

- © 2007 Canadian Medical Association
A 50-year-old woman arrived with progressive neck pain and stiffness, 3 years after a whiplash injury sustained in a motor vehicle crash. Previous diagnoses included cervical spondylosis and muscle imbalance; treatment with analgesics had proven unsatisfactory.
A physical examination revealed bilateral sternocleidomastoid wasting together with trapezius spasm (dystonia) and hypertrophy (Fig. 1). The patient had difficulty elevating and abducting her shoulders, and neck movements were restricted in all directions. Electromyography showed chronic sternocleidomastoid and upper trapezius reinnervation changes (reduced recruitment and increased duration of polyphasic motor units), with relative sparing of the other muscles innervated by cervical C5–C6 roots (the rhomboid major, deltoid and biceps). In addition, spontaneous motor-unit firing was observed in her upper trapezius muscles at rest. MRI revealed reversed cervical lordosis with no compression of the spinal cord.

Fig. 1: Lateral and anterior views showing the patient's severe hypertrophy of the right trapezius muscle (left panel), wasting of the sternocleidomastoid muscles, and bilateral dystonia and hypertrophy of the trapezius muscles (right panel).
The patient was treated with botulinum toxin injections to her trapezius muscles, which considerably reduced her pain and spasm. This clinical improvement lasted 3 months. Ongoing injections as required are planned.
Whiplash injury results from sudden acceleration or deceleration of the head and neck relative to other parts of the body, usually caused by motor vehicle crashes and sports mishaps.1 Excessive hyperextension or hyperflexion of the cervical spine can lead to many complications. Neck pain is a very common symptom; it results from injury to structures of the cervical spine, including the disc annulus, facet joint capsules, muscles, dorsal root ganglia and nerve roots.
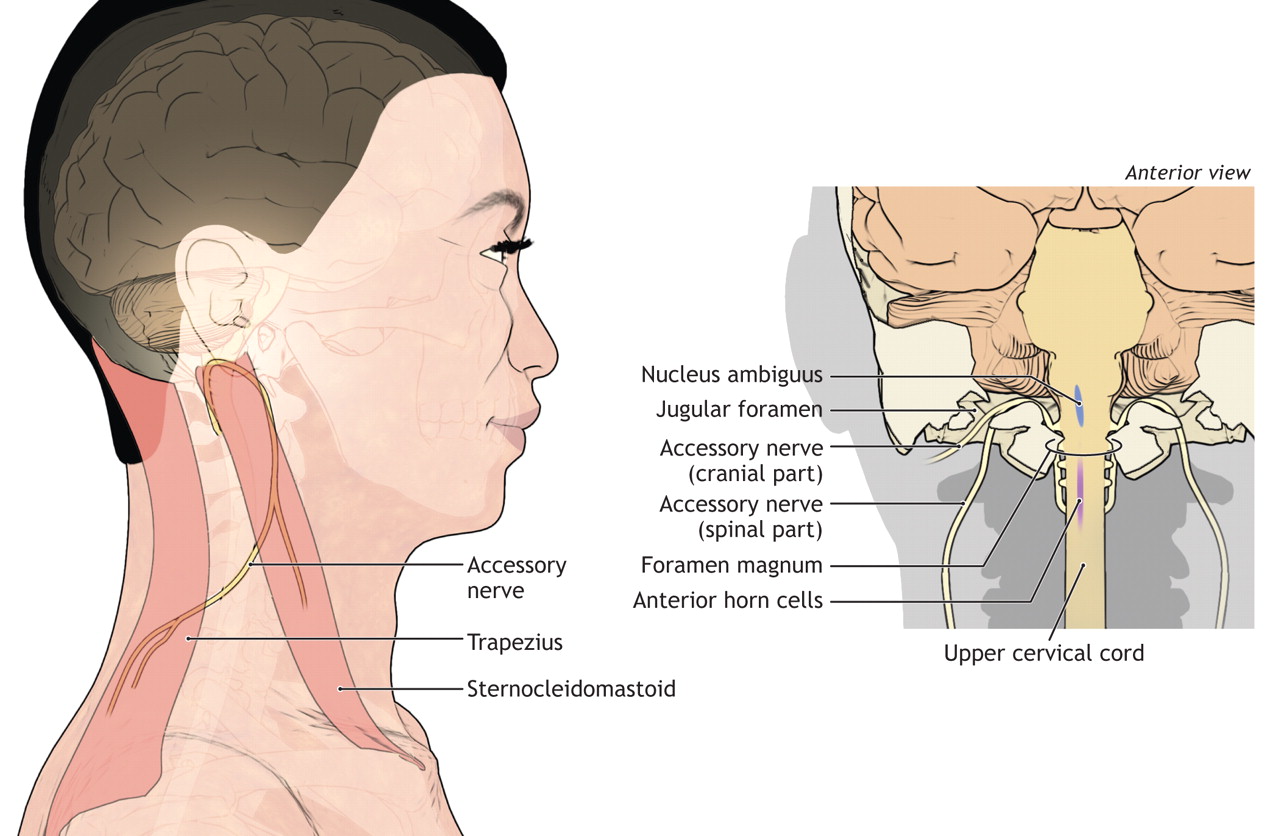
In our case, there was evidence of damage to the spinal component of the accessory nerve, which was suggested by the chronic reinnervation changes in the trapezius and sternocleidomastoid muscles, with relative sparing of those innervated by the C5–C6 roots and wasting of the sternocleidomastoids. The accessory nerve has cranial and spinal components (Fig. 2). The spinal component arises from the anterior horn cells of the first 5 cervical roots, traverses the foramen magnum and unites with the cranial portion. The nerve then innervates the sternocleidomastoid and trapezius muscles. Individual differences in trapezius innervation likely account for the variable clinical presentation of spinal accessory neuropathy.2

{kind=link}
{kind=link}
Fig. 2: The path of the (paired) spinal accessory nerve as it emerges from the foramen magnum, and (left panel) the muscles it innervates.. Photo by: Lianne Friesen and Nicholas Woolridge
Neurogenic muscle hypertrophy in association with spontaneous motor-unit discharges is rare but well documented.3 It has been described in patients with chronic radiculopathy and radiation injury.4 In our patient, the chronic basal motor-unit activity likely explains her excessive muscle spasm and trapezius hypertrophy.
Most reports of accessory nerve damage describe unilateral injury secondary to surgery, penetrating injuries, blunt trauma and mechanical stretching. Bejui and colleagues5 reported bilateral accessory nerve palsy sustained during a traffic accident in a 29-year-old man. The patient had bilateral wasting of the trapezius and right sternocleidomastoid. Over 3 years of follow-up, he showed partial recovery with conservative management.
These unique clinical images illustrate the coexistence of hypertrophy and atrophy of muscles associated with bilateral neuropathy of the spinal accessory nerves.
Footnotes
-
Competing interests: None declared.
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.