

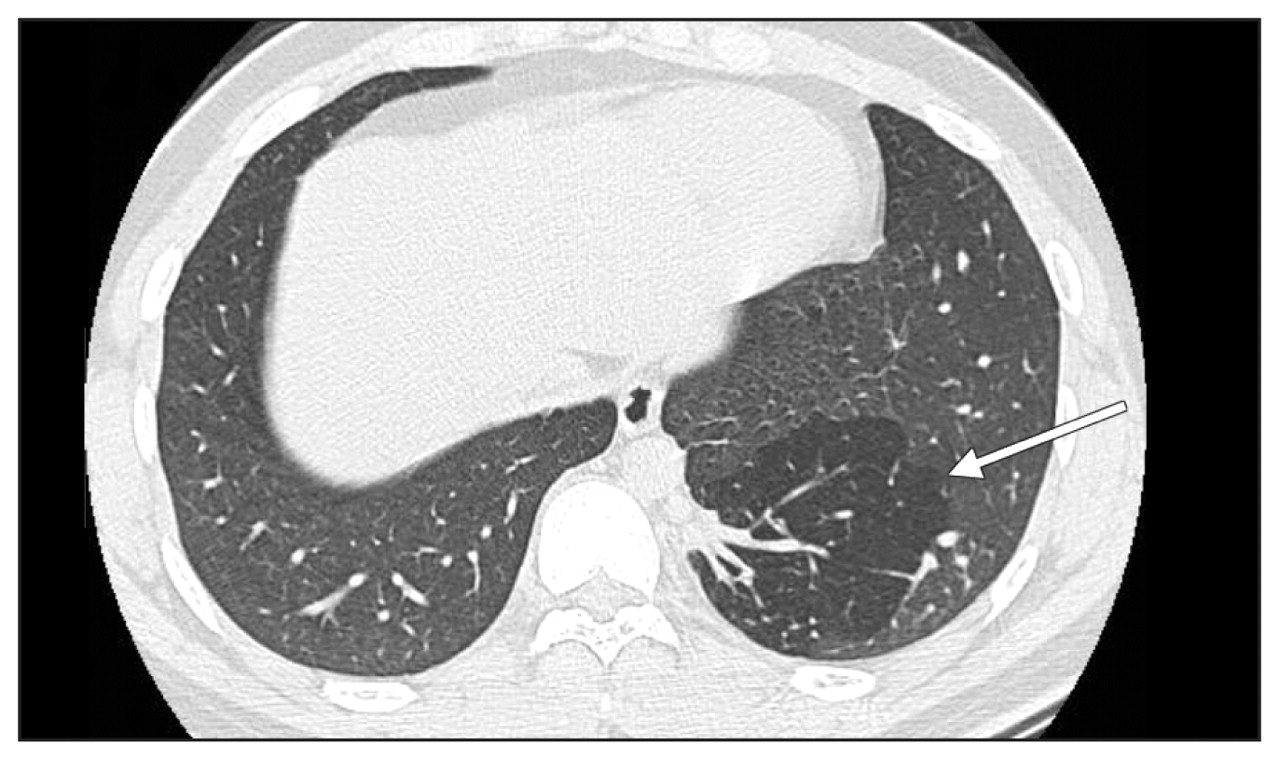
A 17-year-old boy was referred to our hospital because of repeated episodes of hemoptysis for several years. His physical examination was unremarkable. His blood cell count and coagulation profile were normal. Chest radiography (Appendix 1, available at www.cmaj.ca/cgi/content/full/cmaj.100203/DC1) and bronchoscopy showed no anomalies. Computed tomography (CT) of the chest showed a well-circumscribed hyperlucent area in the left basal lung (Figure 1) with a feeding artery from the aorta and venous return to the azygos vein (Appendix 2, available at www.cmaj.ca/cgi/content/full/cmaj.100203/DC1). The reconstructed CT image showed two feeding arteries from the aorta supplying the left basal lung (Figure 2).

Computed tomographic image of the chest in a 17-year-old boy with hemoptysis showing a well-circumscribed hyperlucent area (arrow) in the left basal lung.

{kind=link}
{kind=link}
Reconstructed computed tomographic image showing two feeding arteries (arrows) from the aorta.
Pulmonary sequestration, the second most common congenital lung anomaly after congenital cystic adenomatoid malformation, refers to a spectrum of abnormal connections of one or more of the four major components: airway, lung parenchyma, arterial supply and venous drainage.1 The estimated incidence in referral centres is 0.15%–1.8%.2 Pulmonary sequestration is divided into intralobar and extralobar types on the basis of the presence or absence of pleural covering.
Diagnosis requires a high index of suspicion when a child or young adult presents with recurrent lower lobe pneumonia, hemoptysis, shortness of breath or chest pain.2,3 The typical radiographic manifestation is focal opacification, especially on the left side. Rarely, a pulmonary sequestration appears as an area of hyper-radiolucency, as in our patient. This finding is called the “cystic form” of pulmonary sequestration, based on the radiographic appearance. Demonstration of systemic arterial supply, usually by contrast-enhanced CT, is the critical diagnostic feature for differentiation from other pulmonary parenchymal abnormalities.
Recurrent infection can occur in intralobar sequestration, and surgical resection is supported by case series and expert opinion.2 For asymptomatic lesions, however, there is considerable debate about resection. The prognosis in pulmonary sequestration is variable and depends on the presence of accompanying malformations and perioperative complications.
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.