

- © 2008 Canadian Medical Association
At first glance, the Sabbatsbergs Närsjukhus Hospital in central Stockholm is indistinguishable from the medical centres that together form the front line of Sweden's vaunted health care system.
Its facilities, offering specialized services but no emergency room, are busy with patients who appear to be making use of a public hospital.
But looks can be deceiving. Once a government-managed facility, Sabbatsbergs today is — like nearly one quarter of primary care facilities in Sweden, and like nearly half in Stockholm — privately run, and has been since the mid-1990s.
This hospital, tucked amongst the low-rise heritage buildings of central Stockholm, is part of a growing trend in Sweden, where medical services are increasingly being provided by privately run, but publicly funded clinics in a country famous for its universal health care system.
And compared to the controversy surrounding private health care in other countries, in Sweden, of all places, the private sector has taken on a larger role with relatively little fanfare.
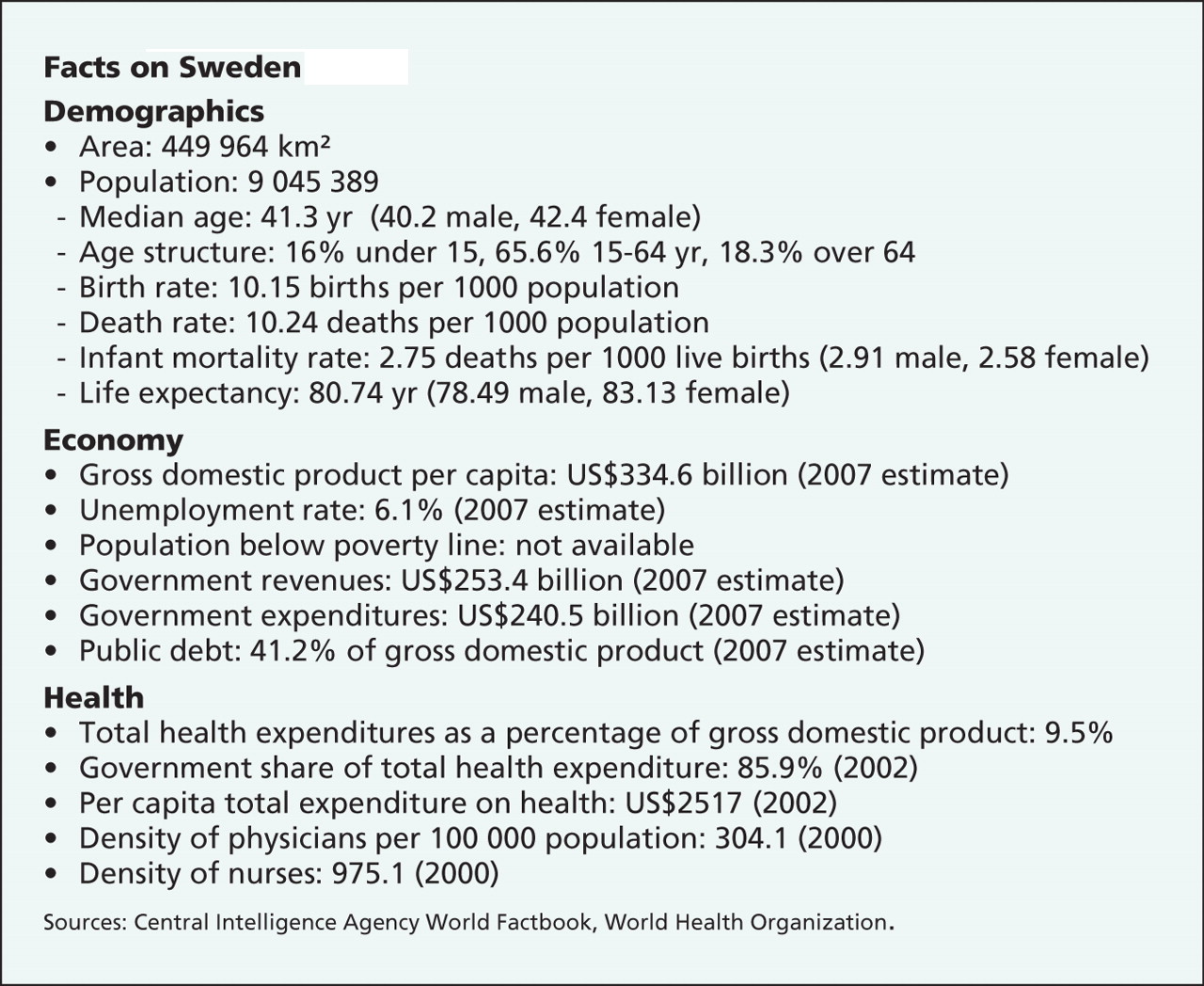
Facts on Sweden
For decades, Sweden has been the global bastion of socialized health care. In many ways, it still is. But as countries the world over struggle with rapidly changing technologies, spiking medical costs, rising demands for service with noncorresponding appetites for increased fees or taxation, Sweden is increasingly turning to the private sector to reduce the burden on a health care system at risk of being crushed under its own weight.
“Many of the developments in the last 15 years have been about going from a government-funded system to a more open system that includes the private sector,” says Dr. Birger Forsberg, a professor of international health at the Karolinksa Institute medical school who also advises Stockholm on health care policies.
The Scandanavian model of a welfare state built on high taxation is known the world over, especially in countries, like Canada, that have adopted various forms of the system.
In fact, Sweden's success at adopting a public–private hybrid was cited by the Supreme Court of Canada in its 2005 decision to strike down prohibitions against private health care insurance in Quebec, saying that countries such as Sweden and Germany, that allow private insurance, have successfully delivered medical services that are superior to and more affordable than services available in Canada.
About 18% of overall health spending in the country comes from the private sector, according to the World Health Organization. But on top of that, private companies compete alongside public facilities for government funding and the right to provide health care to Swedish citizens.
The winning bid — whether public or private — receives government funding with the goal of leaving the end service (in other words, what the patient sees) unchanged, regardless of the service provider, while rewarding those who can provide the quickest and cheapest treatment.

Sweden is almost as famous for its universal health care system as its artifacts, like this Viking helmet displayed at the National Historical Museum. Now, it's becoming renowned for the extent of private involvement in the publicly funded system. Image by: Photos.com
According to the most recently available survey, 250 such privately run but publicly funded clinics operate in the country, representing 24% of the country's health centres. That's up from 146 private clinics representing 14% of overall health centres in 2000, according to Sweden's Association of Private Care Providers.
In addition, the country has 9 fully private, fee-for-service hospitals that operate parallel to the public system.
Sweden is perhaps an unexpected place to find such a mix of public and private health care. But experts here say the country has been forced well past the point of debating the merits and risks of incorporating private health care because Sweden faces such extreme accessibility problems and a rapidly aging population.
“Today the discussion is not whether private health care should have a role in the system, but rather what role private health care will have,” says Klas Öberg, of Sweden's National Board of Health and Welfare. The board studies health care services in each of Sweden's 21 county councils responsible for delivering health care and advises the federal government on policy changes and developing trends.

{kind=link}
{kind=link}
{kind=link}
Nearly one-half of primary care facilities in Stockholm are now privately run, an almost-shocking statistic for a city and a country that has been the archetype for a welfare state built on high taxes. Located on Sweden's east coast, the central parts of Stockholm consist of 14 islands. The geographical centre of the city is essentially located on water, in the Bay of Riddarfjärden. Image by: Andrej Kropotov/iStockphoto.com
Accessibility issues have been at the core of many health care policy shifts in Sweden of late. Therefore, recent changes like a policy to allow patients to seek care from physicians anywhere rather than being tied to one doctor are geared more toward reducing wait times than reducing costs.
Earlier this year, the National Board of Health and Welfare found that nearly 45% of patients have longer wait times than are supposedly guaranteed by the health care system. This, despite a recent influx of 250 million Swedish kronor ($42 million) into reducing wait times.
“These figures are not satisfactory,” Swedish Health Minister Göran Hägglund, said in February when the findings were released. “They show that we haven't approached the problem of availability with the level of force needed. … The wait to receive attention — be it a telephone call to a local clinic or a first visit to a physician — is simply too long.”
The accessibility problem highlighted by the health minister is not going to go away, with a growing demographic challenge similar to that emerging in many Western countries.
Besides a senior citizen population that has grown by more than 10 000 since 2000 (to more than 300 000 total), the Swedish Association of Local Authorities and Regions expects the country's overall population to grow by 870 000 before 2030, only 75 000 of whom they predict will be active in the workforce.
“We're facing a situation where fewer are paying for more services, and where expectations for welfare services continue to increase steadily,” says Anette Åkesson, a member of the Association's welfare financing committee.
Such growth stokes fears of what will happen to a system already overburdened by too many people seeking services from too few medical practitioners. In an attempt to address that influx, the system is turning increasingly to the private sector in the hope that the answer can be found among those with an eye for results, and the bottom line.
Compared to the sensitivity surrounding the public-versus-private health care debate in Canada, Sweden has thus far managed to introduce an increasingly hybrid system with relatively little controversy.
The differing tones of the debate between public and private — hot under the collar in Canada and shrugging shoulders in Sweden — is partly explained by the way in which the Swedish government has approached the issue. It has allowed the 9 private, fee-for-service hospitals to open for business, with little handwringing. But the largest role for private medicine is in the public sector, where the privately run facilities receive public funding to provide citizens much the same services they would at government hospitals.
Within that system, citizens in government-funded clinics are charged user fees that account for about 5% of overall health funding, while the government contributes the rest.
Hospital stays cost about $13 a day. Patients are charged about $20 for each doctor visit, and about twice that to see specialists. But after $150 in 1 year, visits are free, and no citizen pays more than $300 per year including prescription drugs.
The country's drugstores are government-run, though the first private pharmacies are slated to open by January 2009.
Emergency services remain the domain of public hospitals, but as the tone of debate over public versus private health care in Sweden softens, there are fewer and fewer sectors of the system that are off-limits to private companies.
“What couldn't be said 20 years ago can be said today,” Forsberg says. “The ideology is not so important any more, it is just a matter of figuring out how to get the system to work.”