

Abstract
Background: Children are more susceptible to radiation-induced damage than adults, but little research has compared the risk of cancer after exposure to radiation during computed tomography (CT) among children at different ages. We aimed to explore the risk of intracranial tumours, leukemia or lymphoma among children, adolescents and young adults (aged < 25 yr) after radiation exposure from CT at or before the age of 18 years.
Methods: We conducted a nested, population-based case–control study using data from Taiwan’s publicly funded health care system. We identified participants younger than 25 years with newly diagnosed intracranial tumours, leukemia or lymphoma, from Jan. 1, 2000, to Dec. 31, 2013. We assigned 10 non-cancer controls for each case, matching by sex, date of birth and day of entry to the cohort. We considered CT scans received at or before the age of 18 years and 3 or more years before the index date (the date of cancer diagnosis for cases) as exposure. We used conditional logistic regression models and incidence rate ratios (IRRs) to estimate the relationship between risk of these cancers and CT radiation exposure.
Results: We identified 7807 cases and matched to 78 057 controls. Compared with no exposure, exposure to a single pediatric CT scan did not increase risk of intracranial tumours, leukemia or lymphoma. However, participants exposed to 4 or more CT scans had an elevated incidence (IRR 2.30, 95% confidence interval 1.43–3.71) of one of the cancer outcomes of interest. Receiving 4 or more CT scans at or before 6 years of age was associated with the highest risks of cancer, followed by ages 7–12 years and 13–18 years (p for trend < 0.001).
Interpretation: Exposure to a single CT scan was not associated with increased risks of subsequent intracranial tumours, leukemia or lymphoma among children; however, we observed increased cancer risks among those with 4 or more CT scans, especially among younger children. Although these cancers are uncommon, the findings of this study underscore the importance of prudent use of CT in the pediatric population.
The use of computed tomography (CT) in children has increased globally over the past several decades.1–3 In North America, the annual incidence of childhood CT scans plateaued in 2006, followed by a slow decline, but the rate of pediatric CT imaging in the United States and Canada was still higher in 2016 than in 2000.3
Although low-dose (< 500 milliGray) radiation does not cause immediate illness in humans, it inflicts damage to the genome and can induce oncogenesis.4–6 Preclinical cell and animal models have been proposed to illustrate the dose–response effect after low-dose radiation.4,5
Clinical studies have shown that exposure from diagnostic CT is associated with increased risk of cancer among both adults and children,7–13 and that children are more vulnerable to radiation than adults.14 However, studies comparing risk of cancer after CT exposure among children at different ages are limited and have reported conflicting conclusions.7–9,12 It remains unclear how CT exposure at different ages in childhood affects the risk of cancer. In addition, studies that focus on risk of cancer among young adults associated with radiation exposure in childhood are lacking. Compared with cancers among older people, cancers among young adults have shown similar manifestations to those in adolescents in terms of the type of cancer, treatment response and prognosis.15–17
Since head CT is the most common type of CT used for children,3 and hematopoietic tissues are the most radiosensitive,18 we sought to investigate whether childhood CT exposure (at or before age 18 yr) was associated with risks of intracranial tumours, leukemia, non-Hodgkin lymphoma and Hodgkin lymphoma among children, adolescents and young adults. We also sought to evaluate whether any incremental increases in risk of these cancers after pediatric CT would last from adolescence to early adulthood.
Methods
Study design and setting
We conducted a population-based, nested case–control study using the National Health Insurance (NHI) Research Database (NHIRD) in Taiwan, to evaluate the association of radiation exposure (by total number of CT scans, cumulative radiation doses and cumulative number of CTs received at different ages) with subsequent risk of intracranial tumour, leukemia, non-Hodgkin lymphoma and Hodgkin lymphoma.
The population of Taiwan is about 23 million, and the NHIRD contains the health records for all NHI beneficiaries.19 All newborns in Taiwan become beneficiaries of the single-payer NHI program at birth, along with foreign nationals who have established a registered domicile for at least 6 months and those with a regular employer.20
We reported this study according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist for case–control studies.21
Data source
The NHIRD contains deidentified health information for NHI beneficiaries, including demographic information, diagnoses and management of each medical visit.19 Under the NHI program, patients receiving therapies for cancer are eligible to be part of the Registry for Catastrophic Illness (a subset of the NHIRD) to reduce copayments.19,22
The NHI stipulates that health care providers attach reports written by board-certified specialists before reimbursement for procedure claim, including imaging;20 therefore, the NHIRD records only procedures that are actually performed. The NHI employs multiple audits to ensure the appropriateness of claims for medical services, and its accuracy and completeness have been shown in several validation studies.19,23
Cases, controls and matching
For our base cohort, we extracted data on all NHIRD beneficiaries who were younger than 25 years from Jan. 1, 2000, to Dec. 31, 2013.
To form our case cohort, we extracted cases of intracranial tumours (grades I–IV under World Health Organization classification),24 leukemia, non-Hodgkin lymphomas or Hodgkin lymphomas that were newly diagnosed during the study period. We used codes from the International Classification of Diseases, Ninth Revision (ICD-9) to identify these cases from the Registry of Catastrophic Illness; a previous study reported that this approach had a positive predictive value of 94%.25 We further used incidence density sampling to randomly select non-cancer controls from the base cohort.26
Before matching, we excluded patients with any malignant disease diagnosed before the study period. We also excluded those with cancer-predisposing conditions that were potential confounders for our exposure of CT imaging.27 For example, children with Down syndrome, who have an increased risk of leukemia, may receive CT scans for cardiac defects, and children with immunodeficiency may be imaged for recurrent infections.28–30
We identified patients with cancer-predisposing conditions using at least 1 inpatient or 3 outpatient claims.31,32 The relevant ICD-9 codes are listed in Appendix 1, Supplementary Table 1 and Table 2, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.221303/tab-related-content. Finally, we excluded patients with missing data (i.e., unreported sex, date of birth or cohort entry date).
We pooled the remaining participants to form an at-risk population. In this at-risk population, when 1 cancer case was diagnosed during the study period (index case), we randomly assigned up to 10 participants free from cancer at the index diagnosis date as controls, to form a risk set with matched sex, date of birth (± 1 yr), and cohort entry date (± 1 yr).26,33 We repeated this process until all cases had been matched. We excluded risk sets when fewer than 5 controls could be assigned to a case. We defined the exposure period as the period from cohort entry to 3 years (the lag period) before the index date (i.e., the index case’s date of cancer diagnosis). The length of follow-up and the exposure period of the index case and the assigned controls were equivalent.
Exposure
Exposure was CT-associated radiation received at or before the age of 18 years, quantified by the cumulative number of CT scans7–11 and the organ-specific cumulative dose.13 Given that some cancer-related symptoms would prompt CT, we considered exposure to include only CT scans performed 3 or more years before the index date. A descriptive analysis from the United Kingdom found that the mean interval between symptom onset and diagnosis of low-grade pediatric brain tumours was 28.2 weeks.34 Other studies have shown that intracranial tumours associated with radiotherapy in childhood occurred 3–5 years after treatment.35,36 An increased incidence of hematologic malignant diseases was observed 2 years after occupational radiation exposure among adults.37 Therefore, we considered a 3-year lag period to be appropriate to minimize reverse causation bias and avoid improperly excluding cases with malignant diseases relating to radiation from CT scans.
Radiation causes direct damage to tissues and the organ-specific radiation dose varies in different CT types.4,5,38–41 Dosage calculation for CT exposure was done by consensus of a pediatric hematologist and oncologist (W.H.W.) and a radiologist at Changhua Christian Hospital. We used the cumulative radiation dose to the brain to assess the risk of intracranial tumour and the cumulative dose to red bone marrow for leukemia and lymphoma. We quantified effective radiation doses to the brain and red bone marrow based on sex, age, CT type and radiation dosimetry data, as reported by Gao and colleagues40 (Appendix 1, Supplemental Table 3). Gao and colleagues40 combined patient-specific CT parameters with various pediatric-sized phantoms (objects that mimic human tissue) to estimate the organ-absorbed radiation dose. As we were unable to find studies of radiation doses for CTs of extremities, we considered the radiation dose from these procedures to be 0. We divided the calculated cumulative organ-specific CT dosage into quintiles to assess the relationship between total radiation dosage and risk of cancers.
We determined the type of each CT scan according to the corresponding ICD-9 code, if not recorded in the NHIRD database. We also extracted data on other high-radiation procedures using claims for cardiac catheterizations and common nuclear medicine procedures.42,43
Statistical analysis
We calculated the incidence rate ratio (IRR) and built conditional logistic regression models to assess the adjusted odds ratios (ORs) between groups with and without CT exposure. As usage of CT scans increased over our investigation period,2 we adjusted the ORs for the calendar year of cohort entry as a linear variable. We also adjusted for family income (as a linear variable) and degree of urbanization of place of residence (as a categorical variable), as these variables are associated with leukemia among children.44–46
We used the 1-sided Cochran–Armitage test to investigate the relationship between age at CT exposure (categorized as ≤ 6, 7–12 and 13–18 yr) and cancer risk. We applied the Fisher exact test for categorical variables.
We completed all statistical analyses using SAS statistical software version 9.4 (SAS Institute).
Sensitivity analyses
We conducted sensitivity analyses using lag periods of 1–4 years and including the total number of other high-radiation procedures as a covariable in the model.42,43
We recomputed the radiation organ dose using data from Kim and colleagues,41 derived from radiological technician surveys and from realistic, normal-stature, pediatric phantoms ranging in age and body size (Appendix 1, Supplementary Methods and Table 4). We also reassessed the relationship between cumulative organ-specific CT dosage (by quintiles) and risk of cancers using these data.
We noted that participants in the top 2% of cumulative organ-specific doses had received 4 or more CT scans. Therefore, we conducted additional sensitivity analyses for this high-exposure group to evaluate the associated cancer risks, initially using doses calculated with data from Gao and colleagues40 and then with data from Kim and colleagues.41
Ethics approval
This study was approved by the Taipei Medical University – Joint Institutional Review Board (no. N201602055).
Results
In total, we initially identified 8055 patients with intracranial tumours, leukemia, non-Hodgkin lymphoma or Hodgkin lymphoma diagnosed during the study period. We excluded 153 patients with malignant diseases diagnosed before the study period, 72 with cancer-predisposing conditions and 19 with missing information (Figure 1). None of the patients with missing information had CT exposure. Demographic characteristics of the remaining 7807 patients and 78 057 matched controls are summarized in Table 1.

Flow chart of case and control group selection. Note: NHIRD = National Health Insurance Research Database.
Participant characteristics
The proportion of patients exposed to other high-radiation procedures was similar in the case and control groups (Appendix 1, Supplemental Table 5).
Risk of cancer by number of scans
Compared with no exposure, exposure to a single pediatric CT scan did not increase subsequent cancer risk (Table 2). Participants who received 2–3 CT scans had an increased risk of intracranial tumour (adjusted OR 2.36, 95% confidence interval [CI] 1.40–3.97), but not leukemia, non-Hodgkin lymphoma or Hodgkin lymphoma. Participants who received 4 or more CT scans had a higher risk of intracranial tumour (adjusted OR 9.01, 95% CI 2.89–28.11), leukemia (adjusted OR 4.80, 95% CI 1.79–12.84) and non-Hodgkin lymphoma (adjusted OR 6.76, 95% CI 1.91–23.96), but not Hodgkin lymphoma.
Adjusted odds ratios for intracranial tumours, leukemia and lymphomas related to the number of computed tomography scans
The IRR of participants with one of the cancer outcomes of interest receiving 4 or more CT scans was 2.30 (95% CI 1.43–3.71) relative to nonexposed participants (Table 3).
The incidence rate ratio for intracranial tumour, leukemia or lymphomas according to computed tomography exposure status
Cancer risk by cumulative radiation dose
Participants in the top quintile of cumulative brain radiation dose had a significantly higher risk of intracranial tumour compared with nonexposed participants (adjusted OR 3.61, 95% CI 1.93–6.75) (Table 4). We did not observe this association between the cumulative dose of radiation to red bone marrow and risk of hematologic malignancies.
Adjusted odds ratios for intracranial tumours, leukemia and lymphomas related to the cumulative organ-specific dose from computed tomography scans, estimated using radiation dosimetry from Gao and colleagues40
Cancer risk by age of exposure
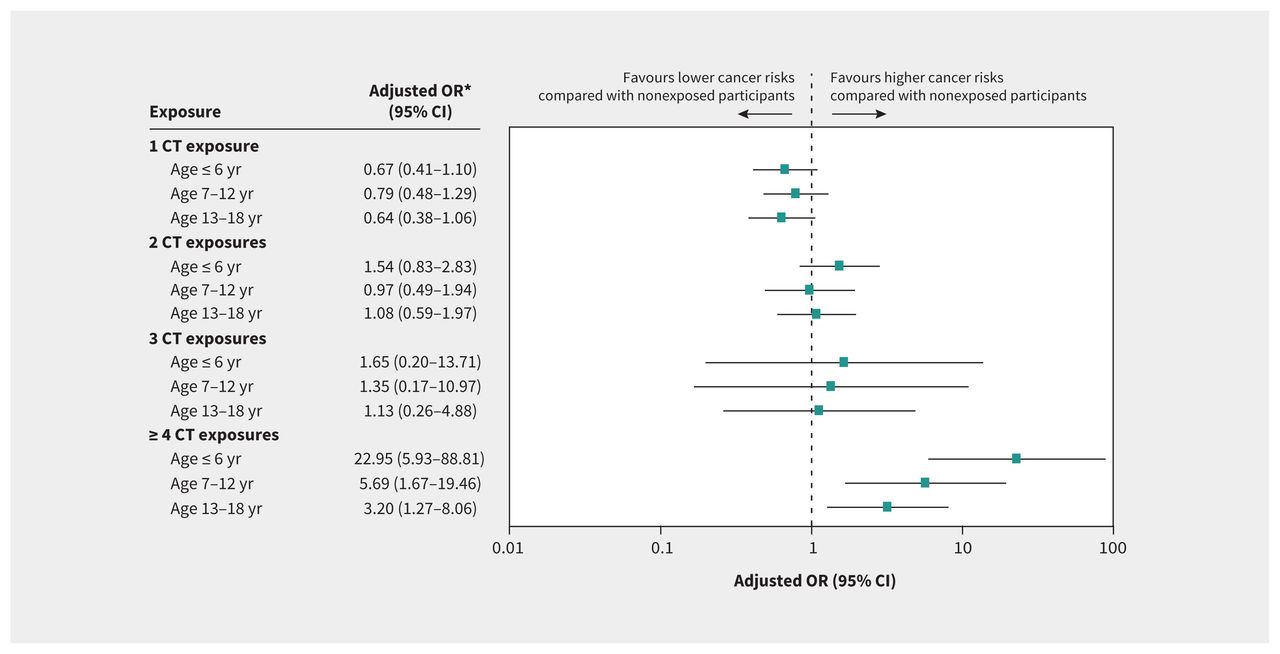
Participants who received 4 or more CT scans at or before the age of 6 years had the highest risk of cancer, followed by those aged 7–12 years and those aged 13–18 years (Figure 2). The correlation was statistically significant (p for trend < 0.001).

{kind=link}
{kind=link}
Forest plots for adjusted odds ratios (ORs) of intracranial tumours, leukemia, non-Hodgkin lymphoma and Hodgkin lymphoma by cumulative number of computed tomography (CT) scans among children at different ages (p value for trend < 0.001 for ≥ 4 CT exposures by Cochran–Armitage test). *Adjusted by the year of cohort entry, annual family income (both as linear variables) and degree of urbanization (as a categorical variable). Note: CI = confidence interval.
Sensitivity analyses
Using a 1- or 2-year lag period, we found a stronger association between risk of intracranial tumour and increasing CT exposure than in the primary analysis. This association also held with a 4-year lag period (Appendix 1, Supplemental Table 6).
We included the number of high-radiation procedures in our full model and the results remained consistent (Appendix 1, Supplemental Table 7).
The re-estimated organ-absorbed radiation dose using data from Kim and colleagues41 still showed an association between an elevated cumulative dose of radiation and risk of intracranial tumour and of leukemia. Increased cumulative radiation did not significantly increase the risk of non-Hodgkin lymphoma or Hodgkin lymphoma (Appendix 1, Supplemental Table 8).
Using data from Gao and colleagues40 and from Kim and colleagues,41 the highest 2% of cumulative organ-specific doses (> 98th to ≤ 100th percentile) was associated with elevated risk of intracranial tumour, leukemia and non-Hodgkin lymphoma, but not Hodgkin lymphoma (Table 4 and Appendix 1, Supplemental Table 8).
Interpretation
We found that receipt of a single CT scan at or before 18 years of age was not associated with increased risk of intracranial tumours, leukemia, non-Hodgkin lymphoma or Hodgkin lymphoma, to the age of 25 years. However, children who had received 4 or more CT scans at or before 18 years of age had a 2.3-fold increase in the incidence of these cancers compared with those without exposure. It is important to note that these neoplasms are uncommon among children, with an incidence of 15–40 cases per million in Taiwan over a 15-year period from 1996 to 2010.47
The associated risk of cancer we observed was highest among children who had received 4 or more CT scans at or before 6 years of age, followed by those aged 7–12 years and adolescents aged 13–18 years (Figure 2), suggesting that younger children are more vulnerable to radiation than older children. However, this finding should be interpreted cautiously, as the risks may be overestimates because of residual confounding and the low number of participants in high-radiation groups.48
Several studies have evaluated the association between pediatric neoplasms and CT scans among children of different ages, but the results were inconclusive.7–9,12 These studies focused on the age of the first CT exposure rather than the cumulative number of CT scans at different ages.
The positive relationship between the cumulative organ-specific dose of radiation and the risk of intracranial tumour and leukemia that we observed has also been seen in other studies,7,8 but the association between childhood CT radiation and lymphoma is still unclear. For Hodgkin lymphoma, the lack of association we observed across the cumulative number of CT scans was consistent with earlier reports,14,49 except for 1 Australian study.8 For non-Hodgkin lymphoma, Li and colleagues12 did not find an association between 2 or more CT scans and non-Hodgkin lymphoma, in contrast to the association we observed for those with exposure to 4 or more CT scans. This discrepancy may have been owing to the different CT protocols used in various countries.50 Further studies with a standard scanning protocol might produce more conclusive results. It should be noted that the association we observed between non-Hodgkin lymphoma and higher numbers of scans did not hold when the data were reanalyzed by increasing quintiles of radiation exposure to red bone marrow.
When human cells are exposed to low-dose radiation, small DNA breaks are generated and mended by intrinsic DNA repair processes. Therefore, low-level CT exposure appears not to be carcinogenic and animal models have suggested that it may even protect cells from mutagenesis.4,5 However, when cumulative DNA damage stimulated by recurrent radiation exposure exceeds DNA repair abilities, the risk of carcinogenesis rises.4,5 This mechanism explains the dose–response relationship between the cumulative organ-specific dose of radiation and the risk of cancers observed in our study and in previous studies.7–11
The large population of this nationwide cohort is one of the major advantages of this study. In addition, we matched cases and controls on the calendar year of cohort entry and the duration of the exposure period to ensure equal opportunity for CT exposure, avoiding a time-window bias.51 Furthermore, we excluded patients with cancer-predisposing conditions to avoid related confounding.
Our work reinforces the importance of radiation protection strategies, addressed by the International Atomic Energy Agency.52 Unnecessary CT scans should be avoided, and special attention should be paid to patients who require repeated CT scans.52 Parents and pediatric patients should be well informed on risks and benefits before radiological procedures and encouraged to participate in decision-making around imaging.53
Limitations
Given the observational study design, our results should not be interpreted as causal; rather, our study assesses the association between radiation exposure and subsequent risks of cancer.
Despite our efforts to control for potential confounders, residual confounding may still be present. For example, data on some risk factors for cancer — such as smoking, alcohol consumption, obesity (i.e., body mass index) and exposure to pesticides or phthalate-containing medications — were lacking in the NHIRD database.54–56 About 10% of patients with childhood or adult cancers have germline genomic alterations for which we had no data.57–59 We were unable to eliminate the influence of high-radiation procedures completely; however, the effect should be minimal because the misclassification would have been non-differential between cases and controls.
Although we adopted a longer lag period than those defined in most of the previous literature,8–12 we are unable to eliminate the possibility of reverse causality. In addition, more than 10% of participants were born after 2005, which led to a short follow-up time for neoplasm development.
Because of a lack of local data on CT radiation dosimetry, errors may have occurred in our calculation of the organ-absorbed dose of radiation. Furthermore, the precision of CT claim data in the NHIRD has not yet been validated, despite previous publications adopting the same approach.9,12 Similarly, the code definitions we used for each individual cancer type have not been validated in the NHIRD, although this approach has been shown to have a high positive predictive value for all cancers as a group in this database.25 The algorithm we used to identify cancer-predisposing conditions has not been validated but is a common approach used by researchers extracting data from the NHIRD.9
Importantly, the small numbers of participants in the high-radiation groups reduced our ability to detect potential effects of high radiation doses. The wide OR ranges found in these analyses indicate that these results should be interpreted with caution, as the OR may be inflated because of sparse data.48
We excluded 19 (0.2%) cases with missing data, but the impact on our results was likely small because none of them had CT scans.
Conclusion
This study found that exposure to a single CT scan at or before 18 years of age was not associated with the development of subsequent intracranial tumours, leukemia, non-Hodgkin lymphoma and Hodgkin lymphoma during childhood, adolescence and early adulthood. Children who received multiple CT scans had higher risks of intracranial tumours, leukemia and non-Hodgkin lymphoma, but not Hodgkin lymphoma. Younger children appeared vulnerable to cancer risks associated with repeated CT exposure. Although these tumours are uncommon, these results indicate that judicious CT usage and radiation-reducing techniques should be advocated.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
Contributors: Yu-Hsuan Shao conceived and designed the study. All of the authors the acquisition, analysis, and interpretation of data. Wei-Hao Wang drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: The authors received no specific funding for this work.
Data sharing: Data are available from the Health and Welfare Data Center published by the Ministry of Health and Welfare. Given legal restrictions imposed by the government of Taiwan in relation to the Personal Information Protection Act, data cannot be made publicly available. Requests for data can be sent as a formal proposal to the Health and Welfare Data Center Administration (https://dep.mohw.gov.tw/DOS/cp-5119-59201-113.html).
- Accepted March 21, 2023.
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/