

A69-year-old man with insulin-treated type 2 diabetes was found unconscious two days after he had last been seen. His vital signs on arrival at the emergency department were normal.
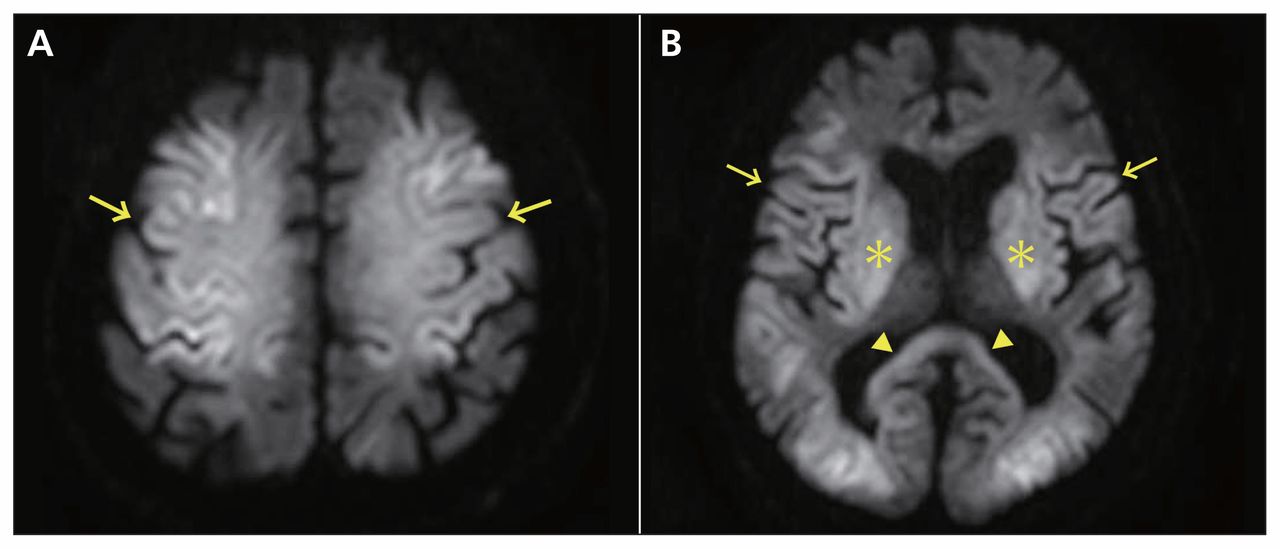
The patient was comatose, with a blood glucose level of 1.94 (normal 3.9–6.1) mmol/L. Arterial blood gas analysis showed no hypoxia. Computed tomography of the brain showed no abnormality. Cerebrospinal fluid analysis showed normal cell count and protein level. Cytologic and microbiologic investigations had negative results, as did investigations for other metabolic and toxic causes. Diffusion-weighted magnetic resonance imaging (MRI) showed extensive bilateral lesions in the cerebral cortex, basal ganglia and grey matter (Figure 1). We diagnosed hypoglycemic encephalopathy, likely from repeated episodes of hypoglycemia.
{kind=link}
Diffusion-weighted magnetic resonance imaging of the brain of a 69-year-old man with type 2 diabetes showing (A) increased signal intensity in the cerebral cortex (arrows) with relative sparing of the white matter; (B) hyperintensity in the cerebral cortex (arrows) and basal ganglia (asterisks), and slight hyperintensity in the splenium of the corpus callosum (arrowheads).
Cohort studies have suggested that as many as 15% of patients with insulin-treated type 2 diabetes have at least one episode of severe hypoglycemia.1 Although the prevalence is not known, hypoglycemic encephalopathy is a potentially life-threatening manifestation of hypoglycemia, which can present with seizures, altered mental status or focal neurologic deficits. Diffusion-weighted MRI of the brain shows symmetric hyperintense lesions in the cerebral cortex, hippocampus, internal capsule, amygdala or basal ganglia.2 Cortical lesions do not usually conform to a specific cerebral arterial distribution, suggesting a metabolic cause, and tend to involve the parieto-occipital area.2 Thalami are usually spared. The differential diagnosis includes hypoxic encephalopathy and an atypical posterior reversible encephalopathy syndrome. It is important to rule out metabolic and toxic causes before making the diagnosis. Case series have reported that diffuse and extensive lesions seen on MRI may predict poor neurologic outcomes.2,3
Our patient remained comatose during his stay in hospital, even after blood glucose levels returned to the normal range. He has remained in a coma for the past 15 months.
Acknowledgements
The authors thank Ms. Ryoko Ono for editing the images.
Footnotes
Competing interests: None declared.
This article has been peer reviewed.
The authors have obtained patient consent.