14–44) | 1 (1.4) | 3 (2.5) | 8 (5.8) | |
| Penicillin G IV + penicillin V PO | 3 (0.7) | 14 (14) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + ceftriaxone IV + doxycycline | 15 (3.5) | 21 (20–73) | 1 (1.4) | 9 (7.6) | 3 (2.2) | 2 (1.9) |
| No antibiotics | 13 (3.0) | … | 1 (1.4) | 3 (2.5) | 7 (5.0) | 2 (1.9) |
| Total No. of patients | 431 | … | 70 | 119 | 139 | 103 |
| Treatment | No. (%) of Patients | Mean Total Length of Treatment, d (Range) | 1995–1999 | 2000–2004 | 2005–2009 | 2010–2014 |
|---|---|---|---|---|---|---|
| Penicillin G IV | 175 (40.6) | 10 (7–21) | 42 (60.0) | 66 (55.5) | 62 (44.6) | 5 (4.9) |
| Penicillin V PO | 1 (0.2) | 10 | 1 (1.4) | |||
| Doxycycline PO | 47 (10.9) | 21 (10–31) | 1 (1.4) | 10 (8.4) | 11 (7.9) | 25 (24.3) |
| Ceftriaxone IV | 85 (19.7) | 14 (10–24) | 15 (21.4) | 15 (12.6) | 24 (17.3) | 31 (30.1) |
| Ceftriaxone IV + doxycycline PO | 39 (9.0) | 21 (14–42) | 3 (4.3) | 8 (5.8) | 28 (27.2) | |
| Penicillin G IV + ceftriaxone IV | 38 (8.8) | 15 (1–30) | 5 (7.1) | 11 (9.2) | 12 (8.6) | 10 (9.7) |
| Ceftriaxone IV + penicillin V PO | 3 (0.7) | 14 (9–21) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + doxycycline | 12 (2.8) | 21 (14–44) | 1 (1.4) | 3 (2.5) | 8 (5.8) | |
| Penicillin G IV + penicillin V PO | 3 (0.7) | 14 (14) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + ceftriaxone IV + doxycycline | 15 (3.5) | 21 (20–73) | 1 (1.4) | 9 (7.6) | 3 (2.2) | 2 (1.9) |
| No antibiotics | 13 (3.0) | … | 1 (1.4) | 3 (2.5) | 7 (5.0) | 2 (1.9) |
| Total No. of patients | 431 | … | 70 | 119 | 139 | 103 |
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: IV, intravenous; PO, oral.
Antibiotic Treatment Type and Treatment Length Among 431 Patients With Lyme Neuroborreliosis
| Treatment | No. (%) of Patients | Mean Total Length of Treatment, d (Range) | 1995–1999 | 2000–2004 | 2005–2009 | 2010–2014 |
|---|---|---|---|---|---|---|
| Penicillin G IV | 175 (40.6) | 10 (7–21) | 42 (60.0) | 66 (55.5) | 62 (44.6) | 5 (4.9) |
| Penicillin V PO | 1 (0.2) | 10 | 1 (1.4) | |||
| Doxycycline PO | 47 (10.9) | 21 (10–31) | 1 (1.4) | 10 (8.4) | 11 (7.9) | 25 (24.3) |
| Ceftriaxone IV | 85 (19.7) | 14 (10–24) | 15 (21.4) | 15 (12.6) | 24 (17.3) | 31 (30.1) |
| Ceftriaxone IV + doxycycline PO | 39 (9.0) | 21 (14–42) | 3 (4.3) | 8 (5.8) | 28 (27.2) | |
| Penicillin G IV + ceftriaxone IV | 38 (8.8) | 15 (1–30) | 5 (7.1) | 11 (9.2) | 12 (8.6) | 10 (9.7) |
| Ceftriaxone IV + penicillin V PO | 3 (0.7) | 14 (9–21) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + doxycycline | 12 (2.8) | 21 (14–44) | 1 (1.4) | 3 (2.5) | 8 (5.8) | |
| Penicillin G IV + penicillin V PO | 3 (0.7) | 14 (14) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + ceftriaxone IV + doxycycline | 15 (3.5) | 21 (20–73) | 1 (1.4) | 9 (7.6) | 3 (2.2) | 2 (1.9) |
| No antibiotics | 13 (3.0) | … | 1 (1.4) | 3 (2.5) | 7 (5.0) | 2 (1.9) |
| Total No. of patients | 431 | … | 70 | 119 | 139 | 103 |
| Treatment | No. (%) of Patients | Mean Total Length of Treatment, d (Range) | 1995–1999 | 2000–2004 | 2005–2009 | 2010–2014 |
|---|---|---|---|---|---|---|
| Penicillin G IV | 175 (40.6) | 10 (7–21) | 42 (60.0) | 66 (55.5) | 62 (44.6) | 5 (4.9) |
| Penicillin V PO | 1 (0.2) | 10 | 1 (1.4) | |||
| Doxycycline PO | 47 (10.9) | 21 (10–31) | 1 (1.4) | 10 (8.4) | 11 (7.9) | 25 (24.3) |
| Ceftriaxone IV | 85 (19.7) | 14 (10–24) | 15 (21.4) | 15 (12.6) | 24 (17.3) | 31 (30.1) |
| Ceftriaxone IV + doxycycline PO | 39 (9.0) | 21 (14–42) | 3 (4.3) | 8 (5.8) | 28 (27.2) | |
| Penicillin G IV + ceftriaxone IV | 38 (8.8) | 15 (1–30) | 5 (7.1) | 11 (9.2) | 12 (8.6) | 10 (9.7) |
| Ceftriaxone IV + penicillin V PO | 3 (0.7) | 14 (9–21) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + doxycycline | 12 (2.8) | 21 (14–44) | 1 (1.4) | 3 (2.5) | 8 (5.8) | |
| Penicillin G IV + penicillin V PO | 3 (0.7) | 14 (14) | 1 (0.8) | 2 (1.4) | ||
| Penicillin G IV + ceftriaxone IV + doxycycline | 15 (3.5) | 21 (20–73) | 1 (1.4) | 9 (7.6) | 3 (2.2) | 2 (1.9) |
| No antibiotics | 13 (3.0) | … | 1 (1.4) | 3 (2.5) | 7 (5.0) | 2 (1.9) |
| Total No. of patients | 431 | … | 70 | 119 | 139 | 103 |
Data are presented as No. (%) unless otherwise indicated.
Abbreviations: IV, intravenous; PO, oral.
When dividing the study period into 5-year intervals, we found a decrease in the use of intravenous penicillin (from 60.9% in 1995–1999 to 4.9% in 2010–2014) and an increase in the use of doxycycline (from 1.4% to 24.3%), ceftriaxone (from 21.4% to 30.1%), and ceftriaxone followed by doxycycline (from 4.3% to 27.2%) in the same time periods. The mean treatment length was 14.8 days (standard deviation, 6.8).
Subsequent Treatment
After their initial treatment, 12 patients received subsequent antibiotics due to persisting residual symptoms. The subsequent treatment was given from 2 months up to 8 years after the initial treatment, and 4 patients received >1 subsequent treatment regimen. Only 1 patient reported an effect of the subsequent treatment; in most cases, the effect was not known due to lack of follow-up.
Patients Who Did Not Receive Treatment
Thirteen patients did not receive antibiotic treatment. Of these, 11 patients did not have CSF pleocytosis. As regards symptoms, 3 had cranial nerve palsy, 3 radicular pain, and 2 headache. Five displayed multiple symptoms: (1) headache and intermittent fever; (2) radicular pain and headache; (3) radicular pain and fatigue; (4) peripheral nerve paresis and radicular pain; (5) intermittent fever, radicular pain, headache, and cranial nerve palsy. Eight had no follow-up after lumbar puncture. Of the 5 patients followed up, 1 had persisting headache and 1 persisting peripheral nerve paresis. None had a repeated lumbar puncture.
Residual Symptoms
We registered the first mention of a treatment effect in the records of the 418 patients who received antibiotic therapy (Table 6). The majority experienced an effect within the first week or month after initiation of antibiotics. Only 14 patients (3.2%) reported no treatment response.
Time from Initiation of Antibiotic Treatment to First Mention of Any Treatment Effect in 418 Patients Treated for Lyme Neuroborreliosis (LNB), and Residual Symptoms in 431 Patients With LNB
| Outcome | No. of Patients |
|---|---|
| Time to treatment response | |
| <1 wk | 157 |
| Between 1 wk and 4 wk | 153 |
| Between 4 wk and 12 wk | 30 |
| Between 12 wk and 6 mo | 11 |
| Between 6 mo and 1 y | 10 |
| Registered with no response | 14 |
| Not reported | 43 |
| Type of residual symptomsa | |
| Radicular pain | 52 |
| Paresis | 22 |
| Cognitive | 27 |
| Otherb | 9 |
| No sequelae | 258 |
| No follow-up registered | 72 |
| Outcome | No. of Patients |
|---|---|
| Time to treatment response | |
| <1 wk | 157 |
| Between 1 wk and 4 wk | 153 |
| Between 4 wk and 12 wk | 30 |
| Between 12 wk and 6 mo | 11 |
| Between 6 mo and 1 y | 10 |
| Registered with no response | 14 |
| Not reported | 43 |
| Type of residual symptomsa | |
| Radicular pain | 52 |
| Paresis | 22 |
| Cognitive | 27 |
| Otherb | 9 |
| No sequelae | 258 |
| No follow-up registered | 72 |
aNine patients had >1 residual symptom.
bOther residual symptoms (No. of patients): fatigue (3), headache (2), impaired balance (1), opsoclonus/myoclonus syndrome (1), impaired hearing (1), dizziness (1).
Time from Initiation of Antibiotic Treatment to First Mention of Any Treatment Effect in 418 Patients Treated for Lyme Neuroborreliosis (LNB), and Residual Symptoms in 431 Patients With LNB
| Outcome | No. of Patients |
|---|---|
| Time to treatment response | |
| <1 wk | 157 |
| Between 1 wk and 4 wk | 153 |
| Between 4 wk and 12 wk | 30 |
| Between 12 wk and 6 mo | 11 |
| Between 6 mo and 1 y | 10 |
| Registered with no response | 14 |
| Not reported | 43 |
| Type of residual symptomsa | |
| Radicular pain | 52 |
| Paresis | 22 |
| Cognitive | 27 |
| Otherb | 9 |
| No sequelae | 258 |
| No follow-up registered | 72 |
| Outcome | No. of Patients |
|---|---|
| Time to treatment response | |
| <1 wk | 157 |
| Between 1 wk and 4 wk | 153 |
| Between 4 wk and 12 wk | 30 |
| Between 12 wk and 6 mo | 11 |
| Between 6 mo and 1 y | 10 |
| Registered with no response | 14 |
| Not reported | 43 |
| Type of residual symptomsa | |
| Radicular pain | 52 |
| Paresis | 22 |
| Cognitive | 27 |
| Otherb | 9 |
| No sequelae | 258 |
| No follow-up registered | 72 |
aNine patients had >1 residual symptom.
bOther residual symptoms (No. of patients): fatigue (3), headache (2), impaired balance (1), opsoclonus/myoclonus syndrome (1), impaired hearing (1), dizziness (1).
Of the 359 patients who were followed after the end of treatment, 101 patients (28.1%) reported 1 or more residual symptoms (Table 6). Children had fewer residual symptoms than adults (5.5% vs 38.2%; P < .001), and men had fewer residual symptoms than women (24.2% vs 34.3%; P = .038). No association was found between risk of residual symptoms and type of antibiotic treatment. Of the 34 patients without CSF pleocytosis who were followed after end of treatment, 20 (59%) had 1 or more residual symptoms; 14 had radicular pain, 5 cognitive sequelae, and 4 peripheral paresis.
Patients with a treatment delay of >30 days had a significantly higher proportion of residual symptoms (44.3%) compared to those with treatment delay ≤30 days (16.2%) (P < .001). This finding was most pronounced when looking at radicular pain (28.2% vs 4.9%; P < .001). The 52 patients with persistent radicular pain had a median treatment delay from symptom debut to initiation of antibiotic treatment of 87.5 days (IQR, 261[35.5–296.5] days).
We found no cases of reoccurring LNB infection during our study period. Only 2 patients died within 1 year of their LNB diagnosis. One died due to sudden cardiac arrest 6 months after successful treatment, and the other suffered an intracranial hemorrhage almost 1 year after successful treatment.
DISCUSSION
This is one of the largest studies of LNB patients to date. Our most surprising finding is that even though radicular pain was the most common symptom of LNB, it was associated with a significantly longer treatment delay than other symptoms. As expected, children presented more frequently with cranial nerve palsy and meningitis compared with adults [29]. These symptoms are commonly associated with LNB and could explain their shorter treatment delay compared to adults.
Although facial nerve palsy is the most common cranial nerve palsy in LNB patients [30], we found patients with paresis located to 8 of the 12 cranial nerves. Encephalitis is considered rare in LNB patients [6, 29], but was found in 16 patients (3.7%).
Former studies have implied that all LNB patients develop positive S-Borrelia antibodies 4–6 weeks after infection [31, 32]. Continuously negative S-Borrelia antibodies have been deemed as no LNB [3], which does not correlate with our findings. We found negative S-Borrelia antibodies at time of positive CSF-Borrelia AI in 15.5% of patients, though somewhat lower (7%), with the Enzygnost test that includes recombinant VlsE in addition to native B. afzelii antigen. We found a S-Borrelia sensitivity of only 79.0% after 6 weeks, and 8 of 9 retested patients were still negative after a mean time period of 5 months. Based on these results, we do not recommend using S-Borrelia antibodies alone to screen for LNB. If LNB is suspected due to relevant clinical symptoms, a lumbar puncture with a Borrelia AI test should be performed regardless of S-Borrelia antibody results.
We found a relatively long treatment delay of a median of 24 days. This may represent the lacking awareness of LNB symptoms among both patients and doctors. Of the 20 patients with a treatment delay of >1 year from symptom debut, 16 had classical radicular pain. The many different departments and physicians seeing LNB patients may have contributed to the long delay, which may also represent difficulties distinguishing between radicular pain due to LNB and pain due to musculoskeletal disorders. Our findings emphasize the need for greater knowledge of LNB symptoms among both the general population and physicians in high-endemic areas. The time of year of symptom debut significantly affected the time to treatment, presumably because LNB is associated with the late summer/fall [33].
Almost one-third of our patients had residual symptoms that persisted after treatment. The correlation between treatment delay and risk of residual symptoms once again stresses the importance of early-onset antibiotic treatment [8]. The risk of residual symptoms in our study could be underreported, as a considerable number of patients (16.7%) had no follow-up after end of treatment. There are, however, limitations in that we do not have standardized data on time from treatment to registration of the residual symptoms. As patients were included in the study at time of diagnosis and not time of infection, we cannot rule out that patients with long delays were selected due to their persisting symptoms and would not have been diagnosed if their symptoms had remitted.
Our patients received antibiotic treatment for a mean of 14.8 days, which is according to European LNB treatment guidelines [8]. Although further studies are needed to strengthen the evidence of the current treatment recommendations, prolonged antibiotic treatment has not shown additional treatment effect in LNB patients [12, 34]. In accordance with previous studies, we did not find any association between the type of antibiotic treatment and treatment outcome [7, 13, 35, 36].
We chose to include all patients with a positive CSF-Borrelia AI and symptoms of neuroborreliosis. This included 48 patients without CSF pleocytosis, who by definition are categorized as possible neuroborreliosis [8]. Even though they displayed the same symptoms as patients with CSF pleocytosis—symptoms compatible with LNB—their treatment delay was longer. Almost 1 in 4 patients (11/48) in this group did not receive antibiotic treatment. Typically, these patients were discharged when the CSF showed no inflammation, before the results of the CSF-Borrelia AI were available. When the test later came out positive, it was either deemed a false-positive test or interpreted as a sign of prior neuroborreliosis, which cannot be ruled out. However, the IDEAI LNB ELISA test has a reported specificity of 99% [37]. Based on the positive CSF-Borrelia AI and LNB symptoms at time of lumbar puncture, we chose to include these patients in our study.
When looking at the LNB patients over time, we found fewer hospitalizations in the last years of the study. This is probably due to a shift in treatment from intravenous penicillin given 4 times daily to intravenous ceftriaxone once daily and oral doxycycline. We did not, however, see any significant decrease in treatment delay over time or in the number of patients with residual symptoms after treatment. These were unexpected findings.
The greatest strengths of the study are the large number of patients included and the well-defined study population in a well-defined geographical area. Limitations to the study are that, because it was made retrospectively, not all data were available for all patients, patients were enrolled based on the time of their diagnosis instead of their symptom debut, and some patients were lost to follow-up.
Our study consists of LNB patients in a European setting, where B. afzelii and B. garinii are the most frequent Borrelia genospecies. This should be noted when extrapolating the results to a US setting, where B. burgdorferi sensu stricto is the only species to cause human disease [3].
In conclusion, this large study of >400 LNB patients showed that even though patients presented with classical symptoms, it is still today, as it was 20 years ago, a challenge to diagnose patients in due time and hence reduce the risk of residual symptoms after treatment. We advise against using S-Borrelia antibodies alone as a diagnostic tool to exclude the diagnosis of LNB. Furthermore, lack of CSF pleocytosis does not rule out the diagnosis. Finally, the health system should focus on shortening the time span from onset of symptoms to initiation of treatment in the hope of diminishing the risk of residual symptoms following LNB.
Supplementary Data
Supplementary materials are available at Clinical Infectious Diseases online. Consisting of data provided by the author to benefit the reader, the posted materials are not copyedited and are the sole responsibility of the author, so questions or comments should be addressed to the author.
Notes
Acknowledgments. We thank Assar Huss, Chief Statistical Consultant at Number Analytics, for help with the statistical analyses. We also thank Professor Isik Somuncu Johansen at the Department of Infectious Diseases, Odense University Hospital, for valuable discussions.
Financial support. This work was supported by the Research Fund at the Senior Consultant Council, Odense University Hospital.
Potential conflicts of interest. All authors: No reported conflicts of interest. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
References


{kind=link}
{kind=link}
Comments