

- © 2007 Canadian Medical Association
What's your call?
Chest radiographs of a 76-year-old woman with previous tuberculosis, progressive dyspnea and peripheral edema.
A 76-year-old woman with a history of childhood tuberculosis was examined before admission to a tuberculosis sanatorium. Over the past 4–5 years, she had been experiencing peripheral edema and episodes of shortness of breath upon exertion. Her medical history included long-standing atrial fibrillation. Her family doctor had prescribed di-uretics, an angiotensin-converting enzyme inhibitor and a β-blocker.
Although she was normotensive upon examination, her neck veins were grossly distended and peripheral edema was obvious. Kussmaul's sign was present, and she had vague distant heart sounds and a distinct pericardial knock. Angiography showed that her coronary arteries were normal. Although her systolic function was also normal, she had an end-diastolic filling impairment consistent with constrictive pericarditis.
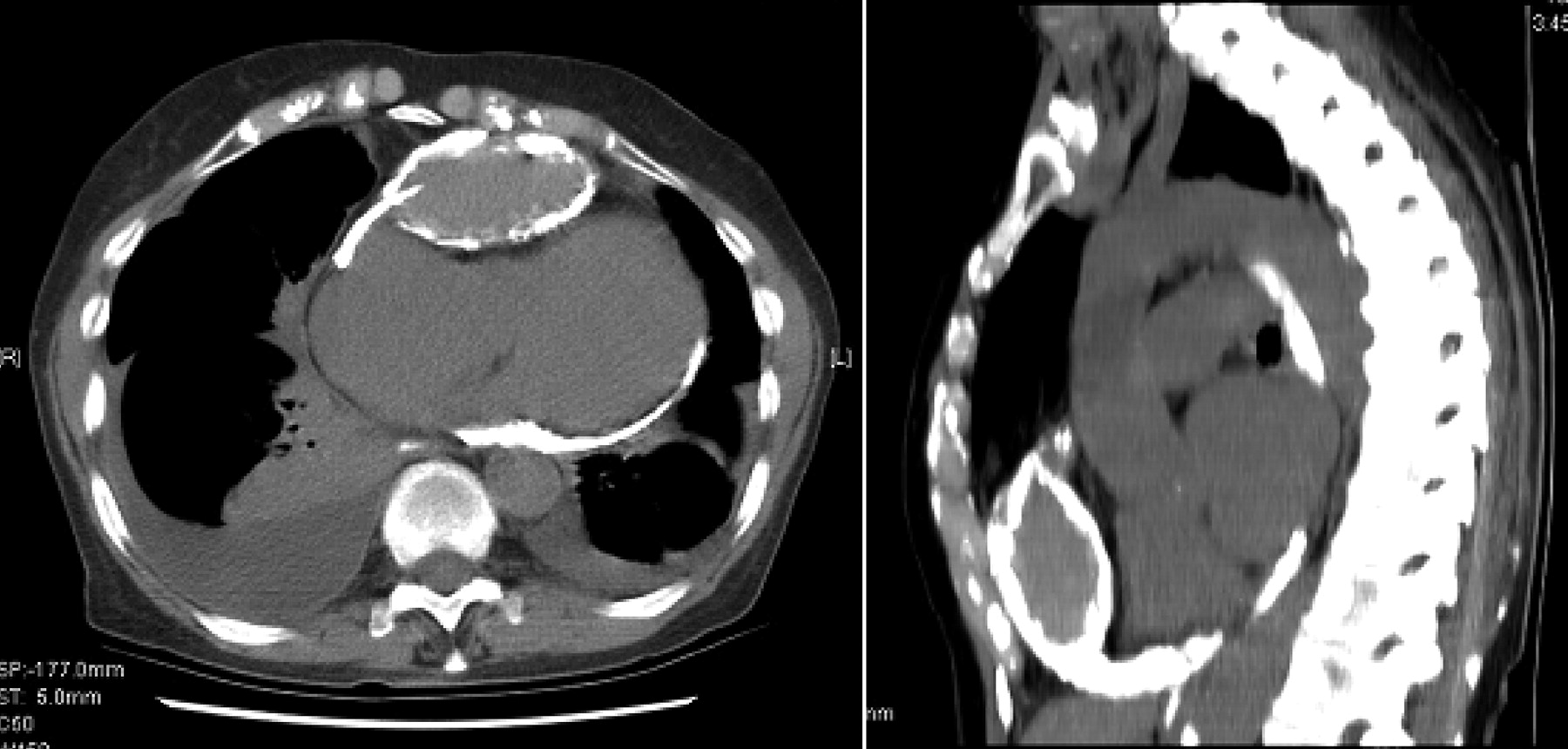
A CT scan revealed calcification on the undersurface of the heart, along its posterior and anterior aspects, and over the cardiac apex (Figure 1). On the anterior cardiac surface a lenticular cystic mass, 8 cm in its longest dimension, was visibly compressing the right ventricular outflow tract.
{kind=link}
Figure 1: A CT scan revealing a large, anterior calcified pericardial abscess and circumferential pericardial calcification.
During a median sternotomy, the cyst was explored in the anterior mediastinal area (Appendix 1; available online at www.cmaj.ca/cgi/content/full/177/2/148-b/DC1). The cyst contained a brown caseous liquid, which was evacuated. Radical pericardectomy without cardiopulmonary bypass was performed, with no intraoperative complications. The patient's postoperative course was uneventful. A specialist in infective diseases was consulted; since the resected tissue showed no active bacteria and the patient had no signs of active disease, no further interventions were suggested.
After discharge from hospital, the patient was no longer bothered by shortness of breath on exertion. At follow-up, she exhibited no physical signs of heart failure.
Constrictive pericarditis, often the result of fibrosis and calcification, can be a long-term consequence of pericarditis, either acute or chronic. Rigid, heavily fibrosed or even calcified pericardium restricts the myocardium and prevents adequate ventricular filling after an initial expansion. Tuberculous pericarditis, which occurs in 1%– 2% of cases of pulmonary tuberculosis, progresses to a constrictive form even more rarely.1 Constrictive tubercular pericarditis commonly arises via extension from pulmonary disease; however, miliary spread to the pericardium can also occur.
Although this patient's symptoms arose because of untreated pulmonary tuberculosis, constrictive calcific pericarditis can result from many processes, including chest trauma, the aftereffects of radiation, connective tissue diseases (e.g., lupus, rheumatoid arthritis) and infections (e.g., tuberculosis, histoplasmosis). In 30% of cases, a cause is not identified.2 Most patients with constrictive pericarditis arrive with signs of heart failure, including dyspnea and peripheral edema. The treatment of choice in symptomatic patients is pericardectomy.
Footnotes
-
This article has been peer reviewed.
Competing interests: None declared.
REFERENCES
- 1.
- 2.