

Influenza immunization among Canadian health care personnel
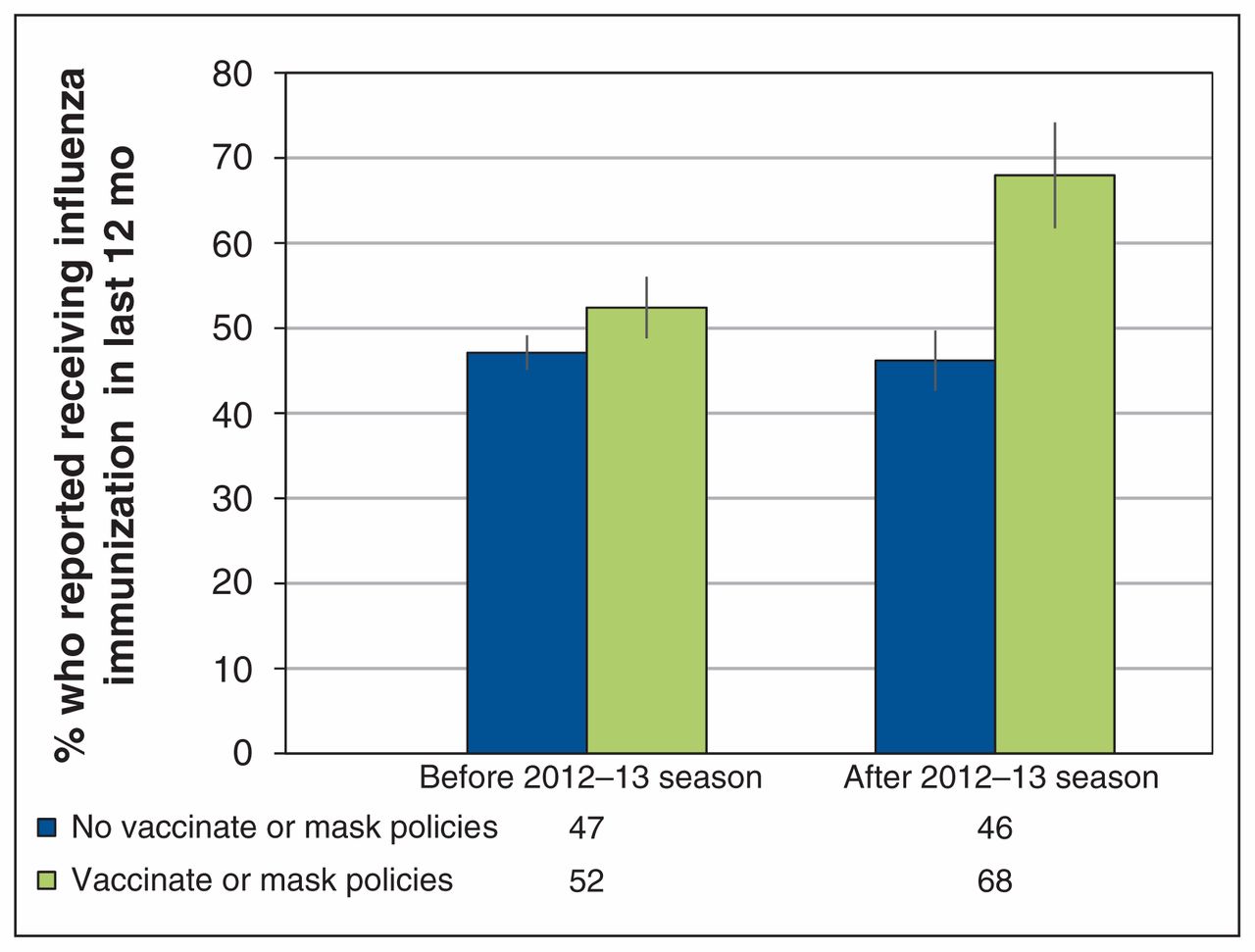
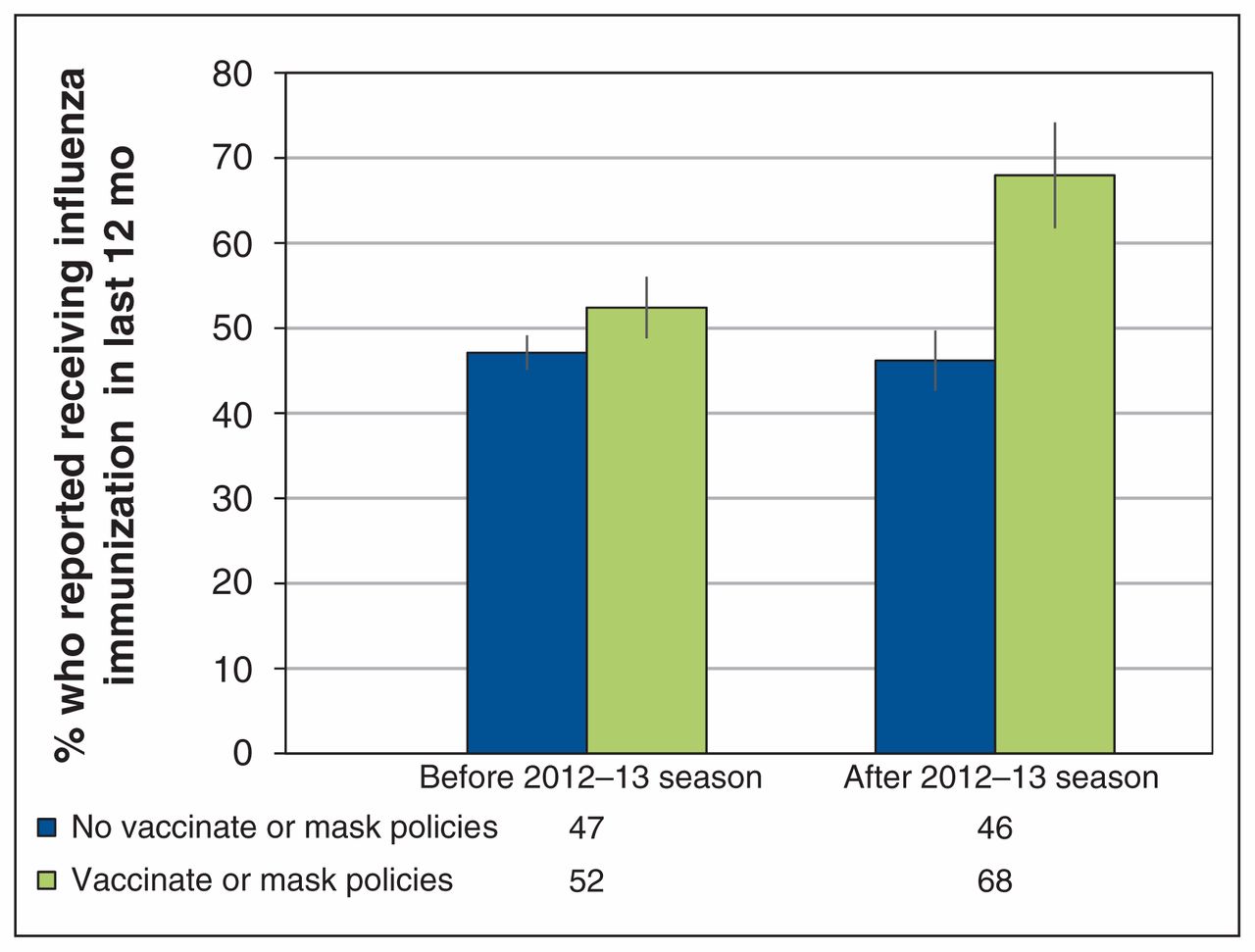
Health care personnel are more likely to be immunized against influenza than the general working population, but coverage remains suboptimal overall, say the authors of this national cross-sectional study. Data from the 2007 to 2014 cycles of the Canadian Community Health were pooled, and restricted to respondents who reported a health care occupation. For all survey cycles combined, about half of 18 446 health care personnel reported receiving seasonal influenza immunization during the previous 12 months, although this varied by occupation type (range 4%–72%). Compared with the general working population, family physicians and general practitioners were most likely to be immunized (prevalence ratio [PR] 3.15, 95% confidence interval [CI] 2.76–3.59), while chiropractors, midwives and practitioners of natural healing were least likely (PR 0.17, 95% CI 0.10–0.30). Among those who were not immunized, the most frequently cited reason was the belief that influenza immunization is unnecessary. Introduction of vaccinate-or-mask policies was associated with increased influenza immunization among health care personnel (Figure 1). CMAJ Open 2016;4:E479–88.
{kind=link}
Influenza immunization, by presence of vaccinate-or-mask influenza prevention policies for health care personnel (excluding Moncton Health Region and the province of Ontario).
Use of postoperative hospital services after bariatric surgery in Ontario or out of country
Before the Ontario Bariatric Network was established, Ontario residents could obtain permission to have bariatric surgery in the United States. However, there was minimal postoperative supervision for this group. This population-based study used administrative data to compare use of hospital services in Ontario within 1 year after surgery for Ontario residents who underwent bariatric surgery between 2007 and 2012 outside the country or at one of the Ontario Bariatric Network’s designated centres of excellence. Of the 10 031 patients included in the study, 4852 had bariatric surgery outside of Canada. After adjustment, surgery at a network centre was associated with a significantly lower utilization rate of postoperative hospital services than surgery performed out of country (rate ratio 0.90, 95% CI 0.84–0.97) (Table 1). There were no differences in mortality or time spent in critical care. However, physician assessment and reoperation rates were significantly higher among patients who received surgery at a network centre (rate ratio 4.10, 95% CI 3.69–4.56, and rate ratio 1.84, 95% CI 1.34–2.53, respectively). Implementation of a comprehensive and multidisciplinary bariatric program, with increased outpatient care, provided a better model of care than outsourcing surgery, resulting in reduced use of postoperative hospital services, say the authors. CMAJ Open 2016;4:E489–95.
Unadjusted and adjusted rate ratios comparing 1-year postoperative health services use and mortality among patients in the Ontario Bariatric Network and those who received bariatric surgery out of country