

A 72-year-old woman with a history of hypertension presented with progressive swelling of the right posterior chest wall that had been present for two days following a diagnostic thoracentesis. She had developed progressive dyspnea two weeks before presentation, and had been assessed elsewhere. A chest radiograph taken at that time had shown a massive pleural effusion on the right, and a diagnostic thoracentesis had been performed under ultra-sonographic guidance with a 1.88-inch 18-gauge needle. The patient had noticed the swelling of her chest when she arrived home. She did not develop fever, chills, cough or worsening dyspnea following the procedure.
On examination, there was mild tenderness, but no redness, over a 10 × 12 cm area of swelling on the right posterior chest wall. A chest radiograph showed a right pleural effusion and severe swelling of the right chest wall (Figure 1). The patient’s white blood cell count and C-reactive protein level were normal. Computed tomography of the chest showed a mass in the right lower lung, along with swelling of the right chest wall with fluid accumulation that was consistent with a subcutaneous seroma (Figure 2). A pleural biopsy was performed and a small-bore catheter was inserted to drain the fluid. A total of 2.1 L of bloody fluid was drained.

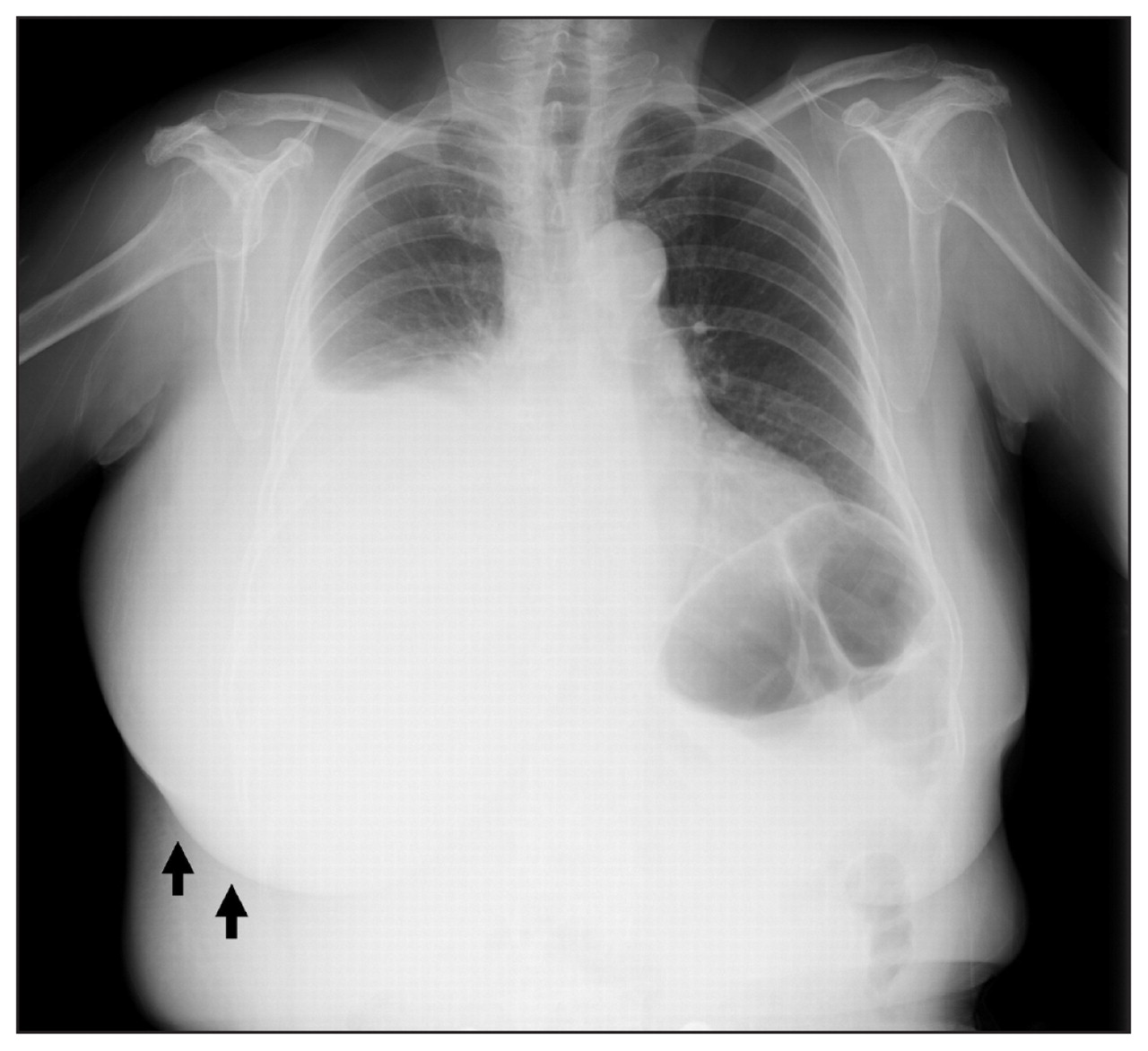
Chest radiograph of a woman showing a right pleural effusion and severe swelling over her right chest wall (arrows).

{kind=link}
{kind=link}
Computed tomographic scan of the chest showing swelling of the chest wall and fluid accumulation (arrows).
Adenocarcinoma of the lung was diagnosed from tissue biopsies taken during bronchoscopy; the pleural fluid was positive for malignancy. With daily application of a compressive dressing, the swelling of the right chest decreased. The patient was started on chemotherapy and the swelling resolved.
Thoracentesis is an invasive procedure involving removal of fluid from the pleural space for diagnostic or therapeutic purposes. Subcutaneous seroma is an uncommon complication of thoracentesis with an incidence of around 0.8%.1 The risk of subcutaneous seroma after thoracentesis is unknown, but the mechanism is thought to be extravasation of the pleural fluid under tension that occurs along the needle track to the subcutaneous tissue.1 Small seroma may resolve spontaneously in a few days,2 but experts suggest that larger seroma may benefit from a compressive dressing and insertion of a catheter for drainage.3
Footnotes
-
Competing interests: None declared.
-
This article has been peer reviewed.