

Abstract
BACKGROUND: Australia introduced tamper-resistant controlled-release (CR) oxycodone in April 2014. We quantified the impact of the reformulation on dispensing, switching and poisonings.
METHODS: We performed interrupted time-series analyses using population-representative national dispensing data from 2012 to 2016. We measured dispensing of oxycodone CR (≥ 10 mg), discontinuation of use of strong opioids and switching to other strong opioids after the reformulation compared with a historical control period. Similarly, we compared calls about intentional opioid poisoning using data from a regional poisons information centre.
RESULTS: After the reformulation, dispensing decreased for 10–30 mg (total level shift −11.1%, 95% confidence interval [CI], −17.2% to −4.6%) and 40–80 mg oxycodone CR (total level shift −31.5%, 95% CI −37.5% to −24.9%) in participants less than 65 years of age but was unchanged in people 65 years of age or older. Compared with the previous year, discontinuation of use of strong opioids did not increase (adjusted hazard ratio [HR] 0.95, 95% CI 0.91 to 1.00), but switching to oxycodone/naloxone did increase (adjusted HR 1.54, 95% CI 1.32 to 1.79). Switching to morphine varied by age (p < 0.001), and the greatest increase was in participants less than 45 years of age (adjusted HR 4.33, 95% CI 2.13 to 8.80). Participants switching after the reformulation were more likely to be dispensed a tablet strength of 40 mg or more (adjusted odds ratio [OR] 1.40, 95% CI 1.09 to 1.79). Calls for intentional poisoning that involved oxycodone taken orally increased immediately after the reformulation (incidence rate ratio (IRR) 1.31, 95% CI 1.05–1.64), but there was no change for injected oxycodone.
INTERPRETATION: The reformulation had a greater impact on opioid access patterns of people less than 65 years of age who were using higher strengths of oxycodone CR. This group has been identified as having an increased risk of problematic opioid use and warrants closer monitoring in clinical practice.
Canada, the United States and Australia have the highest per capita opioid consumption in the world.1 In Australia, there has been a 15-fold increase in opioid use between 1992 and 2012,2 and Australia now has the second largest per capita consumption of oxycodone.3 This has been driven by approvals and subsidies for an increasing number of chronic noncancer pain conditions,4,5 despite a lack of evidence of long-term effectiveness.6–8 This rise has been accompanied by increases in nonmedical use, diversion and opioid-related harms.2,9–13 Injection and snorting of oxycodone are common;13–15 extended- or controlled-release tablets are crushed or dissolved to accelerate their effect.16 To curb this activity, tamper-resistant formulations have come to market; they form a viscous gel when crushed and mixed with water, making them harder to snort or inject. Importantly, tamper-resistant formulations do not avert opioid dependence as they can still be misused when taken orally,17,18 the most common route of administration in oxycodone-related deaths.16,19 Further, the tamper-resistant properties can be circumvented to allow injection.20
In April 2014, all controlled-release (CR) oxycodone in Australia was replaced with a tamper-resistant formulation. The US introduced tamper-resistant oxycodone in 2010 followed by Canada in 2012. To date, studies assessing the impact of this formulation have focused primarily on the US market, showing reductions in overall oxycodone use and oxycodone-related harm,21–24 but increased use of heroin.25,26 Early evidence for Australia has suggested that the tamper-resistant formulation resulted in decreased sales of the 40–80 mg strengths, and a reduction in oxycodone injection.27
However, there are no definitive studies using person-level data in Australia or internationally that have explored the extent to which individuals taking oxycodone CR have switched to other opioids. The purpose of this study was to determine whether the reformulation of oxycodone CR led to a change in use of oxycodone CR and opioid-related harms. We used an interrupted time series analysis and a retrospective cohort study to quantify the impact of the reformulation on dispensing of high-strength oxycodone CR; ending use of all strong opioids; switching from oxycodone CR to other strong opioids; and calls for intentional poisoning that involved oxycodone and other opioids.
Methods
On Apr. 1, 2014, oxycodone CR in Australia was replaced with a tamper-resistant formulation. On Dec. 1, 2014, a generic nontamper-resistant formulation was also subsidized, and we were unable to distinguish the 2 formulations in our data. The nontamper-resistant formulation was not commonly sold;28 nonetheless, to avoid bias because of introduction of this product, we focused on the 8 months after the reformulation and before the subsidy of the generic formulation.
Data sources
Data from the Pharmaceutical Benefits Scheme
In Australia, all residents are entitled to subsidized access to prescribed medicines through the Pharmaceutical Benefits Scheme. We used dispensing records from the Pharmaceutical Benefits Scheme (July 2012 to November 2016) for a representative 10% random sample of people eligible for the scheme, about 2.5 million people.29 The data do not contain medicines dispensed in public hospitals or privately dispensed medicines; however, less than 10% of oxycodone is privately dispensed.30,31
We included all formulations of subsidized strong opioids, including buprenorphine, fentanyl, hydromorphone, methadone, morphine, immediate-release (IR) oxycodone, oxycodone CR, oxycodone/naloxone and tapentadol. Because we did not have data on opioids used to treat opioid dependence (i.e., methadone and buprenorphine/naloxone), these were excluded.
The available oxycodone CR strengths were 5, 10, 15, 20, 30, 40 and 80 mg. The 5 mg strength was withdrawn from the market on Apr. 1, 2014; therefore, we excluded all 5-mg strengths of oxycodone IR, oxycodone CR and oxycodone/naloxone, because we could not separate switching to or from this strength as a result of the withdrawal versus the reformulation. Higher strengths of oxycodone CR were also more commonly misused32 and were the main target of the reformulation.27
New South Wales Poisons Information Centre
The New South Wales Poison Information Centre provides advice to health care professionals and members of the public 24 hours a day; it receives 50% of Australia’s poisoning calls (about 100 000 per year).33 We used data from the New South Wales Poison Information Centre (July 2012 to December 2016) to identify changes in calls associated with oxycodone, oxycodone/naloxone, morphine, other opioids and heroin.
Statistical analysis
Dispensing of oxycodone CR at the population level
Using dispensing data, we summed oxycodone CR dispensings by calendar month stratified by age (< 65 and ≥ 65 yr) and tablet strength (10–30 and 40–80 mg). We estimated population-level dispensing rates using the mid-year Australian population.34 We used stratification by age because we hypothesized that the impact would be greater in participants less than 65 years of age, who are more likely to engage in aberrant opioid-related behaviours.35
We used an interrupted time series analysis to assess the impact of the reformulation on dispensing. To estimate percent change, we modelled the natural log of dispensings. To account for seasonality, trends and autocorrelation, we used an autoregressive integrated moving average (ARIMA) model, using the Box–Jenkins method.36,37 We tested different forms of the impact of the reformulation, including temporary change, immediate level shift and gradual level shift. A level shift is a permanent change in the mean level of dispensing.38 We also included lagged effects if appropriate.
Discontinuing use of opioids and switching
To quantify discontinuation of use of opioids and switching, we identified a cohort of patients who were dispensed oxycodone CR within 60 days before Apr. 1, 2014 and a historical control cohort of patients dispensed oxycodone CR within 60 days before Apr. 1, 2013. We identified switching events between Apr. 1 and Nov. 30 in 2013 and 2014; we counted only the first event. A switch occurred if an individual stopped using oxycodone CR (no dispensing for ≥ 60 d), was dispensed a new strong opioid within 60 days of the last dispensing of oxycodone CR and the new opioid had not been dispensed before Apr. 1. We also identified the discontinuation of use of all strong opioids (no dispensing for ≥ 60 d).
To characterize our 2 cohorts (2013 and 2014), we measured several covariates in the 90 days before Apr. 1, including age and sex; oxycodone CR utilization, specifically number of dispensings and highest tablet strength dispensed (10–30 or 40–80 mg); the number of unique nonopioid medicines dispensed as a proxy for comorbidity;39,40 and co-dispensing of medicines with sedative properties within 30 days of a dispensing of oxycodone CR, because these drugs are commonly present in cases of oxycodone overdose.19 The latter category includes antipsychotics, benzodiazepines, serotonin and noradrenaline reuptake inhibitors, and tricyclic antidepressants. Although pregabalin is also in this category, it was subsidized for only part of the study period, and, therefore, we excluded it. We compared cohorts using standardized differences.41
To compare discontinuation of use and switching after the reformulation with that during the control period, we conducted a competing risks survival analysis.42 Death and switching to different opioids were competing risks. We adjusted standard errors for correlation within individuals who appeared in both cohorts. All models for competing risks were adjusted for the covariates described above to account for differences in users of oxycodone CR in 2013 and 2014. To test for a differential impact by age, we included an interaction term between cohort and age group (< 45, 45–64, 65–79 and ≥ 80 yr); if it was significant (p < 0.05), we presented the age-specific hazard ratios (HRs); if not, we included age as a covariate only.
Finally, we compared participants who switched in 2014 to people who switched in 2013. We examined the association between each of the covariates described above and switching in 2014 versus 2013. Because we were interested only in comparing characteristics, we conducted separate analyses for each variable adjusted for age only. We used generalized estimating equation logistic regression and repeated measures to adjust for correlation within individuals and included an interaction term with age. Owing to small numbers, we collapsed the age groups into less than 65 years, and 65 years and older.
Intentional poisoning calls
We summed all calls to the New South Wales Poison Information Centre that involved opioids or heroin and resulted from an intentional poisoning (i.e., deliberate self-poisoning, recreational use or intentional misuse) for each quarter. We excluded accidental exposures and adverse reactions. Because there was no significant autocorrelation in the data, we used a segmented Poisson regression. For calls involving oxycodone, oxycodone/naloxone, morphine and other opioids, we modelled the impact both unadjusted and adjusted for the total oral morphine equivalents dispensed per quarter to account for changes in use over time, by including the log of the oral morphine equivalents dispensed in milligrams43 as an offset in the model.
All analyses were performed with SAS version 9.3 and Stata 14.
Ethics approval
This study received approval from the New South Wales Population and Health Services Ethics committee (2013/11/494) and the Sydney Children’s Hospital Network Human Research Ethics Committee (LNR/16/SCHN/44). The Australian Government Department of Human Services External Request Evaluation Committee approved access to data from the Pharmaceutical Benefits Scheme.
Results
Dispensing of oxycodone CR at the population level
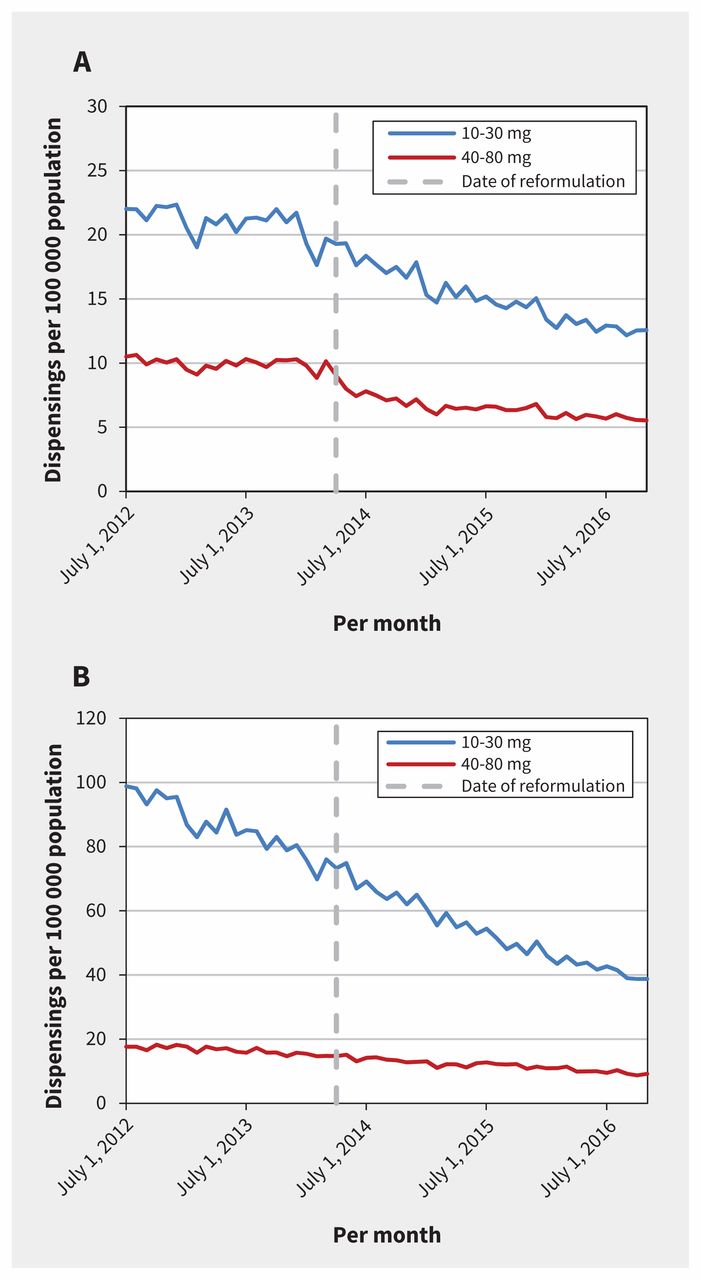
In our sample cohort, 36 528 participants had at least 1 dispensing for oxycodone CR (≥ 10 mg) during the study period; the median age was 57 (interquartile range [IQR] 46–70) years and 56% of participants were female. The impact of the reformulation was best modelled using a gradual, permanent level shift that occurred over several months (Table 1). Among people < 65 years, before the reformulation, dispensing of 10–30 mg strengths was decreasing slightly among participants less than 65 years of age, while dispensing of 40–80 mg strengths was stable (Figure 1). After the reformulation, dispensing of both 10–30 and 40–80 mg strengths decreased gradually before levelling off, for a total level shift of −11.1% (95% CI −17.2% to −4.6%) and −31.5% (95% CI− 37.5% to −24.9%), respectively. In participants 65 years of age and older, there were no significant changes after the reformulation.
Change in dispensing of controlled-release oxycodone after reformulation, by participant age and formulation strength

{kind=link}
Monthly dispensing of oxycodone CR stratified by strength of drug and age of participants after reformulation of oxycodone CR (Apr. 1, 2014). (A) Dispensing per 100 000 population per month stratified by tablet strength in participants aged less than 65 years. (B) Dispensing per 100 000 population per month stratified by tablet strength in participants aged 65 years or more. Note: CR = controlled release.
Discontinuing use of opioids and switching
The cohorts of participants who were dispensed oxycodone CR in the 60 days before the reformulation (n = 6195) and during the same period in 2013 (n = 6702) were similar, with standardized differences ranging from −0.05 to 0.04 (Table 2).
Characteristics of participants who were dispensed controlled-release oxycodone before introduction of the tamper-resistant formulation (2014) and during the control period (2013) in Australia
Overall, we observed little change in discontinuation of use after the reformulation compared with 2013 (HR 0.95, 95% CI 0.91 to 1.00) (Table 3, Table 4). Because we found a significant interaction by year and age for switching to morphine (p < 0.001), we present age-specific results for this outcome. Participants less than 65 years of age were more likely to switch to morphine after the reformulation, particularly those who were less than 45 years of age (HR 4.33, 95% CI 2.13 to 8.80), whereas there was an increase in switching to oxycodone/naloxone in participants of all ages (HR 1.55, 95% CI 1.32 to 1.80).
Participants who discontinued use of opioids or switched opioids in the 8 months after Apr. 1, 2014, compared with the control group (2013), stratified by age group
Discontinuation of use of opioids and switch to other opioids in the 8 months after Apr. 1, 2014, compared with 2013
When we compared participants who switched opioids in 2014 and 2013, we observed a significant interaction between age group (< 65 and ≥ 65 yr) and sex (p = 0.04), the number of dispensings of oxycodone CR before Apr. 1 (p = 0.046) and the number of nonopioid medications dispensed (p = 0.03). In participants who were less than 65 years of age and male sex, a greater number of dispensings of oxycodone CR and fewer nonopioid medications were associated with switching in 2014 (Table 5). Overall, dispensing of a higher strength was also associated with switching in 2014.
Characteristics of participants who switched in 2014 (n = 983) compared with participants who switched in 2013 (n = 794)
Intentional poisoning calls
After adjusting for the total oxycodone CR oral morphine equivalents dispensed, calls for injected and orally administered oxycodone were stable before the reformulation (Table 6); after the reformulation, there was a level shift in the number of calls about orally administered oxycodone (incidence rate ratio [IRR] 1.31, 95% CI 1.05 to 1.64), but there was no change in calls about injected oxycodone. There were no changes in calls involving morphine, other opioids or heroin.
Number of poisoning calls before and after reformulation
Interpretation
Our study reveals patterns of ending use of and switching of opioids at the person level after introduction of tamper-resistant oxycodone CR. Our findings suggest that the observed decline in dispensing of higher-strength oxycodone CR in participants less than 65 years of age may be due to an increase in switching to other strong opioids, chiefly morphine, rather than an increase in ending use. This is of concern because it suggests that people may be seeking out opioids without tamper-resistant properties; however, as with all observational studies, we could not establish a causal relationship between the reformulation and the outcomes, and can report only associations.
Furthermore, despite the reduction in dispensing, we saw no decrease in poisonings associated with injectable oxycodone, the main target of the reformulation. We did observe a small increase associated with orally administered oxycodone, a possible consequence of tamper-resistant formulations not deterring abuse of oral formulations. However, the increase in switching to morphine does not appear to have led to an increase in morphine poisonings.
Switching to oxycodone/naloxone also increased after the reformulation; as oxycodone/naloxone has abuse-deterrent properties and causes withdrawal symptoms if injected,44 switching to this formulation is unlikely to be related to misuse, but could be a result of its increasing popularity as a substitute for oxycodone CR since its subsidization in 2011.4 Patients and prescribers may have seen the reformulation as an opportunity to switch.
Our findings are consistent with an Australian study of the short-term impact of the reformulation that found a reduction in sales of higher strengths of oxycodone CR, which are more commonly diverted and injected.27 Similar reductions have been found in the US;22,26 however, these studies did not examine person-level changes. In contrast to the US but consistent with Australian data in sentinel populations of people who inject drugs,27 we did not observe any increase in heroin poisonings; however, the New South Wales Poison Information Centre only receives a small number of calls relating to heroin use.
Given the limitations of our data, we can only speculate on the reasons for increased switching to morphine; nonetheless, in a US survey of 244 people in drug treatment programs, a third of respondents reported switching to other drugs after the reformulation in 2010.21 Morphine, which is not tamper-resistant, is commonly consumed and injected by people who have reported tampering with opioids in Australia,32 and is a logical substitute for people who misuse oxycodone. Respondents in the survey also reported switching from injection and snorting of oxycodone to swallowing, which may explain our observed increase in oral poisonings.
Limitations
We had no clinical information or the indication for prescribing, which potentially could have identified appropriate and inappropriate use, and we are missing several important covariates associated with misuse, such as socioeconomic status. We also cannot determine the reason for switching and what proportion of participants (if any) switched for reasons of misuse. The findings about poisonings should also be interpreted with caution: these data may not be representative of overdoses in the community, because many poisonings would not result in a call to the New South Wales Poison Information Centre. Thus, these results should be confirmed using other data sources. We also had to limit our analysis to tablet strengths of 10 mg or more only because of the withdrawal of the 5-mg strength of oxycodone CR; however, 5-mg oxycodone is rarely injected and therefore, is not a target of this intervention.27 In addition, a generic nontamper-resistant formulation of oxycodone was subsidized in December 2014. Although not commonly dispensed and, thus, unlikely to have had a major impact,28 the decrease in dispensing of oxycodone CR seems to level off around this time, and we cannot rule out that this was partly influenced by the availability of this generic formulation.
Conclusion
Although dispensing of oxycodone CR among participants less than 65 years of age decreased after the reformulation, we did not find an increase in ending use of strong opioids in parallel with an increase in switching to other nontamper-resistant strong opioids. Participants who switched after the reformulation were more likely to be less than 65 years, male and had higher tablet strengths dispensed more frequently; this population was identified previously as having increased risk of problematic opioid use and may warrant closer monitoring in clinical practice.
Acknowledgement
The authors thank the Australian Government Department of Human Services for providing the data.
Footnotes
Competing interests: Briony Larance and Louisa Degenhardt received untied investigator-driven educational grants from Reckitt Benckiser for postmarketing surveillance studies of buprenorphine–naloxone tablets and film, development of an opioid-related behaviour scale and a study examining the uptake of opioid substitution therapy among chronic noncancer pain patients; from Indivior for studies of buprenorphine depot in community treatment and prison settings; and from Mundipharma for postmarketing surveillance studies of Reformulated OxyContin. Briony Larance, Louisa Degenhardt and Rose Cairns received an untied investigator-driven educational grant from Seqirus for postmarketing surveillance studies of tapentadol. These funders played no role in the design, conduct or interpretation of these studies’ findings, and there were no restrictions placed on publication. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Andrea Schaffer, Sallie-Anne Pearson, Nicholas Buckley, Briony Larance, Louisa Degenhardt and Timothy Dobbins contributed to the design of the study and interpretation of the data. Rose Cairns acquired the data and contributed to the interpretation of the data. Andrea Schaffer analyzed the data and drafted the manuscript. All of the authors critically revised the manuscript for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This research is supported, in part, by the National Health and Medical Research Council (NH MRC) Centre of Research Excellence in Medicines and Ageing (ID 1060407). Andrea Schaffer, Briony Larance and Louisa Degenhardt are supported by the NH MRC (IDs 1074924, 1041472, 1073858). The National Drug and Alcohol Research Centre at the University of New South Wales is supported by funding from the Australian Government under the Substance Misuse Prevention and Service Improvements Grant Fund. The study funders were not involved in the study. All of the authors performed the research independent of the funders.
- Accepted January 9, 2018.