

A previously healthy 54-year-old carpenter presented with a 13-day history of redness, tearing and pain in his left eye, which was associated with a progressive reduction in visual acuity. He had no fever or other systemic symptoms. He had no history of eye trauma or surgery, and he regularly used eye protection at work. He reported no intravenous drug use. He had immigrated to Canada from Vietnam 14 years before presentation, and his last trip to Vietnam was 7 months before the onset of illness. He initially sought medical attention 1 day after the onset of symptoms, and he was given gentamicin eyedrops for presumed conjunctivitis. After his symptoms did not improve, he was referred to an ophthalmologist.
On examination, his visual acuity was bare light perception in the left eye and 20/40 in the right eye. He had eyelid and conjunctival swelling in the left eye (Figure 1). No hypopyon was seen. Examination with a slit lamp showed corneal edema with 4+ leukocytes (greater than 50 cells visualized) and flare (reflection of light from protein in the aqueous humour) in the anterior chamber. Fibrin was also present in the anterior chamber. The fundus could not be seen. The results of an examination of the patient’s right eye were unremarkable. The patient did not have a fever, and the rest of a physical examination, including an abdominal exam, was unremarkable. A presumptive diagnosis of left endogenous endophthalmitis was made. A tap of the vitreous and anterior chamber of the patient’s left eye was performed, and 1.0 mg vancomycin and 2.25 mg ceftazidime were administered into the vitreous.

Figure 1: The patient’s affected eye at presentation.
Within 48 hours, Klebsiella pneumoniae grew in a culture from the vitreous. The patient was admitted to hospital, and infectious disease specialists were consulted. By this time, the patient had increasing eye pain and lid swelling. The results of a physical examination were otherwise unchanged. Laboratory data obtained on admission were within normal ranges, except for a leukocyte count of 15.5 (normal 4–11) × 109/L with 92% neutrophils. Liver function tests were not performed. Blood and urine cultures were negative. A computed tomography (CT) scan of the orbit of his left eye (Figure 2) showed periorbital swelling with marked proptosis.

Figure 2: A contrast-enhanced computed tomogram of the orbits showing left-sided proptosis, circumferential thickening of the scleral margin (arrow) and a crescent-shaped density in the anterior chamber.
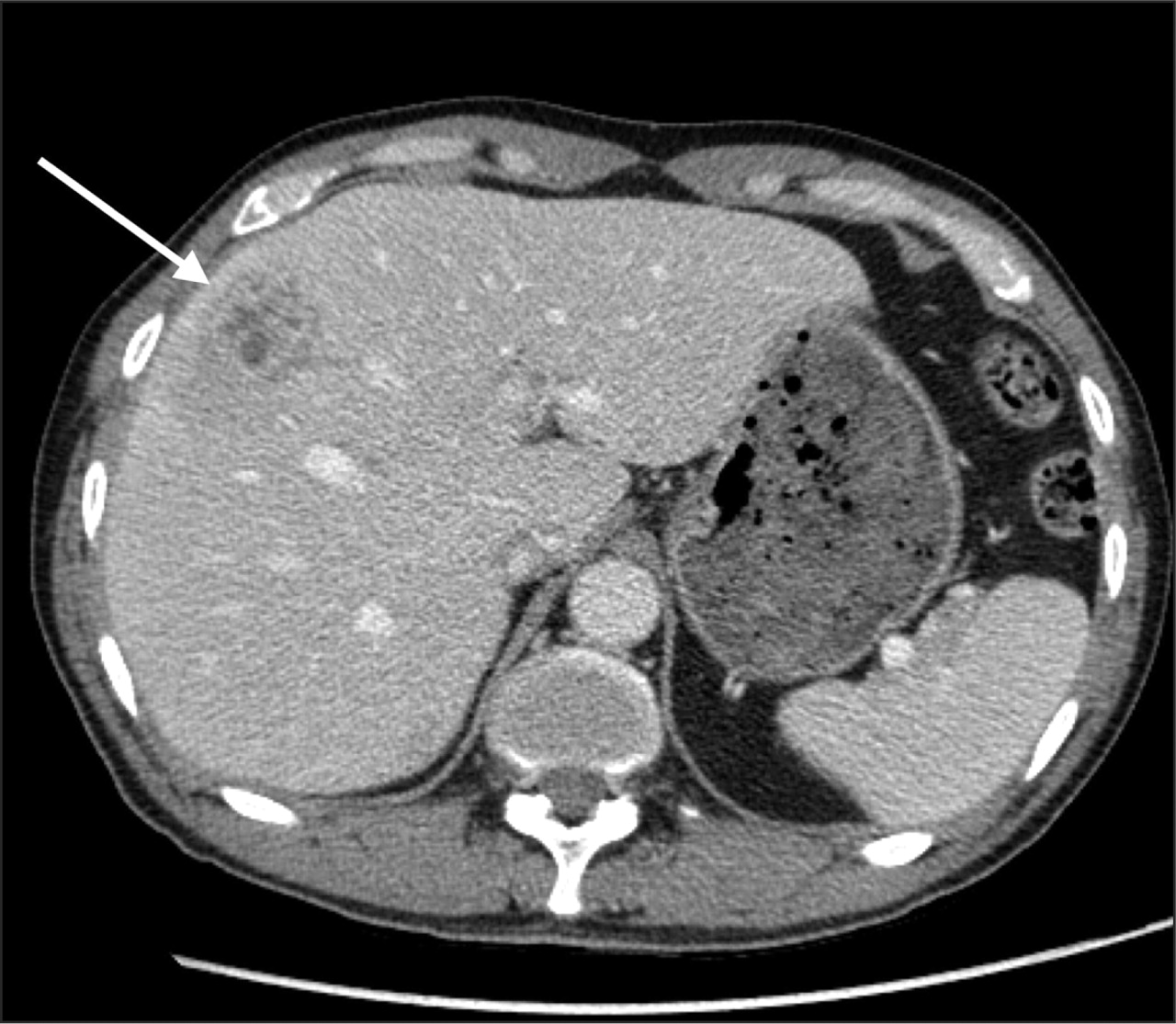
Given the potential association of K. pneumoniae liver abscess and K. pneumoniae endophthalmitis, a CT scan of the patient’s abdomen was performed, which showed a complex 4.7 × 2.7 cm hypodense mass with multiple septations in the right lobe of his liver (Figure 3). Ultrasound-guided percutaneous drainage of the mass was performed, and culture of the fluid yielded K. pneumoniae.

Figure 3: A computed tomogram of the patient’s abdomen with intravenous and oral contrast showing a 4.7 × 2.7 cm heterogeneous complex mass with irregular rim enhancement and multiple septations (arrow) in segment 5/8 of the liver.
The K. pneumoniae isolates were sensitive to all antimicrobials tested, and the patient was given intravenous ceftriaxone and topical ofloxacin. His eye pain and swelling resolved, but his vision did not recover. He was discharged home with oral levofloxacin for treatment of the liver abscess. On follow-up several months later, there was no evidence of progressive liver abscesses, but his vision had decreased to no light perception and he was experiencing eye pain. Ultra-sonography showed retinal detachment. Given the poor visual prognosis, he was ultimately referred for enucleation of the affected eye.
Discussion
Endogenous endophthalmitis is a vision-threatening infection of the vitreous cavity that presents with pain, decreased visual acuity and intraocular inflammation of the anterior and posterior segments. About 50%–80% of patients have fever or other systemic symptoms such as arthralgia, fatigue, anorexia, nausea and vomiting. 1,2 Liver abscesses, pneumonia, endocarditis and skin and soft tissue infections are the most common infectious foci associated with endogenous endophthalmitis, although any source of bacteremia or fungemia can cause endophthalmitis. 2 Unlike exogenous endophthalmitis, endogenous endophthalmitis is not associated with eye trauma, surgery or manipulation. 1,3
Liver abscess and endophthalmitis
Although the common causative agents of endogenous endophthalmitis in North America are Candida species and gram-positive organisms such as Staphylococcus aureus, K. pneumoniae has emerged over the last 20 years as the predominant pathogen in Southeast Asia, with the majority of early reports coming from Taiwan. The underlying source of the infection is a hepatic abscess in more than 50% of patients, and diabetes mellitus appears to be a predisposing factor in more than 75% of patients. 3,4 Metastatic complications, particularly endophthalmitis, are common. 4
The emergence of K. pneumoniae endophthalmitis probably reflects a changing epidemiology of liver abscess in Southeast Asia. However, it is not clear why K. pneumoniae liver abscesses have this ethnic and geographic distribution. Genetic susceptibility, socio-economic factors and geographic variance of specific K. pneumoniae serotypes may be contributing factors. Most cases of K. pneumoniae endophthalmitis and liver abscess appear to be caused by the K1 capsular serotype. A recently described virulence factor, the mucoviscosity associated gene A (magA), is associated with a hyper-mucoviscous phenotype that has decreased susceptibility to phagocytosis and may be partially responsible for the increased metastatic complications seen with some strains of K. pneumoniae. The magA gene is strongly associated with the K1 capsular serotype. 3,5
In the United States, recent reports of a similar clinical syndrome of K. pneumoniae liver abscess complicated by endophthalmitis may be related to immigration of individuals from endemic countries with potential redistribution of magA positive K1 K. pneumoniae strains into North America. Klebsiella pneumoniae is now the most common cause of liver abscess in the United States, overtaking Escherichia coli. 3,5
The association between K. pneumoniae hepatic abscess and diabetes may result from impaired phagocytosis and chemotaxis in patients with diabetes. A recent case–control study showed that the presence of a K. pneumoniae liver abscess, but not ethnic background or diabetes mellitus, is a risk factor for K. pneumoniae endophthalmitis. 6 However, it may be that diabetes and ethnic background predispose patients to K. pneumoniae liver abscess. Once an abscess is present, other bacterial or host factors may determine if metastatic infections such as endophthalmitis occur. 4
Despite the emergence of broad-spectrum antibiotic resistance in K. pneumoniae caused by the production of extended-spectrum β-lactamases or carbapenemases or both, almost all reported cases of monomicrobial K. pneumoniae liver abscess and endophthalmitis show minimal antibiotic resistance. 4,5
Urgent referral
Although this report focuses on endogenous endophthalmitis caused by K. pneumoniae, it also highlights the importance of obtaining an urgent ophthalmologic assessment for patients who present with eye redness, ocular pain and blurred vision. Many potentially vision-threatening diseases can present with these symptoms, including orbital cellulitis, acute angle closure glaucoma, neovascular glaucoma, episcleritis or scleritis, uveitis, corneal ulcers, abrasions and keratitis.
Early recognition of endophthalmitis requires that clinicians consider this diagnosis for patients who present with ocular symptoms and risk factors for exogenous or endogenous endophthalmitis (Box 1). This is especially important for patients who have undergone previous cataract surgery or trabeculectomy for glaucoma, the 2 most common causes of endophthalmitis. If acute endophthalmitis is suspected, urgent (i.e., < 24 hours) assessment by an ophthalmologist is required because visual loss can progress rapidly.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Box 1: Risk factors for endogenous and exogenous endophthalmitis
Endogenous endophthalmitis in a patient of Southeast Asian origin or who has recently travelled to Southeast Asia may be caused by K. pneumoniae. If the causative agent is confirmed, the endophthalmitis is most likely associated with an underlying hepatic abscess.
Guidelines for the diagnosis and management of endogenous endophthalmitis do not exist. We recommend, based on our interpretation of the literature, that all patients with endogenous endophthalmitis have a CT scan of the abdomen to exclude the presence of a hepatic abscess. All patients with monomicrobial liver abscesses caused by K. pneumoniae should be tested for diabetes, and clinicians should be aware of the potential for metastatic infection to occur, particularly endophthalmitis. 5 Prompt investigation and treatment should be initiated if any ocular symptoms develop. Although the visual prognosis with endogenous endophthalmitis caused by K. pneumoniae may be poor, early recognition and therapy represent the best opportunities to preserve vision.
This report provides an important reminder that diseases common on one continent can rapidly emerge on another. Given the large Southeast Asian population in urban areas of Canada, the impact of immigration from Southeast Asia and the associated personal and commercial travel between Asia and North America, the incidence of this disease will probably increase in both Canada and the United States.
-
Acute endophthalmitis should be considered in patients with blurred vision, ocular pain and redness, particularly in those with risk factors for endogenous or exogenous endophthalmitis.
-
It requires urgent referral to an ophthalmologist.
-
In a patient with endophthalmitis due to Klebsiella pneumoniae, the possibility of an associated liver abscess should be considered.
-
Metastatic complications are common in patients with K. pneumoniae liver abscesses and require careful clinical evaluation and urgent referral to an opthamologist if ocular symptoms develop.
Key points
Footnotes
-
Previously published at www.cmaj.ca
This article has been peer reviewed.
Competing interests: None declared.
Acknowledgment: We thank Dr. Tom Marotta for assistance in interpreting the radiographic findings.
The section Cases presents brief case reports that convey clear, practical lessons. Preference is given to common presentations of important rare conditions, and important unusual presentations of common problems. Articles start with a case presentation (500 words maximum), and a discussion of the underlying condition follows (1000 words maximum). Generally, up to 5 references are permitted and visual elements (e.g., tables of the differential diagnosis, clinical features or diagnostic approach) are encouraged. Written consent from patients for publication of their story is a necessity and should accompany submissions. See information for authors at www.cmaj.ca.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.