
Abstract
Infective endocarditis (IE) is lethal if not aggressively treated with antibiotics alone or in combination with surgery. The epidemiology of this condition has substantially changed over the past four decades, especially in industrialized countries. Once a disease that predominantly affected young adults with previously well-identified valve disease—mostly chronic rheumatic heart disease—IE now tends to affect older patients and new at-risk groups, including intravenous-drug users, patients with intracardiac devices, and patients exposed to healthcare-associated bacteremia. As a result, skin organisms (for example, Staphylococcus spp.) are now reported as the pathogen in these populations more often than oral streptococci, which still prevail in the community and in native-valve IE. Moreover, progress in molecular diagnostics has helped to improve the diagnosis of poorly cultivable pathogens, such as Bartonella spp. and Tropheryma whipplei, which are responsible for blood-culture-negative IE more often than expected. Epidemiological data indicate that IE mostly occurs independently of medico-surgical procedures, and that circumstantial antibiotic prophylaxis is likely to protect only a minute proportion of individuals at risk. Therefore, new strategies to prevent IE—including improvement of dental hygiene, decontamination of carriers of Staphylococcus aureus, vaccination, and, possibly, antiplatelet therapy—must be explored.
Key Points
-
Infective endocarditis (IE) remains universally lethal if not aggressively treated
-
Medical progress has altered the epidemiology of IE
-
Healthcare-associated IE has become a major issue in industrialized countries
-
Prophylaxis for IE has been questioned and new guidelines have been proposed
-
Successful therapy for IE is being challenged by the development of antibiotic resistance
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others
References
Moreillon, P. & Que, Y. A. Infective endocarditis. Lancet 363, 139–149 (2004).
Hoen, B. et al. Changing profile of infective endocarditis: results of a 1-year survey in France. JAMA 288, 75–81 (2002).
Tleyjeh, I. M. et al. A systematic review of population-based studies of infective endocarditis. Chest 132, 1025–1035 (2007).
de Sa, D. D. et al. Epidemiological trends of infective endocarditis: a population-based study in Olmsted County, Minnesota. Mayo Clin. Proc. 85, 422–426 (2010).
Delahaye, F. et al. Characteristics of infective endocarditis in France in 1991. A 1-year survey. Eur. Heart J. 16, 394–401 (1995).
Hasbun, R., Vikram, H. R., Barakat, L. A., Buenconsejo, J. & Quagliarello, V. J. Complicated left-sided native valve endocarditis in adults: risk classification for mortality. JAMA 289, 1933–1940 (2003).
Chirouze, C. et al. Prognostic factors in 61 cases of Staphylococcus aureus prosthetic valve infective endocarditis from the International Collaboration on Endocarditis merged database. Clin. Infect. Dis. 38, 1323–1327 (2004).
Normand, J., Bozio, A., Etienne, J., Sassolas, F. & Le Bris, H. Changing patterns and prognosis of infective endocarditis in childhood. Eur. Heart J. 16 (Suppl. B), 28–31 (1995).
Letaief, A. et al. Epidemiology of infective endocarditis in Tunisia: a 10-year multicenter retrospective study. Int. J. Infect. Dis. 11, 430–433 (2007).
Hill, E. E. et al. Infective endocarditis: changing epidemiology and predictors of 6-month mortality: a prospective cohort study. Eur. Heart J. 28, 196–203 (2007).
Cabell, C. H. et al. Changing patient characteristics and the effect on mortality in endocarditis. Arch. Intern. Med. 162, 90–94 (2002).
Fowler, V. G., Jr et al. Staphylococcus aureus endocarditis: a consequence of medical progress. JAMA 293, 3012–3021 (2005).
Lopez, J. et al. Age-dependent profile of left-sided infective endocarditis: a 3-center experience. Circulation 121, 892–897 (2010).
Durante-Mangoni, E. et al. Current features of infective endocarditis in elderly patients: results of the International Collaboration on Endocarditis Prospective Cohort Study. Arch. Intern. Med. 168, 2095–2103 (2008).
Baddour, L. M. et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation 111, e394–e434 (2005).
Habib, G. et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis (new version 2009): the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Eur. Heart J. 30, 2369–2413 (2009).
Wilson, L. E., Thomas, D. L., Astemborski, J., Freedman, T. L. & Vlahov, D. Prospective study of infective endocarditis among injection drug users. J. Infect. Dis. 185, 1761–1766 (2002).
von Reyn, C. F., Levy, B. S., Arbeit, R. D., Friedland, G. & Crunpacker, C. S. Infective endocarditis: an analysis based on strict case definitions. Ann. Intern. Med. 94, 505–518 (1981).
van der Meer, J. T., Thompson, J., Valkenburg, H. A. & Michel, M. F. Epidemiology of bacterial endocarditis in The Netherlands. I. Patient characteristics. Arch. Intern. Med. 152, 1863–1868 (1992).
van der Meer, J. T., Thompson, J., Valkenburg, H. A. & Michel, M. F. Epidemiology of bacterial endocarditis in The Netherlands. II. Antecedent procedures and use of prophylaxis. Arch. Intern. Med. 152, 1869–1873 (1992).
Murdoch, D. R. et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 169, 463–473 (2009).
Tleyjeh, I. M. et al. Temporal trends in infective endocarditis: a population-based study in Olmsted County, Minnesota. JAMA 293, 3022–3028 (2005).
Wang, A. et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA 297, 1354–1361 (2007).
Benito, N. et al. Health care-associated native valve endocarditis: importance of non-nosocomial acquisition. Ann. Intern. Med. 150, 586–594 (2009).
Fowler, V. G., Jr. et al. Infective endocarditis due to Staphylococcus aureus: 59 prospectively identified cases with follow-up. Clin. Infect. Dis. 28, 106–114 (1999).
Fernández-Hidalgo, N. et al. Contemporary epidemiology and prognosis of health care-associated infective endocarditis. Clin. Infect. Dis. 47, 1287–1297 (2008).
Day, M. D., Gauvreau, K., Shulman, S. & Newburger, J. W. Characteristics of children hospitalized with infective endocarditis. Circulation 119, 865–870 (2009).
Gerber, M. A. et al. Prevention of rheumatic fever and diagnosis and treatment of acute Streptococcal pharyngitis: a scientific statement from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young, the Interdisciplinary Council on Functional Genomics and Translational Biology, and the Interdisciplinary Council on Quality of Care and Outcomes Research: endorsed by the American Academy of Pediatrics. Circulation 119, 1541–1551 (2009).
Nesta, F. et al. New locus for autosomal dominant mitral valve prolapse on chromosome 13: clinical insights from genetic studies. Circulation 112, 2022–2030 (2005).
Grau, J. B., Pirelli, L., Yu, P. J., Galloway, A. C. & Ostrer, H. The genetics of mitral valve prolapse. Clin. Genet. 72, 288–295 (2007).
Freed, L. A. et al. Prevalence and clinical outcome of mitral-valve prolapse. N. Engl. J. Med. 341, 1–7 (1999).
Kim, S. et al. Relationship between severity of mitral regurgitation and prognosis of mitral valve prolapse: echocardiographic follow-up study. Am. Heart J. 132, 348–355 (1996).
Stehbens, W. E., Delahunt, B. & Zuccollo, J. M. The histopathology of endocardial sclerosis. Cardiovasc.Pathol. 9, 161–173 (2000).
Croft, L. B. et al. Age-related prevalence of cardiac valvular abnormalities warranting infectious endocarditis prophylaxis. Am. J. Cardiol. 94, 386–389 (2004).
Vongpatanasin, W., Hillis, L. D. & Lange, R. A. Prosthetic heart valves. N. Engl. J. Med. 335, 407–416 (1996).
Sidhu, P. et al. Mechanical or bioprosthetic valves in the elderly: a 20-year comparison. Ann. Thorac. Surg. 71, S257–S260 (2001).
Varstela, E. Personal follow-up of 100 aortic valve replacement patients for 1081 patient years. Ann. Chir. Gynaecol. 87, 205–212 (1998).
Tornos, P. et al. Clinical outcome and long-term prognosis of late prosthetic valve endocarditis: a 20-year experience. Clin. Infect. Dis. 24, 381–386 (1997).
Ivert, T. S. et al. Prosthetic valve endocarditis. Circulation 69, 223–232 (1984).
Wilson, W. R. et al. Prosthetic valve endocarditis. Ann. Intern. Med. 82, 751–756 (1975).
Lopez, J. et al. Definition, clinical profile, microbiological spectrum, and prognostic factors of early-onset prosthetic valve endocarditis. Eur. Heart J. 28, 760–765 (2007).
Moss, R. & Munt, B. Injection drug use and right sided endocarditis. Heart 89, 577–581 (2003).
Pulvirenti, J. J. et al. Infective endocarditis in injection drug users: importance of human immunodeficiency virus serostatus and degree of immunosuppression. Clin. Infect. Dis. 22, 40–45 (1996).
Gebo, K. A., Burkey, M. D., Lucas, G. M., Moore, R. D. & Wilson, L. E. Incidence of, risk factors for, clinical presentation, and 1-year outcomes of infective endocarditis in an urban HIV cohort. J. Acquir. Immune Defic. Syndr. 43, 426–432 (2006).
Mathew, J. et al. Clinical features, site of involvement, bacteriologic findings, and outcome of infective endocarditis in intravenous drug users. Arch. Intern. Med. 155, 1641–1648 (1995).
Zhan, C., Baine, W. B., Sedrakyan, A. & Steiner, C. Cardiac device implantation in the United States from 1997 through 2004: a population-based analysis. J. Gen. Intern. Med. 23 (Suppl. 1), 13–19 (2008).
Cabell, C. H. et al. Increasing rates of cardiac device infections among Medicare beneficiaries: 1990–1999 Am. Heart J. 147, 582–586 (2004).
Duval, X. et al. Endocarditis in patients with a permanent pacemaker: a 1-year epidemiological survey on infective endocarditis due to valvular and/or pacemaker infection. Clin. Infect. Dis. 39, 68–74 (2004).
Sohail, M. R. et al. Management and outcome of permanent pacemaker and implantable cardioverter-defibrillator infections. J. Am. Coll. Cardiol. 49, 1851–1859 (2007).
Baddour, L. M. et al. Update on cardiovascular implantable electronic device infections and their management: a scientific statement from the American Heart Association. Circulation 121, 458–477 (2010).
McGowan, J. E., Jr, Barnes, M. W. & Finland, M. Bacteremia at Boston City Hospital: Occurrence and mortality during 12 selected years (1935–1972), with special reference to hospital-acquired cases. J. Infect. Dis. 132, 316–335 (1975).
Rodríguez-Créixems, M. et al. Bloodstream infections: evolution and trends in the microbiology workload, incidence, and etiology, 1985–2006 Medicine (Baltimore) 87, 234–249 (2008).
Hoen, B. Infective endocarditis: a frequent disease in dialysis patients. Nephrol. Dial. Transplant. 19, 1360–1362 (2004).
Kamalakannan, D., Pai, R., Johnson, L., Gardin, J. & Saravolatz, L. Epidemiology and Clinical Outcomes of Infective Endocarditis in Hemodialysis Patients. Ann. Thorac. Surg. 83, 2081–2086 (2007).
Gouello, J. P. et al. Nosocomial endocarditis in the intensive care unit: an analysis of 22 cases. Crit. Care Med. 28, 377–382 (2000).
Chang, F. Y. et al. A prospective multicenter study of Staphylococcus aureus bacteremia: incidence of endocarditis, risk factors for mortality, and clinical impact of methicillin resistance. Medicine (Baltimore) 82, 322–332 (2003).
Moreillon, P., Que, Y. A. & Bayer, A. S. Pathogenesis of streptococcal and staphylococcal endocarditis. Infect. Dis. Clin. North Am. 16, 297–318 (2002).
Campbell, L. A. & Kuo, C. C. Chlamydia pneumoniae: an infectious risk factor for atherosclerosis? Nat. Rev. Microbiol. 2, 23–32 (2004).
Patti, J. M., Allen, B. L., McGavin, M. J. & Hook, M. MSCRAMM-mediated adherence of microorganisms to host tissues. Annu. Rev.Microbiol. 48, 585–617 (1994).
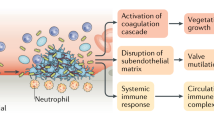
Widmer, E., Que, Y. A., Entenza, J. M. & Moreillon, P. New concepts in the pathophysiology of infective endocarditis. Curr. Infect. Dis. Rep. 8, 271–279 (2006).
Que, Y. A. et al. Fibrinogen and fibronectin binding cooperate for valve infection and invasion in Staphylococcus aureus experimental endocarditis. J. Exp. Med. 201, 1627–1635 (2005).
Piroth, L. et al. The fibrinogen- and fibronectin-binding domains of Staphylococcus aureus fibronectin-binding protein A synergistically promote endothelial invasion and experimental endocarditis. Infect. Immun. 76, 3824–3831 (2008).
Heying, R., van de Gevel, J., Que, Y. A., Moreillon, P. & Beekhuizen, H. Fibronectin-binding proteins and clumping factor A in Staphylococcus aureus experimental endocarditis: FnBPA is sufficient to activate human endothelial cells. Thromb. Haemost. 97, 617–626 (2007).
Heying, R. et al. Contribution of (sub)domains of Staphylococcus aureus fibronectin-binding protein to the proinflammatory and procoagulant response of human vascular endothelial cells. Thromb. Haemost. 101, 495–504 (2009).
Brouqui, P. & Raoult, D. Endocarditis due to rare and fastidious bacteria. Clin. Microbiol. Rev. 14, 177–207 (2001).
Herzberg, M. C. et al. The platelet interactivity phenotype of Streptococcus sanguis influences the course of experimental endocarditis. Infect.Immun. 60, 4809–4818 (1992).
Burnette-Curley, D. et al. FimA, a major virulence factor associated with Streptococcus parasanguis endocarditis. Infect. Immun. 63, 4669–4674 (1995).
Anderson, D. J. et al. Enterococcal prosthetic valve infective endocarditis: report of 45 episodes from the International Collaboration on Endocarditis-merged database. Eur. J. Clin. Microbiol. Infect. Dis. 24, 665–670 (2005).
Olaison, L. & Schadewitz, K. Enterococcal endocarditis in Sweden, 1995–1999: can shorter therapy with aminoglycosides be used? Clin. Infect. Dis. 34, 159–166 (2002).
Schlievert, P. M. et al. Aggregation and binding substances enhance pathogenicity in rabbit models of Enterococcus faecalis endocarditis. Infect. Immun. 66, 218–223 (1998).
Nallapareddy, S. R. et al. Endocarditis and biofilm-associated pili of Enterococcus faecalis. J. Clin. Invest. 116, 2799–2807 (2006).
Nallapareddy, S. R., Singh, K. V. & Murray, B. E. Contribution of the collagen adhesin Acm to pathogenesis of Enterococcus faecium in experimental endocarditis. Infect. Immun. 76, 4120–4128 (2008).
Singh, K. V., Nallapareddy, S. R., Sillanpaa, J. & Murray, B. E. Importance of the collagen adhesin ace in pathogenesis and protection against Enterococcus faecalis experimental endocarditis. PLoS Pathog. 6, e1000716 (2010).
Ythier, M. et al. Natural variability of in vitro adherence to fibrinogen and fibronectin does not correlate with in vivo infectivity of Staphylococcus aureus. Infect. Immun. 78, 1711–1716 (2010).
Moreillon, P., Overholser, C. D., Malinverni, R., Bille, J. & Glauser, M. P. Predictors of endocarditis in isolates from cultures of blood following dental extractions in rats with periodontal disease. J. Infect. Dis. 157, 990–995 (1988).
Hall, G., Heimdahl, A. & Nord, C. E. Bacteremia after oral surgery and antibiotic prophylaxis for endocarditis. Clin. Infect. Dis. 29, 1–8 (1999).
Roberts, G. J. Dentists are innocent! “Everyday” bacteremia is the real culprit: a review and assessment of the evidence that dental surgical procedures are a principal cause of bacterial endocarditis in children. Pediatr. Cardiol. 20, 317–325 (1999).
Pallasch, T. J. Antibiotic prophylaxis: theory and reality. J. Calif. Dent. Assoc. 17, 27–39 (1989).
Strom, B. L. et al. Dental and cardiac risk factors for infective endocarditis. A population-based, case-control study. Ann. Intern. Med. 129, 761–769 (1998).
Veloso, TR. et al. Induction of experimental endocarditis by continuous low-grade bacteremia mimicking spontaneous bacteremia in human. Infect. Immun. doi:10.1128/IAI.01208–10.
Durack, D. T. & Beeson, P. B. Experimental bacterial endocarditis. I. Colonization of a sterile vegetation. Brit. J. Exp. Pathol. 53, 44–49 (1972).
Nucifora, G. et al. Infective endocarditis in chronic haemodialysis patients: an increasing clinical challenge. Eur. Heart J. 28, 2307–2312 (2007).
Yersin, B., Glauser, M. P., Guze, P. A., Guze, L. B. & Freedman, L. R. Experimental Escherichia coli endocarditis in rats: role of serum bactericidal activity and duration of catheter placement. Infect. Immun. 56, 1273–1280 (1988).
Dankert, J. et al. Involvement of bactericidal factors from thrombin-stimulated platelets in clearance of adherent viridans streptococci in experimental infective endocarditis. Infect. Immun. 63, 663–671 (1995).
Fowler, V. G., Jr. et al. In vitro resistance to thrombin-induced platelet microbicidal protein in isolates of Staphylococcus aureus from endocarditis patients correlates with an intravascular device source. J. Infect. Dis. 182, 1251–1254 (2000).
Kitten, T., Munro, C. L., Wang, A. & Macrina, F. L. Vaccination with FimA from Streptococcus parasanguis protects rats from endocarditis caused by other viridans streptococci. Infect. Immun. 70, 422–425 (2002).
Vernachio, J. H. et al. Human immunoglobulin G recognizing fibrinogen-binding surface proteins is protective against both Staphylococcus aureus and Staphylococcus epidermidis infections in vivo. Antimicrob. Agents Chemother. 50, 511–518 (2006).
McCormick, J. K., Tripp, T. J., Dunny, G. M. & Schlievert, P. M. Formation of vegetations during infective endocarditis excludes binding of bacterial-specific host antibodies to Enterococcus faecalis. J. Infect. Dis. 185, 994–997 (2002).
Schlievert, P. M., Chuang-Smith, O. N., Peterson, M. L., Cook, L. C. & Dunny, G. M. Enterococcus faecalis endocarditis severity in rabbits is reduced by IgG Fabs interfering with aggregation substance. PLoS ONE 5, e13194 (2010).
Wilson, W. et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 116, 1736–1754 (2007).
Nicolau, D. P. et al. Reduction of bacterial titers by low-dose aspirin in experimental aortic valve endocarditis. Infect.Immun. 61, 1593–1595 (1993).
Li, J. S. et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 30, 633–638 (2000).
Lee, A., Mirrett, S., Reller, L. B. & Weinstein, M. P. Detection of bloodstream infections in adults: how many blood cultures are needed? J. Clin. Microbiol. 45, 3546–3548 (2007).
Habib, G. et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur. J. Echocardiogr. 11, 202–219 (2010).
Evangelista, A. & Gonzalez-Alujas, M. T. Echocardiography in infective endocarditis. Heart 90, 614–617 (2004).
Houpikian, P. & Raoult, D. Blood culture-negative endocarditis in a reference center: etiologic diagnosis of 348 cases. Medicine (Baltimore) 84, 162–173 (2005).
Richardson, D. C. et al. Tropheryma whippelii as a cause of afebrile culture-negative endocarditis: the evolving spectrum of Whipple's disease. J. Infect. 47, 170–173 (2003).
Fournier, P. E. et al. Comprehensive diagnostic strategy for blood culture-negative endocarditis: a prospective study of 819 new cases. Clin. Infect. Dis. 51, 131–140 (2010).
Brouqui, P. & Raoult, D. New insight into the diagnosis of fastidious bacterial endocarditis. FEMS Immunol. Med. Microbiol. 47, 1–13 (2006).
Lalani, T. et al. Analysis of the impact of early surgery on in-hospital mortality of native valve endocarditis: use of propensity score and instrumental variable methods to adjust for treatment-selection bias. Circulation 121, 1005–1013 (2010).
Aksoy, O. et al. Early surgery in patients with infective endocarditis: a propensity score analysis. Clin. Infect. Dis. 44, 364–372 (2007).
Cabell, C. H. et al. Use of surgery in patients with native valve infective endocarditis: results from the International Collaboration on Endocarditis Merged Database. Am. Heart J. 150, 1092–1098 (2005).
Tleyjeh, I. M. et al. The impact of valve surgery on 6-month mortality in left-sided infective endocarditis. Circulation 115, 1721–1728 (2007).
Vikram, H. R., Buenconsejo, J., Hasbun, R. & Quagliarello, V. J. Impact of valve surgery on 6-month mortality in adults with complicated, left-sided native valve endocarditis: a propensity analysis. JAMA 290, 3207–3214 (2003).
Wang, A. et al. The use and effect of surgical therapy for prosthetic valve infective endocarditis: a propensity analysis of a multicenter, international cohort. Am. Heart J. 150, 1086–1091 (2005).
Bannay, A. et al. The impact of valve surgery on short- and long-term mortality in left-sided infective endocarditis: do differences in methodological approaches explain previous conflicting results? Eur. Heart J. doi:10.1093/eurheartj/ehp008.
Prendergast, B. D. & Tornos, P. Surgery for infective endocarditis: who and when? Circulation 121, 1141–1152 (2010).
Kim, D. H. et al. Impact of early surgery on embolic events in patients with infective endocarditis. Circulation 122 (Suppl. 11), S17–S22 (2010).
Ruttmann, E. et al. Neurological outcome of septic cardioembolic stroke after infective endocarditis. Stroke 37, 2094–2099 (2006).
Thuny, F. et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur. Heart J. 28, 1155–1161 (2007).
Znazen, A. et al. High prevalence of Bartonella quintana endocarditis in Sfax, Tunisia. Am. J. Trop. Med. Hyg. 72, 503–507 (2005).
Benslimani, A., Fenollar, F., Lepidi, H. & Raoult, D. Bacterial zoonoses and infective endocarditis, Algeria. Emerg. Infect. Dis. 11, 216–224 (2005).
Knoll, B., Tleyjeh, I. M., Steckelberg, J. M., Wilson, W. R. & Baddour, L. M. Infective endocarditis due to penicillin-resistant viridans group streptococci. Clin. Infect. Dis. 44, 1585–1592 (2007).
Howden, B. P., Johnson, P. D., Ward, P. B., Stinear, T. P. & Davies, J. K. Isolates with low-level vancomycin resistance associated with persistent methicillin-resistant Staphylococcus aureus bacteremia. Antimicrob. Agents Chemother. 50, 3039–3047 (2006).
Centers for Disease Control and Prevention (CDC). Staphylococcus aureus resistant to vancomycin—United States, 2002. MMWR Morb. Mortal. Wkly Rep. 51, 565–567 (2002).
Centers for Disease Control and Prevention (CDC). Vancomycin-resistant Staphylococcus aureus—Pennsylvania, 2002. MMWR Morb. Mortal. Wkly Rep. 51, 902 (2002).
Fowler, V. G., Jr. et al. Daptomycin versus standard therapy for bacteremia and endocarditis caused by Staphylococcus aureus. N. Engl. J. Med. 355, 653–665 (2006).
Guignard, B., Entenza, J. M. & Moreillon, P. Beta-lactams against methicillin-resistant Staphylococcus aureus. Curr. Opin. Pharmacol. 5, 479–489 (2005).
Reynolds, R. et al. Antimicrobial susceptibility of the pathogens of bacteraemia in the UK and Ireland 2001–2002: the BSAC Bacteraemia Resistance Surveillance Programme. J. Antimicrob. Chemother. 53, 1018–1032 (2004).
Gavalda, J. et al. Brief communication: treatment of Enterococcus faecalis endocarditis with ampicillin plus ceftriaxone. Ann. Intern. Med. 146, 574–579 (2007).
Enoch, D. A., Phillimore, N., Karas, J. A., Horswill, L. & Mlangeni, D. A. Relapse of enterococcal prosthetic valve endocarditis with aortic root abscess following treatment with daptomycin in a patient not fit for surgery. J. Med. Microbiol. 59, 482–485 (2010).
Morpeth, S. et al. Non-HACEK gram-negative bacillus endocarditis. Ann. Intern. Med. 147, 829–835 (2007).
Pierrotti, L. C. & Baddour, L. M. Fungal endocarditis, 1995–2000 Chest 122, 302–310 (2002).
Ellis, M. E., Al-Abdely, H., Sandridge, A., Greer, W. & Ventura, W. Fungal endocarditis: evidence in the world literature, 1965–1995 Clin. Infect. Dis. 32, 50–62 (2001).
Garzoni, C., Nobre, V. A. & Garbino, J. Candida parapsilosis endocarditis: a comparative review of the literature. Eur. J. Clin. Microbiol. Infect. Dis. 26, 915–926 (2007).
Lye, D. C., Hughes, A., O'Brien, D. & Athan, E. Candida glabrata prosthetic valve endocarditis treated successfully with fluconazole plus caspofungin without surgery: a case report and literature review. Eur. J. Clin. Microbiol. Infect. Dis. 24, 753–755 (2005).
Moreillon, P. in Infectious Diseases 3rd Edn Vol. I Ch. 47 (ed Cohen, J., Powderly, W. G. & Opal, S. M.) 514–528 (Mosby, Philadelphia, 2010).
Ribera, E. et al. Effectiveness of cloxacillin with and without gentamicin in short-term therapy for right-sided Staphylococcus aureus endocarditis. A randomized, controlled trial. Ann. Intern. Med. 125, 969–974 (1996).
Olaison, L., Schadewitz, K. & Swedish Society of Infectious Diseases Quality Assurance Study Group for Endocarditis. Enterococcal endocarditis in Sweden, 1995–1999: can shorter therapy with aminoglycosides be used? Clin. Infect. Dis. 34, 159–166 (2002).
Buchholtz, K., Larsen, C. T., Hassager, C. & Bruun, N. E. Severity of gentamicin's nephrotoxic effect on patients with infective endocarditis: a prospective observational cohort study of 373 patients. Clin. Infect. Dis. 48, 65–71 (2009).
Acknowledgements
Y.-A. Que was supported by Swiss National Science Foundation/Swiss Medical Association (FMH) grant # PASMP3-123226 and a grant from the SICPA Foundation. P. Moreillon is supported by grant 3200B0-113854 from the Swiss National Science Foundation.
C. P. Vega, University of California, Irvine, CA, is the author of and is solely responsible for the content of the learning objectives, questions and answers of the Medscape, LLC-accredited continuing medical education activity associated with this article.
Author information
Authors and Affiliations
Contributions
Both authors contributed to discussion of content for the article, researched data to include in the manuscript, wrote, reviewed and edited the manuscript before submission, and revised the manuscript in response to the peer-reviewers' comments.
Corresponding author
Ethics declarations
Competing interests
P. Moreillon declares that he has been a consultant for and has received grant/research support from Novartis and Wyeth Pharmaceuticals during the past 2 years.
Y. A. Que declares no competing interests.
Rights and permissions
About this article
Cite this article
Que, YA., Moreillon, P. Infective endocarditis. Nat Rev Cardiol 8, 322–336 (2011). https://doi.org/10.1038/nrcardio.2011.43
Published:
Issue Date:
DOI: https://doi.org/10.1038/nrcardio.2011.43
This article is cited by
-
von Willebrand factor-binding protein (vWbp)-activated factor XIII and transglutaminase 2 (TG2) promote cross-linking between FnBPA from Staphylococcus aureus and fibrinogen
Scientific Reports (2023)
-
Infektiöse Endokarditis bei Kindern und Jugendlichen
Oralprophylaxe & Kinderzahnheilkunde (2023)
-
Recurrence of bacteremia and infective endocarditis according to bacterial species of index endocarditis episode
Infection (2023)
-
Pathogenomics of Streptococcus ilei sp. nov., a newly identified pathogen ubiquitous in human microbiome
Journal of Microbiology (2021)
-
Antineutrophil cytoplasmic antibodies (ANCA)-positive patient with infective endocarditis and chronic hepatitis B virus: a case report and review of the literature
Journal of Medical Case Reports (2020)
