

- © 2005 Canadian Medical Association or its licensors
Contrary to popular belief, moving the nondominant side of the body is a bihemispheric event, with commands originating from the major hemisphere and effected by the minor hemisphere. In contrast, moving the dominant side of the body is a single hemispheric event.
According to the 1-way callosal traffic theory, motor signals that cross hemispheres through the corpus callosum do so exclusively from the major hemisphere to the minor hemisphere. Extraocular movements are governed by this same principle, which explains the eye deviations that can occur in the setting of acute stroke.1
Normal physiology
According to the 1-way callosal traffic theory, the decision to move the eyes begins in the major hemisphere. Therefore, in a person whose left brain is dominant (the case for most who are right-handed), the signal to move the eyes to the left originates in the left brain and travels across the corpus callosum to the right brain and onward to the pons. Here, the signal crosses to the nucleus of the sixth cranial nerve on the left side of the pons; the lateral rectus muscle is activated and the left eye is abducted. As the left eye moves to the left, it yokes the right eye to that side by activating the right medial rectus (Fig. 1).
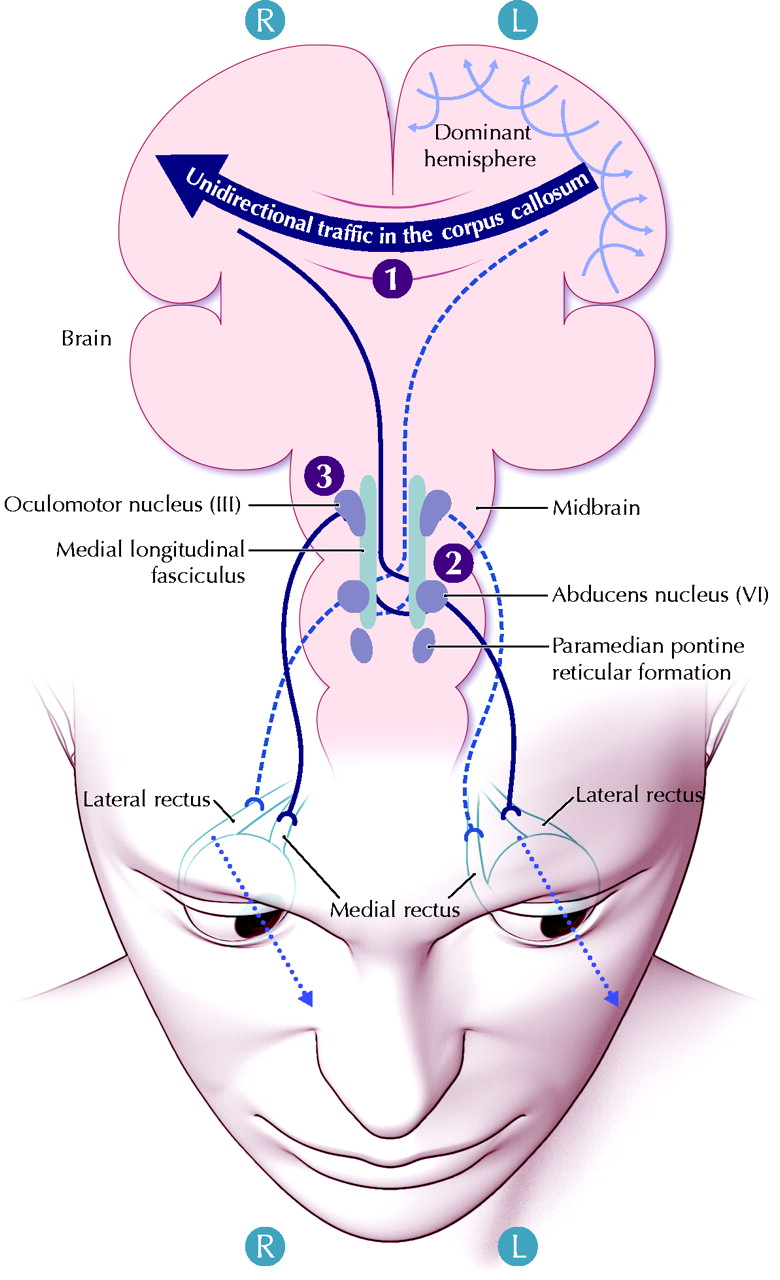
Fig. 1: Normal movement of the eyes to the left in a right-handed person. The signal to move the eyes originates in the dominant cortex (the left in most people) and is transmitted through the corpus callosum to the right motor cortex (1). The signal travels downward, crosses back to the left side to the abducens (sixth cranial nerve nucleus) (2) and then to the left lateral rectus. An impulse also reaches the third nucleus on the right side (3) through fibres in the medial longitudinal fasciculus and moves to the right medial rectus, pulling the right eye to the left. Stimuli also reach the left paramedian pontine reticular formation, causing inhibitory input to the left and right abducens to enable saccadic movement. See the animated figure at www.cmaj.ca/cgi/content/full/172/2/171/DC1. Photo: Lianne Friesen and Nicholas Woolridge
This yoking is accomplished not because a parallel signal is sent from the opposite motor cortex but because the right medial longitudinal fasciculus is activated by a signal from the left abducens. This signal crosses to the right side of the midline and ascends to the opposite third cranial nerve nucleus to yoke the right eye.
In order to abduct the left eye, the opposing action of the left medial rectus must simultaneously be inhibited. This is accomplished by the paramedian pontine reticular formation, a group of inhibitory cells on each side of the brain that lies just anterior to the abducens at the sixth nucleus; signals from here are projected across the midline to the opposite abducens nucleus to inhibit the right lateral rectus muscles (Fig. 1).
Conjugate eye deviation
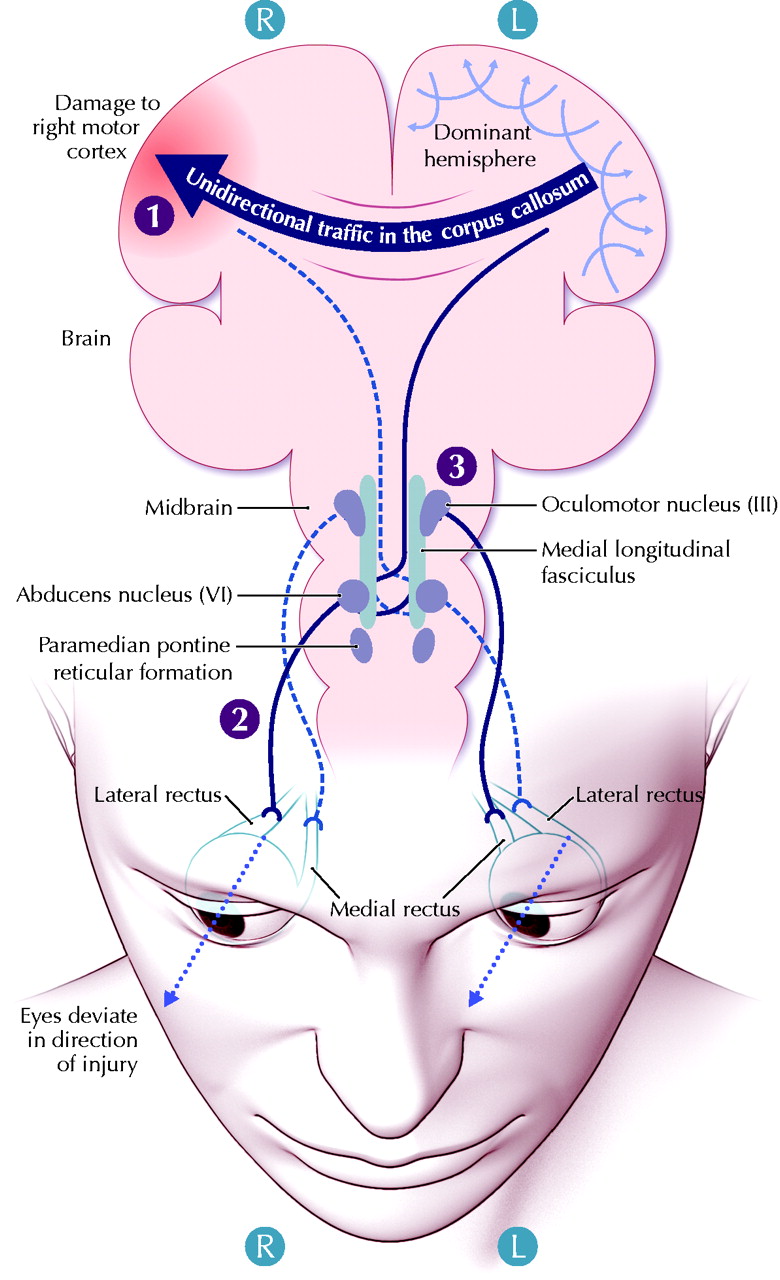
A classic clinical finding in a middle cerebral artery stroke is conjugate deviation of the eyes to the side of the lesion.2,3,4 In the case of a right-sided stroke in a patient with a left-dominant brain, signals from the right brain to the left eye are disrupted, whereas signals from the left brain to the right eye continue to work (Fig. 2 and Fig. 3). The result is an imbalance in neural tone that causes the right eye (which remains functional) to move to the right at rest because of the absence of a counter pull to the left. The left eye follows in a yoking manner because the intrapontine neural connections to the left medial rectus muscle are intact. The result is conjugate eye deviation to the right (and temporary gaze palsy to the left). However, conjugate eye deviation is not always present, an anomaly that may be explained using the 1-way callosal traffic theory.

Fig. 3: Conjugate eye deviation resulting from a right-sided middle cerebral artery stroke in a right-handed person. The right motor cortex is damaged (1), and signals reaching it from the dominant hemisphere (the left) cannot descend to move the left eye. As well, the right eye cannot follow the left in a yoking manner because of the nonfunctioning medial longitudinal fasciculus and the resulting diaschisis of the right third cranial nerve nucleus. The right eye, however, whose direct motor connections with the left cortex are in this context unaffected, deviates to the right “involuntarily” (2) as a result of the imbalance created by the lesion in the right hemisphere. The left eye follows in a yoking manner, using connections in the paramedian pontine reticular formation and medial longitudinal bundle (3). See the animated figure at www.cmaj.ca/cgi/content/full/172/2/171/DC1. Photo: Lianne Friesen and Nicholas Woolridge

Fig. 2: CT scan showing conjugate eye deviation to the right. The patient was right-handed. A second CT scan performed 20 hours after symptom onset confirmed a right frontal infarct in the right middle cerebral artery territory. Photo: Courtesy of Dr. Rob Sevick
Should a left-sided middle cerebral artery stroke occur in a left-dominant brain, the patient is usually unable to voluntarily look left or right, since both hemispheres are affected. Thus, eye deviations at rest are less predictable and less helpful in localizing the lesion for clinical purposes. According to the 1-way callosal theory, the patient is unable to look to the left because the left cortex does not transmit the original command to the left eye through the corpus callosum and right hemisphere.1,4
There is good evidence for this theory. For example, in a left-dominant brain, we know that the time it takes to abduct the right eye is less than the time it takes to abduct the left by a margin commensurate to the interhemispheric transfer time (the time it takes for a signal from the command centre on the left to reach the right hemisphere).1 Furthermore, in a series of cases described by Simon and colleagues2,3 81% (29/36) of patients with right-sided strokes had eye deviation to the right, whereas only 59% (42/71) patients with a left-sided stroke had eye deviation to the left. (In the remaining cases the eyes were not deviated, deviation was indeterminant [30], or the eyes were deviated in the opposite direction [6], appearing to look “away” from the lesion.) Finally, there is overwhelming evidence that excitatory signals governing motor commands originate in the dominant cortex.1
Lone abducting eye
In their case series, Simon and colleagues found that some patients with a right cerebral infarct had a “lone abducting eye” on the same side as the lesion.3 The right eye deviated to the right (as we would have predicted), but the left eye remained in the midline, giving the appearance of internuclear ophthalmoplegia. The authors defined this hitherto undescribed cortical sign “as a single appreciably abducting eye, with the other eye undeviated.”3
One of the patients was a right-handed person who experienced a right-sided stroke, which affected motor control of the left side of the body (Fig. 4). How can we explain the eye positions? A right-sided lesion results in an inability of the left eye to move in any direction. In this case, the left eye stayed in the midline, which reflects a total gaze palsy of the eye caused by diaschisis involving the pontine nuclear structure. The right eye looked to the right because there was no counter pull to the left. Furthermore, the right eye was unable to yoke with the left because of dysfunction in the right medial longitudinal bundle. In the setting of a right cortical lesion, diaschitic paralysis must also be responsible for this finding.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fig. 4: Lone abducting eye. The right eye, whose motor connection with the left cortex remains intact, has been pulled to the right as a result of the imbalance created by the right-sided stroke (1). The fibres going from the left cortex to the right lateral rectus (2) find their way directly, without callosal participation, to brainstem nuclei on the right. The left eye, which would normally follow the right in such a case, becomes immobile because of the diaschisis in the pons (3), which results from the acute cortical lesion on the right. The syndrome indicates a wider diaschitic paralysis of the left brainstem than in conjugate eye deviation. See the animated figure at www.cmaj.ca/cgi/content/full/172/2/171/DC1. Photo: Lianne Friesen and Nicholas Woolridge
Summary
According to the 1-way callosal traffic theory, there is directionality in callosal traffic that is coded by handedness: motor signals travel strictly from the left to right in right-handed people and from the right to the left in neural left-handed people, using the anterior part of the callosum. Thus, the left eye, like all effectors on or toward the left side, is entirely controlled by the right hemisphere, with ultimate control remaining in the major hemisphere.
Footnotes
-
No less than 15% of the public display a behavioural handedness opposite to that for which they are wired. This explains, for example, crossed aphasia (aphasia after right-brain damage) and crossed nonaphasia (left-brain damage that occurs without aphasia but with visuospatial and other deficits typical of right-brain damage).1
Diaschisis is a loss of electrical activity and function as a result of a cortical lesion in an area distant from the lesion but neuronally connected to it.
See the animated figures on www.cmaj.ca/cgi/content/full/172/2/171/DC1.
References
- 1.
- 2.
- 3.
- 4.