


Abstract
Background: Because there are no standardized reporting systems specific to residents of retirement homes in North America, little is known about the health of this distinct population of older adults. We evaluated rates of health services use by residents of retirement homes relative to those of residents of long-term care homes and other populations of older adults.
Methods: We conducted a retrospective cohort study using population health administrative data from 2018 on adults 65 years or older in Ontario. We matched the postal codes of individuals to those of licensed retirement homes to identify residents of retirement homes. Outcomes included rates of hospital-based care and physician visits.
Results: We identified 54 733 residents of 757 retirement homes (mean age 86.7 years, 69.0% female) and 2 354 385 residents of other settings. Compared to residents of long-term care homes, residents of retirement homes had significantly higher rates per 1000 person months of emergency department visits (10.62 v. 4.48, adjusted relative rate [RR] 2.61, 95% confidence interval [CI] 2.55 to 2.67), hospital admissions (5.42 v. 2.08, adjusted RR 2.77, 95% CI 2.71 to 2.82), alternate level of care (ALC) days (6.01 v. 2.96, adjusted RR 1.51, 95% CI 1.48 to 1.54), and specialist physician visits (6.27 v. 3.21, adjusted RR 1.64, 95% CI 1.61 to 1.68), but a significantly lower rate of primary care visits (16.71 v. 108.47, adjusted RR 0.13, 95% CI 0.13 to 0.14).
Interpretation: Residents of retirement homes are a distinct population with higher rates of hospital-based care. Our findings can help to inform policy debates about the need for more coordinated primary and supportive health care in privately operated congregate care homes.
In the continuum of care services and settings for older adults lies home care at one end and long-term care at the other.1 Home care services may include, but are not limited to, nursing care, personal care, homemaking services, and physiotherapy and occupational therapy for older adults who live independently in their community. Home care services are publicly funded under the Ontario Health Insurance Plan (OHIP).2,3 Long-term care homes provide access to 24-hour nursing and personal care and operate at full capacity in Ontario, with waiting lists of 6 months or longer before an older adult in the community could receive an offer for a bed.2,4 Retirement homes are thought to fit between home care and long-term care in this continuum.1
Retirement homes are referred to as assisted-living facilities in other North American jurisdictions, and they are private, congregate living environments that deliver supportive care to adults who are 65 years of age and older.3,5,6 These homes are often marketed to provide a lifestyle and community, and they provide a range of assisted-living care services (e.g., meals, nursing services, etc.).5,7 Retirement homes predominately operate on a private, for-profit business model, and the room, board and services are purchased by residents.3,5 In Ontario, retirement homes are regulated through an independent, not-for-profit regulator (i.e., Retirement Homes Regulatory Authority [RHRA]).5 There are more than 700 licensed retirement homes in Ontario with over 70 000 available beds occupied by over 55 000 residents, which is comparable to the number of available beds in the long-term care sector.3,5,6,8 Retirement homes are legislated differently from long-term care homes and primarily cater to adults who do not require 24-hour nursing care.1,5,9 Unlike long-term care homes, no standardized reporting system is available to identify and describe residents of retirement homes.10 These residents are conceptualized as having fewer needs for care because they reside in a congregate care home to support independent living; however, this has been difficult to verify given there are no population-level data.
A body of literature from the United States has described residents of assisted-living facilities and the sector,11–17 but Canadian literature is comparatively nascent. Canadian studies have investigated transitions to a long-term care home, risk of hospital admission among those who live with dementia, and life events and health conditions associated with the transition to a congregate care setting.7,9,18–20 At present, a Canadian population-level cohort of residents of retirement homes that describes the individual-level characteristics and use of health services of the older adults who reside in these homes appears to be lacking. Therefore, it is difficult to position this sector in the gradient of services and housing options for older adults in Canada.
We created a population-level cohort of residents in retirement homes and sought to evaluate their rates of health services utilization relative to residents of long-term care homes and other populations of older adults (i.e., home care recipients and community-dwelling older adults) in Ontario.
Methods
We conducted a population-based retrospective cohort study using linked, individual-level Ontario health system administrative data from 2018 that are held at ICES. ICES is an independent nonprofit research institute with legal status under Ontario’s health information privacy law that allows it to collect and analyze health care and demographic data, without consent, for evaluation and improvement of the health system. We have reported our study according to the REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement guideline (Appendix 1, Supplemental Table 1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.211883/tab-related-content).21
Data sources
We obtained access to the RHRA’s public register of licensed retirement homes, which contains historical data on the licence of the home, resident and suite capacities, provision of regulated care services and full postal address. We verified and visualized the postal code of each licensed retirement home through Canada Post, Statistics Canada and Google Maps. Building off research that evaluated the feasibility of using postal codes to identify residents of retirement homes,22 we used a modified taxonomy to classify the postal code of each licensed retirement home as unique, or not unique, to the retirement home. We imported the RHRA’s public register and our classified postal code data on licensed retirement homes to ICES. The health system administrative data sets we used are listed and described in Appendix 1, Supplemental Table 2. These data sets were linked using unique encoded identifiers and analyzed at ICES.
Study population
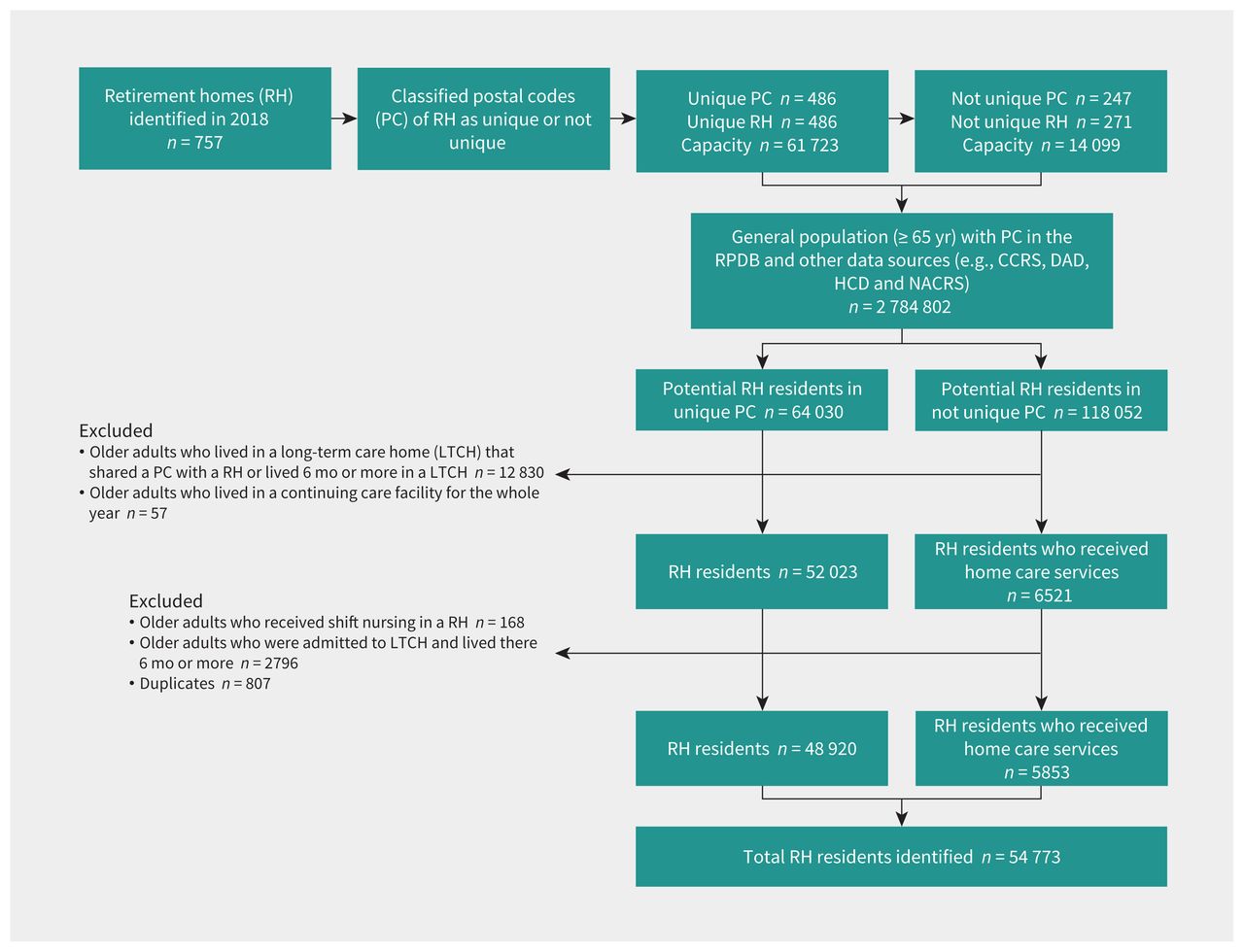
We identified adults who were 65 years of age and older from Jan. 1 to Dec. 31, 2018, and had a postal code that ever matched to a licensed retirement home with a unique postal code classification (Figure 1). There were substantially more older adults who had a postal code that matched to a licensed retirement home without a unique postal code classification than beds in licensed retirement homes. We limited our identification of residents in retirement homes in nonunique postal codes to residents at those postal codes who were identified as residing in a retirement home in census-level home care records, given that more than 40% of all residents of retirement homes are recipients of home care.3,9 We defined the index date as when the older adult’s postal code matched to the postal code of a licensed retirement home; we ended follow-up when the older adult transitioned to a long-term care home, complex continuing care facility or died.

Flow chart showing the creation of the Residents of Retirement Homes Cohort in 2018 (n = 54 773). Note: CCRS = Continuing Care Reporting System, DAD = Discharge Abstract Database, HCD = Home Care Database, NACRS = National Ambulatory Care Reporting System, RPDB = Registered Persons Database.
We excluded older adults who were residing in a long-term care home that was co-located with a retirement home and older adults who resided in a long-term care home for more than half of 2018 (i.e., 6 mo plus 1 d). We excluded older adults who resided in a continuing care facility for the whole year in 2018. We also excluded older adults who received shift nursing in retirement homes, as these people were only temporarily housed in the retirement home for specialized convalescent programs, and so they were not true residents of retirement homes. We excluded duplicates who moved from one retirement home to another during the year. According to the RHRA’s register, there were 75 822 beds in all licensed retirement homes in 2018; however, population surveys suggest that retirement homes operate at 74% overall capacity with about 56 491 residents as of May 2020.6
We identified residents of long-term care homes by their inclusion in the Continuing Care Reporting System. We differentiated older adults who received home care services from residents of retirement homes by their postal code that never matched to a postal code associated with a licensed retirement home. Community-dwelling older adults were defined as those who were 65 years of age or older and never met any of the above criteria. We defined the index date as when the older adult met the criteria to be categorized as one of these mutually exclusive populations in 2018; we ended follow-up when the older adult met the criteria to be categorized as a different population or died.
Variables
The outcomes of interest were rates of emergency department visits, hospital admissions, alternate levels of care (ALC) days (i.e., when a person occupies a bed in hospital because they cannot be safely discharged to a more appropriate setting in their community), primary care visits and specialist physician visits in 2018. We standardized these rates at the level of the individual (i.e., from index to end of follow-up). We defined emergency department visits as any care received in an emergency department. Hospital admissions were defined as any hospital admission. We obtained ALC days from the Discharge Abstract Database.
We defined primary care visits among residents of retirement homes, home care recipients and community-dwelling older adults as any billing by a family or community medicine physician to OHIP in which the location of the visit occurred in an office, home or via telephone. We similarly defined primary care visits among residents of long-term care homes as billings that were in accordance with monthly capitated primary care through consistent primary care providers under contract by the home and that included a long-term care home as the visit location. We defined specialist physician visits as any billing to OHIP by a physician whose specialty was not family or community medicine. All older adults could have only 1 primary care or specialist physician visit per physician per day.
We obtained demographic (i.e., age and sex) and community characteristics (i.e., urban location, neighbourhood income quintile, Ontario Marginalization Index) at the index date.23,24 We also obtained clinical comorbidities at the index date from physician-diagnosed billing codes to OHIP, International Classification of Diseases, 9th Revision (ICD-9) or International Statitical Classification of Diseases and Related Health Problems, 10th Revision (ICD-10) diagnosis codes, validated ICES-derived cohorts and the Canadian Institute for Health Information population grouping methodology.25–33
Statistical analysis
We calculated counts and proportions for categorical variables, and means and standard deviations (SDs) or medians and interquartile ranges (IQRs) for continuous variables. We calculated incidence densities and differences and 95% confidence intervals (CIs).34 We used a generalized linear model with a γ distribution and log link to model the standardized health service rates among the different populations of older adults, as this distribution and link are appropriate to model dispersed rates or costs in dollars.35 We obtained adjusted relative rates (RRs) and 95% CIs from exponentiated β coefficients. All statistical tests were 2-tailed, and we considered a p value of less than 0.05 to be significant. We conducted a sensitivity analysis involving residents only from unique postal codes. We also conducted a sex-stratified subgroup analysis. We used SAS Enterprise 9.4 for data set processing and statistical analyses.
Ethics approval
The use of the data in this study is authorized under Section 45 of Ontario’s Personal Health Information Protection Act and does not require review by a research ethics board.
Results
There were 757 licensed retirement homes in 2018 in Ontario (Table 1), and our approach identified a cohort of 54 733 residents in these homes (72.2% of all licensed beds). More than two-thirds of these residents were female (n = 37 768, 69.0%), and they had a mean age of 86.7 years (Table 2). Hypertension (n = 47 212, 86.2%), osteoarthritis (n = 36 978, 67.5%), mood disorders (n = 35 000, 63.9%) and dementia (n = 20 651, 37.7%) were prevalent clinical comorbidities. Almost all residents resided in urban communities (n = 50 650, 92.5%).
Characteristics of licensed retirement homes in Ontario (2018)
Sociodemographic characteristics and clinical comorbidities among residents of retirement homes, residents of long-term care homes, recipients of home care and community-dwelling older adults in Ontario in 2018
During 472 151.57 person-months of follow-up, residents of retirement homes had 10.62 emergency department visits, 5.42 hospital admissions, 6.01 ALC days, 16.71 primary care visits and 6.27 specialist physician visits per 1000 person-months (Table 3). We found that there was an excess rate of 6.14 emergency department visits, 3.33 hospital admissions, 3.04 ALC days and 3.06 specialist physician visits but 91.77 fewer primary care visits per 1000 person-months associated with being a resident of a retirement home compared with a resident of long-term care home (Table 4).
Incidence densities for health services received among residents of retirement homes, residents of long-term care homes, recipients of home care and community-dwelling older adults in 2018
Incidence density differences and adjusted relative rates for health services received among residents of retirement homes compared to residents of long-term care homes, recipients of home care and community-dwelling older adults in 2018
After we adjusted for relevant characteristics at the index date, residents of retirement homes had significantly higher rates of emergency department visits (adjusted RR 2.61, 95% CI 2.55 to 2.67), hospital admissions (adjusted RR 2.77, 95% CI 2.71 to 2.82) and ALC days (adjusted RR 1.51, 95% CI 1.48 to 1.54) than residents of long-term care homes. Residents of retirement homes had a lower rate of primary care visits (RR 0.13, 95% CI 0.13 to 0.14), but a significantly higher rate of specialist physician visits (RR 1.64, 95% CI 1.61 to 1.68), compared with residents of long-term care homes.
Similarly, compared to recipients of home care, residents of retirement homes had significantly higher adjusted RRs of emergency department visits, hospital aadmissions and ALC days and lower rates of primary care visits, although relative differences were in most cases of lesser magnitude than those between residents of retirement homes and residents of long-term care homes (Table 4). However, residents of retirement homes had significantly lower rates of specialist physician visits than recipients of home care (RR 0.51, 95% CI 0.50 to 0.52). Rates of all outcomes were higher among residents of retirement homes than among community-dwelling older adults, markedly so for hospital-based care outcomes (Table 4).
The results of our primary analysis did not change when we meaningfully analyzed only residents of retirement homes from unique postal codes (Appendix 1, Supplemental Table 3, Supplemental Table 4, Supplemental Table 5). Female residents of retirement homes had a significantly higher rate of ALC days (RR 2.63, 95% CI 2.58 to 2.69), whereas male residents of retirement homes had a significantly lower rate of ALC days (RR 0.86, 95% CI 0.83 to 0.89) compared with residents of long-term care homes (Appendix 1, Supplemental Table 6, Supplemental Table 7).
Interpretation
We found that residents of retirement homes have high rates of hospital-based care. These older adults purchase health care services from their retirement home to support independent living, yet we found they consume more publicly funded hospital-based care and have substantially lower rates of primary care visits relative to residents of long-term care homes. Our findings contribute to ongoing policy debates about the provision and organization of universal primary and supportive care services in privately operated congregate care homes for older adults, and suggest that more coordinated models of primary and supportive health care may reduce episodic care use.
Variations in legislative and operating requirements for retirement homes affect rates of hospital-based care among these residents. 36–38 Some smaller cohort studies found that residents of retirement homes have higher rates of emergency department visits and hospital admissions than residents of long-term care homes and community-dwelling older adults.16,39 Our findings align with these studies and may suggest residents of retirement homes have higher needs for care that may not be fully met in an assisted-living setting.
We found that residents of retirement homes had the highest rates of ALC days, which suggests that the needs of some residents may exceed their capacity to procure, publicly or privately, the level and scope of care needed in their retirement home. Some of these residents may not be able to afford additional care from their retirement home, as rates for heavy care in Ontario can exceed $6000 per month.40 Nearly half of the residents of retirement homes lived in middle- and low-income neighbourhoods, and so the costs for additional and heavy care may be out of reach or unavailable for many of these residents.41–43 This underscores the need for equitable policies that reduce barriers to housing and health care for this population to curtail the incidence of ALC patient days that strain hospital resources.
We found that residents of retirement homes had substantially lower rates of primary care visits relative to residents of long-term care homes. Residents of long-term care homes commonly receive monthly capitated primary care through consistent primary care providers under contract by the home, but no similar model exists in retirement homes, nor is there a regulatory requirement for on-site or on-call physicians in Ontario or elsewhere.44 Our findings suggest that the implementation and expansion of similar medical models of care in retirement homes may be an important intervention to promote continuity of care and reduce rates of hospital-based care among this population.
Assisted-living markets in North America are rapidly expanding to accommodate the varying preferences of older adults for housing, health and social care.5,10–12,41,45,46 The growth and availability of beds in these homes outpaces that of long-term care homes,5,45 and this growth is likely attributed to fewer supply and regulatory requirements than in long-term care homes that encourage capital growth in response to real demand. The increased supply of retirement homes may suggest that some of these retirement homes are a growing substitute for a long-term care home.12,45 As an important link in the continuum of care settings for older adults, our data suggest retirement homes should be subject to oversight in keeping with the vulnerability of their residents.
Limitations
We conducted a secondary analysis of health system administrative data; as such, the possibility of misclassification bias and residual confounding could have influenced our results and interpretation. We were unable to accurately identify residents of retirement homes who did not receive home care services in licensed retirement homes with nonunique postal codes, which is estimated to represent as much as 10% of the population (i.e., about half of the total capacity in these homes). As there is no individual-level population register or reporting system for retirement homes, we could not validate our cohort; however, our cohort size is consistent with the most accurate point estimate of the population of older adults in retirement homes in Ontario,6 as well as with the presumed accuracy of other derived cohorts in common use.27,29,47 Furthermore, the lack of demographic outliers suggests high specificity, which is consistent with other derived cohorts.27,29,47
Conclusion
Residents of retirement homes are a unique population of older adults. Future research should examine with more granularity the reasons why residents of retirement homes visited emergency departments or were admitted to hospital to understand their needs for hospital-based care that may not be met in their retirement home.
Acknowledgements
The authors thank the Retirement Homes Regulatory Authority (in particular, Paul Pham, Adriane Castellino and Chloe Ma) for their support of this work.
Footnotes
Competing interests: Andrew Costa holds the Schlegel Chair in Clinical Epidemiology in Aging at McMaster University, which was established by a gift by the Schlegel family (who own and operate Schlegel Villages; a chain of long-term care and retirement homes). Andrew Costa and Susan Bronskill have received honoraria from the Canadian Institutes for Health Research Best Brains Exchange on Retirement Homes. Derek Manis was a member of the Board of Directors of The Justice Emmett Hall Memorial Foundation (2018–2021). Paula Rochon holds the RTOERO Chair in Geriatric Medicine at the University of Toronto. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Andrew Costa, Derek Manis, Jeffrey Poss, Aaron Jones and Ahmad Rahim led the design of the study and acquisition of data. Ahmad Rahim and Glenda Babe conducted the statistical analyses. Derek Manis and Andrew Costa led the interpretation of the data. Derek Manis drafted the manuscript. All of the authors contributed important intellectual content, interpreted the data, edited the manuscript, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This work was substantially supported by the Schlegel Chair in Clinical Epidemiology in Aging at McMaster University; the Juravinski Research Institute, in partnership with the St. Joseph’s Healthcare Foundation, McMaster University and the Hamilton Health Sciences Foundation; as well as partly by the Ontario Ministry of Health System Research Fund (2017-01097).
Derek Manis has received a Mitacs Accelerate Fellowship.
Data sharing: The data set from this study is held securely in coded form at ICES. While legal data-sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at https://www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full data set creation plan and underlying analytic code are available from the authors upon request, with the understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: Nathan Stall is an associate editor with CMAJ and was not involved in the editorial decision-making for this article.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and the Ministry of Long-Term Care. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information. The analyses, conclusions, opinions and statements expressed herein are solely those of the authors and do not reflect those of the funding or data sources; no endorsement is intended or should be inferred.
- Accepted May 5, 2021.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
References
In this issue

{kind=link}
Article tools






Jump to section
Related Articles
Cited By...
- No citing articles found.
More in this TOC Section
Similar Articles
Collections

